


Abstract
Background Point-of-care C-reactive protein (POCCRP) is a biomarker of inflammation that offers clinicians a rapid POC test to guide antibiotic prescribing decisions for acute cough and lower respiratory tract infections (LRTI). However, evidence that POCCRP is cost-effective is limited, particularly outside experimental settings.
Aim To assess the cost-effectiveness of POCCRP as a diagnostic tool for acute cough and LRTI from the perspective of the health service.
Design and setting Observational study of the presentation, management, and outcomes of patients with acute cough and LRTI in primary care settings in Norway and Sweden.
Method Using hierarchical regression, data were analysed in terms of the effect on antibiotic use, cost, and patient outcomes (symptom severity after 7 and 14 days, time to recovery, and EQ-5D), while controlling for patient characteristics (self-reported symptom severity, comorbidities, and health-related quality of life) at first attendance.
Results POCCRP testing is associated with non-significant positive reductions in antibiotic prescribing (P = 0.078) and increased cost (P = 0.092). Despite the uncertainty, POCCRP testing is also associated with a cost per quality-adjusted life year (QALY) gain of €9391. At a willingness-to-pay threshold of €30 000 per QALY gained, there is a 70% probability of CRP being cost-effective.
Conclusion POCCRP testing is likely to provide a cost-effective diagnostic intervention both in terms of reducing antibiotic prescribing and in terms of QALYs gained.
INTRODUCTION
A major challenge in managing patients with acute cough and lower respiratory tract infections (LRTI) is determining which patients will benefit from antibiotic treatment. It is often not feasible for clinicians to order microbiological and/or other investigations for all patients with symptoms of acute respiratory infections. Instead, clinicians generally rely on the patient’s medical history and a basic physical examination.1 However, clinical assessment alone has poor predictive value.2–3 Consequently, antibiotics are often prescribed to those who are unlikely to benefit, contributing to the development of antimicrobial resistance.4–5
A rapid test, point-of-care C-reactive protein (POCCRP) is widely used in Scandinavia to guide antibiotic management for acute cough and LRTI.6–7 Near-patient testing provides results in minutes and so guides antibiotic treatment decisions at the initial consultation.8 Although CRP level in patients with LRTI appear to strongly influence the likelihood of antibiotic prescribing,7 there remains mixed evidence about the diagnostic value of CRP in distinguishing bacterial from viral infection (aetiology), and its prognostic value in indicating potential benefit from antibiotics.9–14 More evidence is needed about whether CRP is an effective diagnostic and prognostic tool in primary care.
The impact of POCCRP on antibiotic prescribing and patient outcomes has been assessed in clinical settings, showing that antibiotic prescribing in patients managed with POCCRP testing was lower than the control group,6 and that POCCRP did not compromise patient recovery. However, the study did not consider multiple outcomes and was limited to one country (the Netherlands); it is unclear whether results are generalisable to other high income countries.
The aims of the work reported here were: first, to evaluate the impact of POCCRP testing in two European countries (Sweden and Norway) on antibiotic prescribing; secondly, to confirm that it did not compromise patient recovery; and thirdly to assess the cost-effectiveness of the test for diagnosing LRTI from a health service perspective. Each is important in the essential purpose of POCCRP, to reduce antimicrobial resistance through improving antibiotic prescribing decisions.
How this fits in
This study is the first to assess the cost-effectiveness of point of care C-reactive protein (POCCRP) in a pragmatic clinical setting using an observational design. The results of this study indicate that POCCRP is a cost-effective tool to aid antibiotic prescribing decisions for acute cough and lower respiratory tract infections.
METHOD
Patients and settings
This analysis was conducted as part of the Genomics to combat Resistance against Antibiotics in Community-acquired LRTI in Europe (GRACE) observational study, conducted in 14 primary care networks in 13 countries. This study recruited consenting patients aged ≥18 years presenting to their GP for the first time with an acute or worsened cough as the main or dominant symptom for up to 28 days, or who had a clinical presentation suggesting LRTI. Consecutive eligible patients were recruited, and followed-up for 28 days. Full details of study design and clinical outcomes are reported elsewhere.15 For this analysis, data were included from two countries (Sweden and Norway) where primary care clinicians use POCCRP testing routinely in treating LRTI.
Data collection
Resource use
Healthcare resource use by patients was recorded from two sources. First, patients provided resource-use information on a weekly basis in diary format, for each week over a 4-week period, including information about primary care clinic visits, nurse visits, and hospital admissions. Secondly, after the initial clinic visit, clinicians completed a case report form containing information about medical investigations, referrals, antibiotics, and other drug prescriptions.
Healthcare unit cost
Country-specific unit cost data were obtained from four sources: (i) national and international publications on costs; (ii) collaborators from the GRACE network; (iii) British health economists who had participated in studies in the countries; and (iv) health economists in the countries. Over-the-counter medication was classified into eight groups and costs generated for each group by estimating an average price from a list of drugs in that group. Costs in all countries were converted to Euros (€) using purchasing power parities (PPPs) and 2007 prices. Full details are presented elsewhere.16 The cost of a POCCRP test was estimated to be €6.20 in Sweden and € 4.10 in Norway.
Health outcomes
Health outcome data were collected from the following:
EQ-5D questionnaires: patients completed the EQ-5D questionnaire on the day of their initial primary care attendance, and then weekly until the end of the 4 weeks. EQ-5D comprises five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each with three levels (no problems, some problems, and severe problems).17 The European harmonised value set18 was used to value the EQ-5D data.
Symptom diaries: Patients provided information about symptoms on a daily basis over a 4-week period using a validated measure presented in a diary.19 Symptoms included were cough, phlegm production, shortness of breath, wheezing, blocked nose, chest pain, fever, muscle ache, headache, disturbed sleep, feeling unwell, interference with normal activities, and interference with social activities. Each symptom was scored on a scale of 0–6, where 0 indicated the symptom was absent and 6 indicated the highest level of severity. A composite score ranging between 0 and 100 was generated.15 Patients were deemed to have recovered when their composite score fell to 0. Patients were also asked to indicate the day on which they felt well.
Case report forms. Clinicians completed case report forms at the initial clinic visit. Symptom information, comorbidities, and findings from chest auscultations were collected.
Data analysis
The effect of POCCRP testing on patient outcomes and antibiotic prescribing was investigated. First, patient characteristics at first clinic visit (age, length of illness prior to consulting, EQ-5D score, composite patient-reported severity scores, comorbidities, findings from chest auscultations, and symptoms) between patients receiving and not receiving POCCRP were compared, to determine whether POCCRP tests were more likely to be given to a particular profile of patients. Secondly, the relationship between receiving POCCRP and outcomes was explored, using hierarchical regression to control for the effect of patient characteristics at first clinic visit (with explanatory variables stratified into patient and practice levels). Outcomes considered were antibiotic prescribing, EQ-5D scores on days 7 and 14, composite severity scores on days 7 and 14, days to recovery based on having no reported symptoms and patient-reported days to recovery. Using the area under the curve approach, quality-adjusted life years (QALYs) were estimated from EQ-5D scores. QALYs provide a measure of benefit that combines quality and quantity of life; they are often used in healthcare decision making.20 A net monetary benefit value17 was estimated for each patient using the formula (threshold x QALY) – total cost. This was included as a dependent variable in the model. The primary explanatory variable was whether or not POCCRP testing was administered. However, baseline EQ-5D scores, baseline composite severity score, patient comorbidities, symptoms at baseline, findings from chest auscultations ,and country were also included as covariables.
Model estimates of the difference in healthcare costs and the probability of being prescribed antibiotics between patients receiving and not receiving POCCRP were compared. This was used to estimate cost-per-patient reduction in prescribed antibiotics and cost per QALY gained. Incremental net benefits were also obtained. A cost-effectiveness acceptability curve (CEAC) showing the probability that POCCRP is cost-effective across a range of values that a decision maker is willing to pay for an additional QALY was constructed following the method of Hoch and colleagues.21–22 All analysis was carried out in Stata (version 12) and Microsoft® Excel®.
In Norway and Sweden, there is no explicit threshold at which an intervention is considered cost-effective. Thus, a threshold value of €30 000 per QALY gained was assumed.
RESULTS
Patient characteristics
The study population included 370 patients of whom 32% were male and 68% female. Patients ranged in age from 18 to 86 years. All patients consulted with cough, 314 (84.9%) with phlegm and 321 (86.8%) felt generally unwell. There was a higher rate of CRP testing by clinicians in Norway (Table 1). Diaries were completed by all 370 patients that were included in this study.
Number of LRTI consultations where CRP tests are administered, by country
Association between patient characteristics at first visit and CRP use
Patients receiving POCCRP tests presented to their GP with more comorbidities than those not administered the test (P<0.01). There was no significant difference in EQ-5D scores, and severity scores between the two groups at the initial clinic visit (Table 2).
Patient characteristics at first clinic visit
Resource use
Having POCCRP was significantly associated with undergoing more medical investigations and fewer hospital admissions (P<0.01). After controlling for patient characteristics, the POCCRP group was still associated with having more medical investigations and fewer hospital admissions (P = 0.03). All other resource use items were not significantly associated with POCCRP at the 5% significance level (Table 3).
Relationship between administration of CRP test patient outcomes and resource use
Costs
Patients receiving POCCRP tests had greater mean healthcare costs compared to patients who did not, but this difference was not statistically significant either before adjustment or after using hierarchical regression to account for patient characteristics at first visit (Table 3).
Patient outcomes
Patients receiving POCCRP did not have significantly different measures of recovery or outcomes compared to patients not receiving this test (Table 3).
Antibiotic prescribing
Antibiotic prescribing was lower in the POCCRP group but this relationship was not statistically significant at the 5% level either before adjustment or after patient characteristics at first clinic visit were taken into account ( P = 0.08; Table 3).
Cost-effectiveness
Once patient characteristics at first clinic visit are accounted for, the regression model predicts that use of POCCRP increases healthcare costs by €11.27 ( P = 0.09) and reduces the probability of antibiotic prescribing by 10% ( P = 0.08) per patient. This suggests that an additional cost per patient prescription avoided as a result of POCCRP is €112.70. POCCRP is also associated with a cost per QALY gain of €9391. At €30 000 per QALY, the incremental net monetary benefit was €25.20. Figure 1 shows the incremental net monetary benefit at different willingness-to-pay thresholds. At a willingness-to-pay threshold of €30 000 per QALY, the probability of POCCRP being cost-effective is approximately 70% (Figure 2).
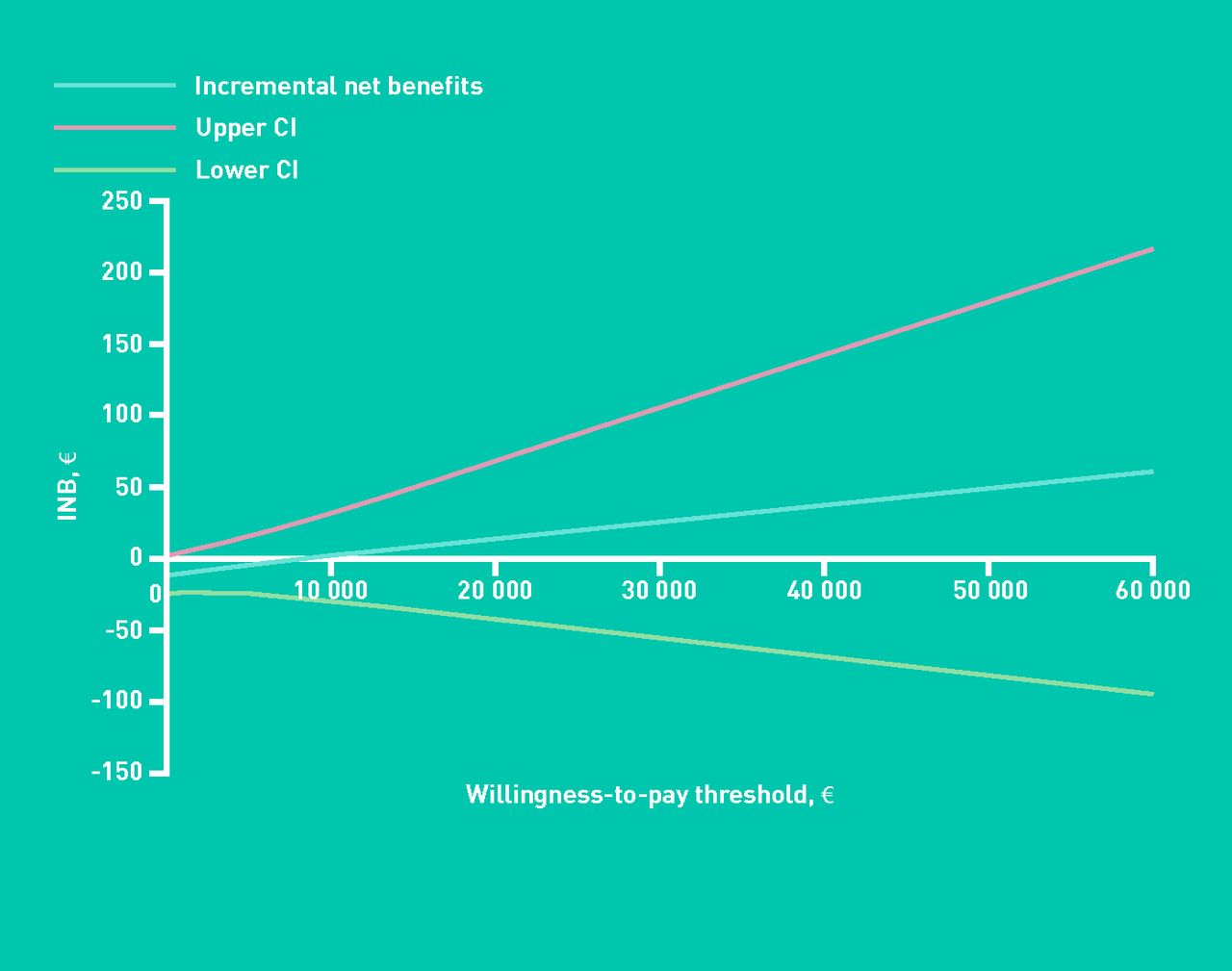
Incremental net benefits (INB) of CRP versus no CRP (95% CI).

{kind=link}
{kind=link}
Cost-effectiveness acceptability curve. CRP = C-reactive protein.
DISCUSSION
Summary
In this observational study, perhaps unsurprisingly, POCCRP tests were more likely to be administered to patients with more comorbidities. This reflects use of POCCRP in a pragmatic clinical, as opposed to an experimental setting. The study also suggests that patients with acute cough and LRTI administered POCCRP tests in primary care have higher healthcare costs, worse outcomes, and a lower probability of being prescribed antibiotics. These results were not statistically significant and, therefore, the intuition might be to conclude that POCCRP does not provide value for money. However, within the current paradigm an analyst faced with a study not powered for equivalence is advised to conduct a cost-effectiveness analysis in all cases because of the need to focus jointly on estimating costs and effects.23 The results indicates that POCCRP testing was associated with a reduction in antibiotic prescribing at the cost of €112.70 per patient prescription avoided and a cost per QALY gain of €9391.
Strengths and limitations
The observational nature of this study is both a limitation and strength. As patients were selected by their primary care clinicians to receive POCCRP tests (or not), rather than being randomly allocated to receive a test, patients with more severe illness were more likely to be tested. Therefore, multivariable regression was used to account for differences in outcomes due to cofactors. There is a possibility that not all cofactors are controlled for, and that there may still be a difference between the patient characteristics in the two groups as a result of this residual confounding. To minimise this possibility all relevant cofactors (26 variables) were included. In keeping with the study’s pragmatic aim of assessing usual care, clinicians were not directed how they should interpret POCCRP results; instead they were interpreted according to their usual practice. An article7 also using data from the GRACE observational study found for Sweden and Norway a CRP value <20 mg/L in 65% of those tested, with antibiotics being prescribed to 19% these. Among the 13% with a CRP value ≥50 mg/L, 88% were prescribed antibiotics, indicating that CRP level did influence prescribing
However, the strength of an observational study such as this is that it takes place under conditions that more closely approximate usual care; the findings are therefore likely to have greater applicability to primary care in ‘the real world’ than findings of experimental studies where use of POCCRP is carefully prescribed and delivered according to patient randomisation. This wider applicability is of particular importance when considering cost-effectiveness, where experimental studies sometimes bear little resemblance to provision in the actual health economy. A further strength is that the study shows what types of patients actually receive a POCCRP test in clinical practice, which is not revealed in randomised studies24 and which is relevant to resource allocation decisions. However, the study was limited to 4 weeks of follow-up. While not a problem for the analysis, any long-term issues such as change in practice over time associated with the use of POCCRP would not be detected.
Comparison with existing literature
Two studies have evaluated the cost-effectiveness of POCCRP in a trial setting.9,25 In both cases, POCCRP was cost-effective. The finding that POCCRP testing reduces the rate of antibiotic prescribing for LRTI in primary care is consistent with conclusions in a randomised study carried out in the Netherlands,6 which also concluded that POCCRP does not have any significant effect on outcomes, again consistent with the results found here.
Implications for research and practice
The results from this study provide useful information to decision makers. In the short term, they suggest that POCCRP has no adverse influence on the health of patients, and may be associated with a reduction in the probability of prescribing, which would ultimately lead to societal health benefits in the long-run through helping to contain antibiotic resistance. The incremental cost of POCCRP testing per unit reduction in antibiotic prescribing is €112.70, and the incremental cost per QALY gained is €9391. However, there is no commonly accepted threshold at which achieving a particular quantum of antibiotic prescribing would be considered cost-effective. To determine whether POCCRP is a good use of healthcare resources, the societal benefit of reduced antibiotic use needs to be considered.26 Such benefit stems from its potential to contain antimicrobial resistance.27–30 Antibiotic resistance is generally low in Nordic countries in comparison to other parts of Europe.31 Prescribing in the Nordic countries is also lower than in most other parts of Europe. This could be partly as a result of high use of POCCRP tests in the Nordic countries. Other European countries could also see benefits from implementing POCCRP testing in primary care. However, to estimate the long-term effect of reduced antibiotic use on antibiotic resistance and the associated societal benefit, mathematical models of bacterial infection are required. Early models have produced interesting theoretical results,32 but studies such as this one are needed to parameterise them so that they can be used for policy making.
Although this article provides evidence of cost-effectiveness, there are also resource implications from widespread use of the test. It is difficult to predict the total size of these costs, although the relatively small cost of the test needs to be balanced against potential longer-term costs associated with increased resistance.
Acknowledgments
We thank the GRACE Clinical Platform, Mark Kelly and Samuel Coenen for their input into this study.
Notes
Funding
This study was funded as part of the GRACE (Genomics to combat resistance against antibiotics in community-acquired LRTI in Europe), a European Commission funded project within the Sixth Framework Programme, reference number LSHM-CT-2005-518226.
Ethical approval
This study was approved by the ethics review committees in all participating countries and written consent was obtained from all participants before their inclusion into the study.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received December 19, 2012.
- Revision received February 19, 2013.
- Accepted March 11, 2013.
- © British Journal of General Practice 2013
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

