


INTRODUCTION
Femoroacetabular impingement (FAI) is a pathological hip condition characterised by abnormal contact between the acetabulum and femoral head–neck junction.1 This can occur within the normal physiological range of motion as a result of osseous abnormalities described as either cam or pincer deformities. Cam deformities describe an abnormal anterosuperior femoral head–neck junction, whereas pincer deformities describe abnormalities in the shape or orientation of the acetabulum (Figure 1). Some patients have both deformities, designated mixed pathology.2 Impingement can also occur in a morphologically normal hip as a result of extreme range of motion activities, such as in ballet dancers or gymnasts.

Illustrative lateral view of a hip showing a) cam deformity with additional bone at the anterior femoral headneck junction (shown in red) b) normal hip c) pincer deformity with additional bone at the anterior acetabular rim (shown in red). The deformities in a) and c) cause the femoral neck to impact against the labrum and acetabular rim on flexion and internal rotation.
Repeated abutment of the femoral neck against the acetabular rim can result in injury to the labrum and adjacent cartilage.3 Over time these focal lesions may progress to more extensive degenerative disease. There is increasing evidence implicating FAI in the development of osteoarthritis (OA).1,4 In a large population study, cam and/or pincer deformities were found in 71% of males and 37% of females with hip OA.5 Recent longitudinal studies also support this association.6
PRESENTATION
FAI commonly presents in healthy, active adults, most frequently between the ages of 25 and 50 years. In older patients it is more frequently accompanied by OA.
Deep intermittent discomfort, during or after activity is the most common presenting complaint. The first step in assessment involves a comprehensive pain history. Intermittent discomfort in the groin during or after repetitive or persistent hip flexion is characteristic of anterior impingement resulting from either cam or pincer deformities. Sprinting or kicking sports, hill climbing or prolonged sitting in low chairs are common exacerbating activities. Pain may be referred to the anterior thigh, symphysis pubis, or the ipsilateral testicle in men.
Pincer deformities may also give rise to posterior impingement with pain experienced in the buttock or sacroiliac region and are often difficult to differentiate from pain referred from the low back or sacroiliac joint. Repeated hyperextension with such activities as fast-walking, or walking downhill are common exacerbating activities. Posterior hip pain during intercourse is also a frequent complaint in women.
Associated mechanical symptoms such as catching or clicking may be seen when labral tears are also present. Duration of symptoms is variable, and patients sometimes report an inciting event.
EXAMINATION
Antalgic or Trendelenberg-gait patterns may be observed.
Internal rotation with the hip at 90° of flexion is typically markedly limited. Flexion and abduction are also often limited, although this is a less consistent feature.
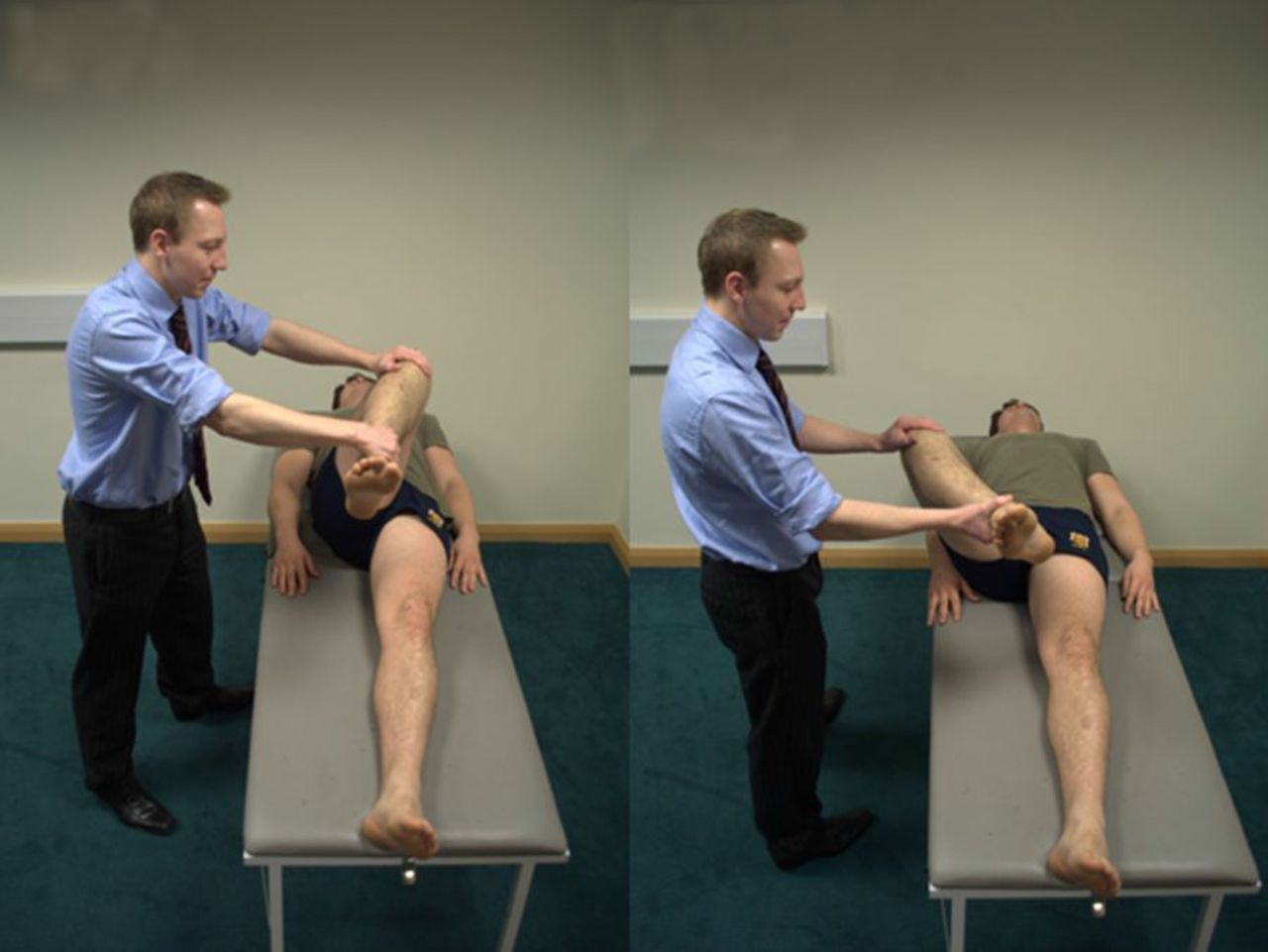
The hip impingement test is performed with the patient supine with hip and knee flexed to 90°, the hip is progressively rotated from external rotation to internal rotation while moving from abduction to adduction (Figure 2). A positive test elicits a sudden, sharp pain in the hip. Patients often report that the manoeuvre recreates their typical symptoms. A positive impingement test has been shown to be present in more than 90% of patients who go on to have FAI confirmed either radiologically or at the time of surgery,1,7 in addition it has a high positive predictive value for labral pathology.8

{kind=link}
{kind=link}
Hip impingement test. FADIR = flexion, adduction, and internal rotation. FABER = flexion, abduction, and external rotation.
INVESTIGATION
Plain radiology
Initially, an anteroposterior pelvis film with a cross-table lateral or Dunn view are all that are required. Morphological abnormalities as well as degenerative changes may be observed, although radiographic evidence can be subtle and the radiographs of patients with FAI are often reported as normal. This should not overshadow a convincing history and physical examination, and the need for appropriate management and referral remains. (Misdiagnosis and management as groin strain, low back pain, trochanteric bursitis, or early OA is not uncommon).
Magnetic resonance imaging (MRI) and computerised tomography (CT)
MRI arthrogram (MRA) with intra-articular contrast is the investigation of choice. In addition, intra-articular injection of local anaesthetic and steroid at the time of MRA is safe and of diagnostic value, particularly in the presence of early OA.
3D reconstruction of CT scans has proved useful in the recognition of subtle femoral deformities and in preoperative planning during the management of complex deformities.
TREATMENT
Non-operative
A course of non-operative treatment for most hip pathology may be tried first. Patients presenting with FAI or labral pathology can try modification of activity, avoiding excessive ranges of hip movement, with regular non-steroidal anti-inflammatory medication. Pincer impingement may be amenable to sports therapy that focuses on modifying dynamic hip flexion by maintaining core stability and a more upright stance during activity.9
Operative
Operative management has been shown to be effective in providing symptomatic relief and functional improvement. Despite evidence that FAI predisposes to OA,10 thus far there is no evidence that intervention will alter the natural history of the disease or the future need for arthroplasty.
Arthroscopy
The arthroscopic approach is minimally invasive with faster rehabilitation and a lower incidence of complications, but access to some areas of the joint is difficult. Complications of this approach include transient neuropraxias and fluid extravasation.11
Labral repair is possible and areas of chondral damage can be debrided or regenerative techniques implemented such as microfracture. Osteochondroplasty can be performed in cam impingement to reshape the head–neck junction, while acetabular rim trimming can be used to reshape the acetabulum with reattachment of the labrum.
Open hip dislocation
All procedures that can be performed arthroscopically can also be performed with an open approach, and this approach also provides better access to the postero-inferior portion of the hip. However, this is a major operation and carries a longer rehabilitation period and slightly higher complication rate.12
CONCLUSION
FAI is a common, often unrecognised condition causing hip pain and degenerative hip disease.
Careful history and examination (a positive impingement test in particular) are key to the diagnosis and enough to alert the GP to the possibility of FAI.
Surgery has two main goals: to provide symptomatic relief and functional improvement in the short term, for which there is increasing evidence; and potentially modify the disease process and delay or even prevent the onset of OA.
GPs have an important role to play in the recognition and management of FAI.
Notes
Provenance
Freely submitted; not externally peer reviewed.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received July 18, 2012.
- Accepted November 2, 2012.
- © British Journal of General Practice 2013
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

