


Abstract
Background Physical inactivity is a major, potentially modifiable, risk factor for cardiovascular disease, cancer, and other chronic diseases. Effective, simple, and generalisable interventions that will increase physical activity in populations are needed.
Aim To evaluate the effectiveness of a smartphone application (app) to increase physical activity in primary care.
Design and setting An 8-week, open-label, randomised controlled trial in rural, primary care in the west of Ireland.
Method Android smartphone users >16 years of age were recruited. All participants were provided with similar physical activity goals and information on the benefits of exercise. The intervention group was provided with a smartphone app and detailed instructions on how to use it to achieve these goals. The primary outcome was change in physical activity, as measured by a daily step count between baseline and follow-up.
Results A total of 139 patients were referred by their primary care health professional or self-referred. In total, 37 (27%) were screened out and 12 (9%) declined to participate, leaving 90 (65%) patients who were randomised. Of these, 78 provided baseline data (intervention = 37; control = 41) and 77 provided outcome data (intervention = 37; control = 40). The mean daily step count at baseline for intervention and control groups was 4365 and 5138 steps per day respectively. After adjusting, there was evidence of a significant treatment effect (P = 0.009); the difference in mean improvement in daily step count from week 1 to week 8 inclusive was 1029 (95% confidence interval 214 to 1843) steps per day, favouring the intervention. Improvements in physical activity in the intervention group were sustained until the end of the trial.
Conclusion A simple smartphone app significantly increased physical activity over 8 weeks in a primary care population.
INTRODUCTION
Decreasing physical activity and rising obesity are major global public health issues. Physical inactivity is a primary risk factor for obesity, diabetes mellitus,1 and a major cause of premature death from cardiovascular disease,2,3 cancer,4 and other chronic diseases.5,6 Although numerous studies have shown than even modest increases in physical activity are associated with a reduction in cardiovascular3 and all-cause mortality,7 the World Health Organization reports that obesity rates have doubled since 1980;8 while this is occurring, rates of physical activity are continuing to decline.9
For interventions to effectively increase physical activity, they need to:
motivate people to undertake a change in behaviour;10
offer realistic goal setting,11 which can be in conjunction with a primary care health professional;12 and
provide regular feedback on activity rates, such as provided by a pedometer.13
Such interventions can significantly increase physical activity,14 but changes are usually not sustained.10 Pedometers have additional disadvantages, such as the need for individuals to carry an extra piece of purchased technology and the instrument’s limited memory and feedback capability. Smartphone applications (apps), on the other hand, provide solutions to many of these limitations and, in addition, have added functionality that may be useful in the promotion of physical activity via third-generation ‘computer-tailored’ interventions.15 As a potential population-based intervention, apps are very attractive, as 90% of mobile phone users in the US are in possession of their telephone 24-hours a day.16 This randomised controlled trial (RCT) aimed to evaluate the effectiveness of a smartphone app in increasing physical activity in primary care.
METHOD
Participant recruitment
The SMART MOVE intervention featured an open-label, RCT of a smartphone app to promote physical activity in primary care. The study took place in the west of Ireland, with participants recruited and followed up through three primary care centres that make up the North Clare Primary Care Team; a rural primary care team covering an economically diverse, but predominantly white, population of approximately 8000 individuals.17
How this fits in
Numerous studies have shown that even modest increases in physical activity are associated with reductions in cardiovascular and all-cause mortality, as well as contributing to primary and secondary prevention of several chronic diseases. Despite this, obesity rates have doubled since 1980, with rates of physical activity continuing to decline. Effective, simple, and generalisable interventions are needed in primary care and this study demonstrates that use of a smartphone application can increase physical activity by over a 1000 steps a day. Such inexpensive, widely available, and user-friendly technologies should be considered as a component of future interventions to promote physical activity.
Enrolment into the study commenced on 15 August 2012 and all final outcome assessments were completed by 1 June 2013. The full study protocol has been published elsewhere18 and the study was carried out without any deviations from the protocol. Patients were eligible for the study if they were over the age of 16 years and active Android smartphone users; patients were excluded if they:
did not have an Android smartphone;
had an acute psychiatric illness;
were pregnant; or
could not undertake moderate exercise (for any reason including being overweight).
Multiple methods were used to recruit potential participants, including referral by their primary care health professional or self-referral in response to primary care centre and community advertisements or mailshots.
Randomisation and intervention
At the first contact (face-to-face or telephone), information about the study was provided to potential participants and they were invited to attend a preliminary screening meeting with the study investigators at their nearest primary care centre. If eligible, informed consent was obtained and participants were assigned a code. Randomisation occurred using random permuted blocks to ensure there were similar numbers of participants in the intervention and control groups. An independent investigator was responsible for generating the allocation sequence using the Research Randomizer computer software program (available at www.randomizer.org/form.htm) The same independent investigator was responsible for assigning participants to the intervention and control groups after being called at a central site.
After the randomisation code was assigned, baseline screening was conducted blinded, during which relevant clinical, anthropometric, psychological, and mobile-device data were collected. All participants then had the smartphone app downloaded onto their mobile phone to record their daily step count in order to provide a measurement of their baseline physical activity levels. The app provided automatic feedback and tracking of the step count and calories burned, and a visually appealing display of step count history and goal achievement. A 20-step test19 was carried out with each participant to calibrate the sensitivity level of the telephone for different individuals to ensure their step count would be recorded accurately. For the week following the screening visit (week 1), all participants were asked to carry their smartphone during waking hours and to continue operating at their normal physical activity levels. During week 1, the smartphone app display was not visible for either group and the investigators remained blinded.
At the end of week 1, the randomisation code was broken by the investigators. In this way, the allocation sequence was concealed from all study investigators and participants until all codes were assigned and week 1 was completed. Both intervention and control groups were then given similar physical activity goals and information on the benefits of exercise; however, only the intervention group was told how to use the app to help them achieve these goals. All participants were also issued with the Irish Heart Foundation Be Active physical activity promotion brochure20 by post or email and were instructed to keep their telephone charged and to always carry it during waking hours.
Those assigned to the intervention group were contacted by telephone at the end of week 1 and were told how to turn on the app’s display and about the usability features of the app’s settings and feedback. They were encouraged to interact with the smartphone app and were given a physical activity goal of 10 000 steps per day. Those assigned to the control group were also contacted by telephone at the end of week 1 and were given a physical activity goal of walking for 30 minutes per day in addition to their normal activity (the equivalent of 10 000 steps).21
At the end of weeks 1, 2, and 8, all participants were contacted via SMS and asked to email their step-count data to the research team using a ‘share data’ function of the app. All participants were invited back for follow-up testing within 1 week of finishing the trial.
Smartphone app and selection process
Smartphone apps are software applications designed to run on smartphones. The Accupedo-Pro Pedometer app (available at www.accupedo.com) was chosen for the study as it scored highest during a selection process using already-established desired criteria for smartphone apps promoting physical activity.22 These criteria included:
automatic feedback and tracking of step count and calories burnt;
visually appealing graphic display of step-count history; and
goal setting functionality and goal-achievement feedback.
Outcomes
The primary outcome measure was difference in mean daily step count between baseline (week 1) and follow-up (weeks 2–8). Step-count data were recorded automatically, beyond the control of investigators and participants, and stored by the app on the telephones of all trial participants. Seven secondary outcomes were measured at baseline and at the end of the follow-up period:
mean systolic blood pressure;
mean diastolic blood pressure;
mean resting heart rate;
weight and body mass index (BMI);
mental health, as measured by the Hospital Anxiety and Depression Scale (HADS);
quality of life, as measured by EuroQol (EQ)-5D; and
quality of life, as measured by EQ-VAS (EQ, visual analogue scale).
The recording of mean systolic blood pressure and mean diastolic blood pressure was carried out by a specifically trained research nurse using the current British Hypertension Society guidelines (available at www.bhsoc.org/latest-guidelines/how-to-measure-blood-pressure) and independently validated devices (Omron I-C10 if arm circumference was ≤17 inches or Omron R7 if arm circumference was >17 inches.23
Sample size
The required sample size was based on previous pilot work and calculated by taking into account the following assumptions:
individuals had an estimated mean daily step count at baseline of 4700 steps;
there would be a 10% reduction in the daily step count in the control group over the trial period;
the standard deviation (SD) of mean change in step count would be 2000 steps;
it would be possible to detect a relative increase of at least 20% in the change of the average step count between the intervention and control groups, with 80% power at a significance level of 0.05; and
there would be a drop-out rate of 15%.
Based on these considerations, approximately 40 participants per group were required.
Statistical analysis
Baseline data were summarised across the two arms using suitable numerical summaries and graphical techniques. For the primary outcome, the mean change in step count from week 1 to week 8 was compared between the intervention and control groups (unadjusted and adjusted). For the adjusted analysis (primary analysis), a generalised, additive, mixed model was used and explanatory variables identified a priori.18 The model was adjusted for the non-linear relationship that was evident between the primary outcome and time, the correlation within subject over time, baseline step count, age, sex, socioeconomic status, BMI, blood pressure, heart resting rate, mental health, quality of life, and smartphone literacy.
Analysis of missing data suggested they were missing at random and were, therefore, accounted for in the mixed model; the validity of this assumption was investigated by looking at the missing-data patterns and by modelling the probability of missing data based on the explanatory variables available. Model checking was performed using suitable model diagnostics and residual plots. All statistical analyses were performed using the software packages SPSS (version 21.0 R version 2.14.3), R libraries nlme, mgcv, and ggplot 2.
RESULTS
Participants’ recruitment and baseline characteristics
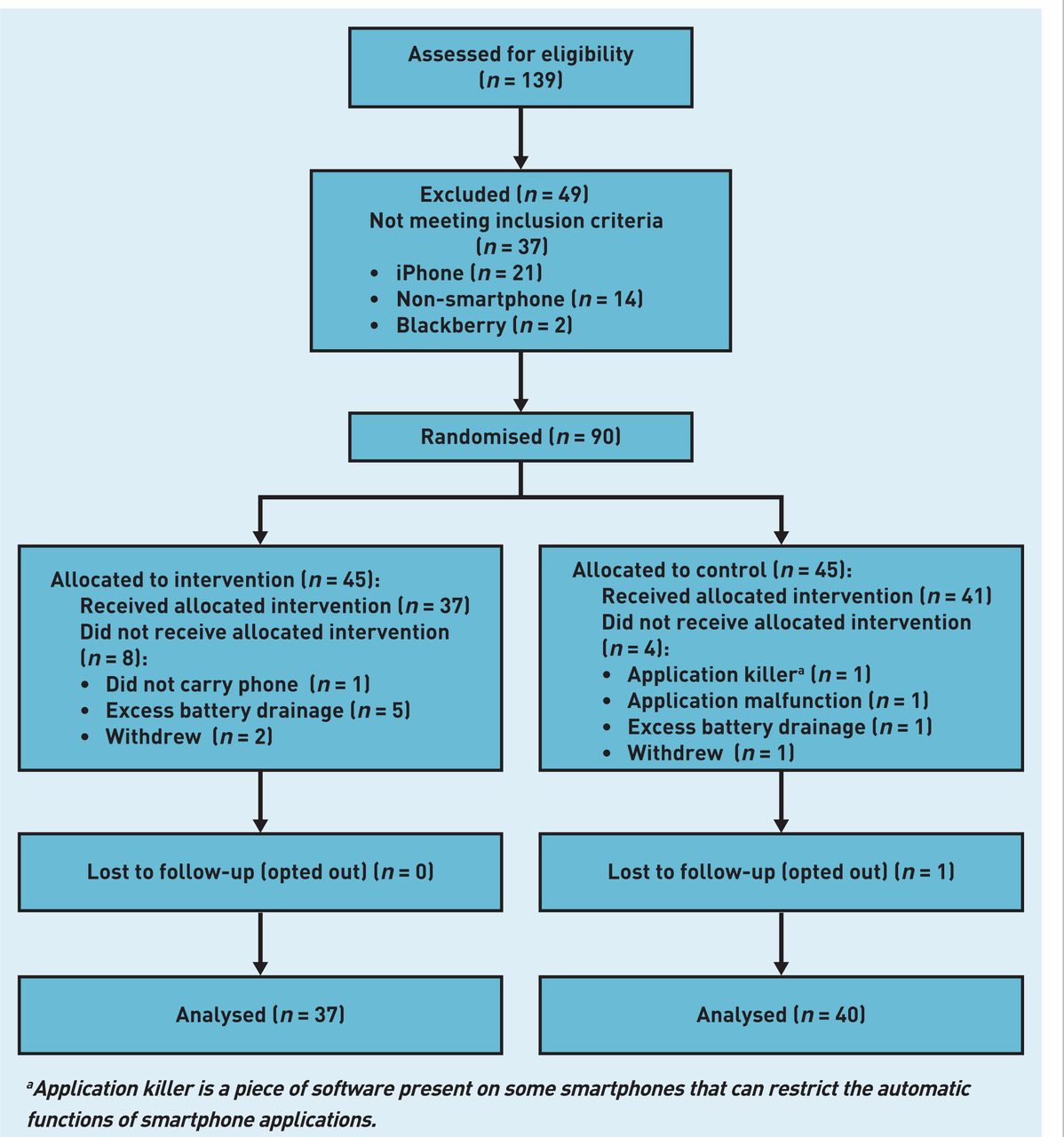
A total of 139 potential participants were referred by their primary care health professional or self-referred to the study. Of these, 49 (35%) were excluded, mainly due to not having the correct mobile device; as a result, 90 were eligible and randomised (Figure 1). Those randomised had a mean age of 44.1 (+/−11.5) years, a mean BMI of 28.2 (+/−5.5) and 58 (64%) were female. Other baseline clinical characteristics are outlined in Table 1.
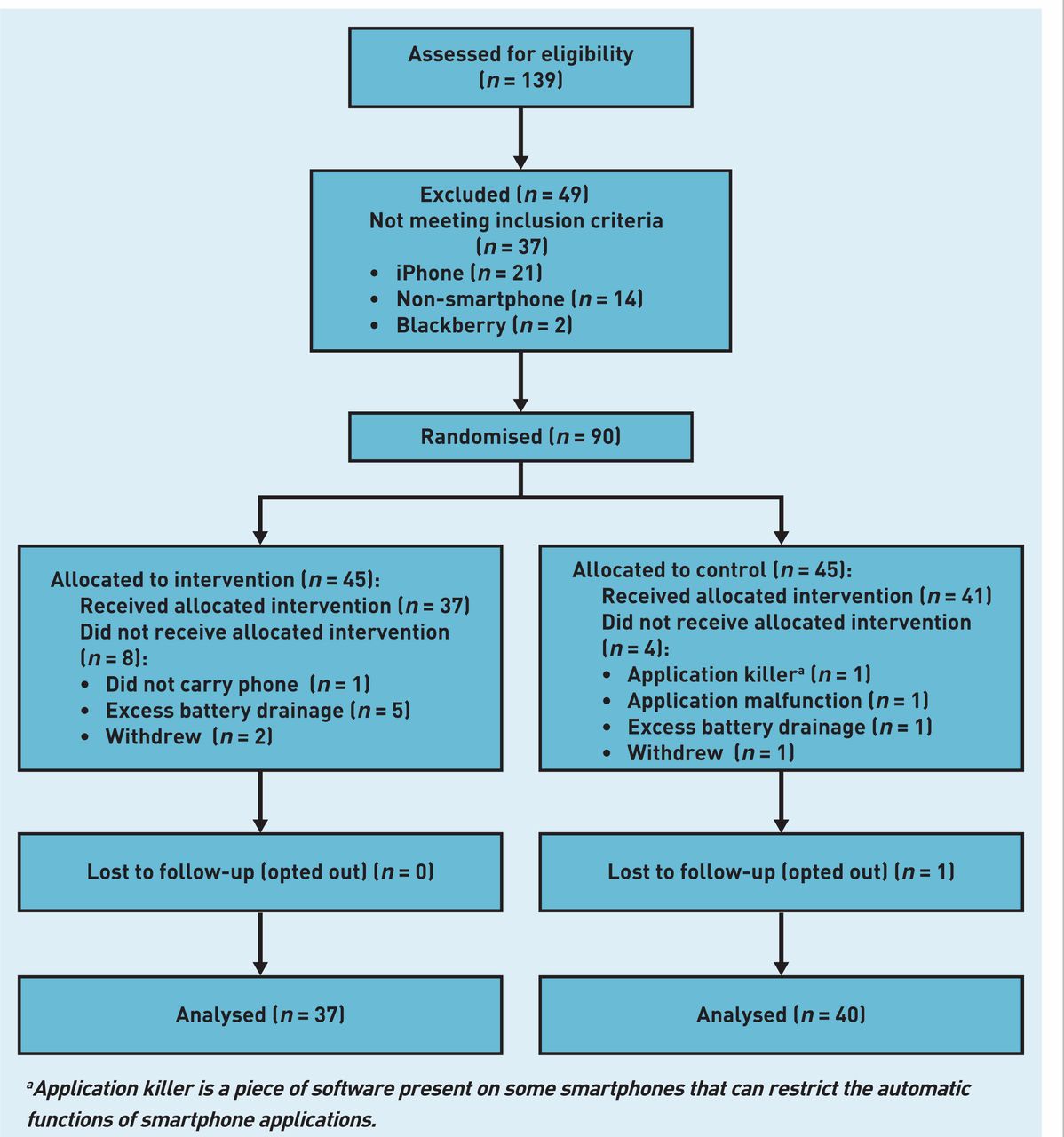
Participant recruitment and follow-up.
aApplication killer is a piece of software present on some smartphones that can restrict the automatic functions of smartphone applications.
Participants’ baseline characteristics.
There were no significant differences between control and intervention groups at baseline except for sex (P = 0.008) and one measure of quality of life (EQ-5D, P = 0.03). Both these differences were addressed by the a priori decision to adjust for these covariates, among others, in the analyses. Of the 90 participants randomised, 77 (86%) completed follow-up; most loss to follow-up occurred during baseline week (Figure 1).
Outcome data
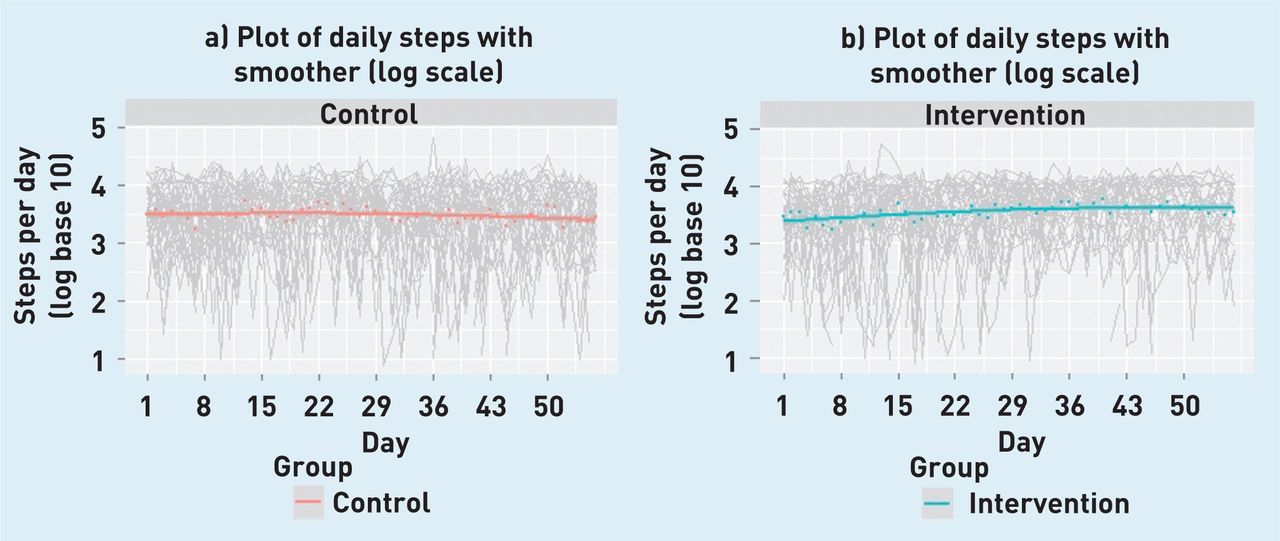
A non-linear effect of time is evident in plots of the daily step count. Figures 2a and 2b illustrate daily and smoothed mean steps (with 95% confidence interval [CI] for cubic spline smoother) for the step data when using a log (to the base 10) for ease of interpretation. The unadjusted mean difference (and SD) in improvement in step count between week 1 and week 8 for the control and intervention groups was −386 (SD = 3281) and 1631 (SD = 3842) steps, respectively (Table 2 and Figure 3), which is a difference in mean improvement of 2017 (95% CI = 265 to 3768) steps per day, favouring the intervention.

Daily step count with smoothed mean steps using a log to the base 10 for control and intervention groups.
Mean differences for outcomes in control and intervention groups.

{kind=link}
{kind=link}
{kind=link}
8-week improvement in mean steps in control and intervention groups.
Changes between baseline and follow-up for control and intervention groups for all primary and secondary outcomes are outlined in Table 2. No significant changes were observed for secondary outcomes of systolic blood pressure (+3.8mmHg versus −0.6mmHg), diastolic blood pressure (+0.9mmHg versus −0.9mmHg), weight (−0.16kg versus −0.33kg), and BMI (−0.06kg/[height in m2] versus −0.12kg/[height in m2]), although point estimates all favoured the intervention group.
After adjusting for possible explanatory variables, there was still evidence of a significant treatment effect (P = 0.009), where the difference in mean improvement in mean daily step count from week 1 to week 8 inclusive was 1029 (95% CI 214 to 1843) steps per day favouring the intervention.
Given that the mean daily step count during week 1 was 4771, a difference in improvement of 1029 steps per day is approximately a 22% (95% CI = 5 to 39) increase in physical activity, relative to baseline. There was evidence that the treatment effect was maintained at 8 weeks in the intervention group only (Figure 2).
DISCUSSION
Summary
The use of a smartphone app was found to increase physical activity over an 8-week period, when compared with data from the control group. The magnitude of change (over 1000 steps per day or approximately half a mile) is clinically meaningful and, if continued, is expected to result in long-term health benefits such as reduced cardiovascular and diabetes risk.
Although the control group demonstrated an initial increase in physical activity, this was followed by a decrease to baseline activity by the end of the trial period; the increase in activity seen in the intervention group, however, was maintained.
Strengths and limitations
The strengths of this study are the randomised design, the high completion rate for participants (86%) and the limited number of exclusion criteria. The relatively small number of potential participants that were excluded should strengthen the external validity24 of the results and may help to facilitate implementation, particularly with such an open recruitment strategy.
However, this study also had a number of limitations. The study was small and conducted in a single country in a white population with short follow-up. The relatively small sample size makes the study more vulnerable to a failure of randomisation, which the researchers sought to correct by using a multivariable analysis with explanatory variables identified a priori.18 The sample size also meant the study was underpowered to detect significant differences in the secondary outcomes.
In addition, there was a difference in baseline step count between control and intervention groups. This was not statistically significant but, nonetheless, this potential difference was recognised a priori and adjusted for in the final statistical model. Participants in the control-group were not given instructions on how to use the app and its display was not made visible on their telephones; however, they were aware that the app was running in the background, monitoring their daily activity. An experienced smartphone user in the control group could have accessed the app and, therefore, benefited from interaction with it, but this would decrease the likelihood of there being any difference between the groups. Alternatively, it is possible this awareness in the control group could have had a paradoxical effect on their motivation and physical activity.
Finally, due to the ‘sleep’ function on certain smartphone models, which forced the app to pause, some step-count data were not recorded’ this is why such data were not available for all participants at follow-up. However, this was similar for both groups over the course of the trial and was accounted for in the statistical modelling.
Comparison with existing literature
The SMART MOVE intervention shares the basic features and accuracy of pedometer-based interventions, which are associated with increases in physical activity of approximately 500–3500 steps per day, as well as significant decreases in BMI and blood pressure.14 A similar intervention effect size was reported here, but without the burden of cost associated with a pedometer purchase or the need for individuals to remember to carry this extra piece of equipment. The improvements in physical activity that have been seen when individuals use pedometers and other interventions are often not sustained and, indeed, appear to decrease with time.10 This is, in part, due to the fact that the practice of carrying the pedometer wanes with time,25 particularly among younger (>20 years) age groups.26
The advantage of using a smartphone app is that no additional instrument is required as people generally carry their mobile phones with them continuously. This in itself however, may not be sufficient to guarantee ongoing engagement with the app. Additional features may help such as feedback on time, speed, and energy consumption metrics, accompanied by attractive user-friendly graphic displays and a system of rewards for goals achieved. These features provide smartphone apps with significant potential as third-generation ‘tailored’ interventions that can be used to promote physical activity in particular.
A growing body of evidence shows that behaviour-change programmes using computer tailoring can be effective in changing lifestyle risk factors, such as physical activity.15 The emerging field of captology — the study of computers as persuasive technology — has described many of the mechanisms by which mobile phones have become such an important platform for changing human behaviour.27
Implications for practice
It has been suggested that significant improvements in public health in the future are more likely to come from behavioural change, rather than from technological or scientific innovation.28 The results of this current study would suggest that novel technologies, such as mobile devices and related smartphone apps, may become an important driver for the behavioural-change process. Rather than just providing more evidence that tracking in any form supports behaviour change, this trial represents an important step forward in the challenging issue of physical activity promotion. However, larger RCTs with longer follow-up are required to examine long-term sustainability of such improvements. Further data with longer follow-up using the smartphone app from the current trial is being compiled across six European countries.29
The exponential rise in global smartphone use in the past 5 years means that accessibility to such technologies is now the norm rather than the exception: in Ireland, 57% of mobile telephone customers possess a smartphone,30 while this number is greater than 60% in the US.31 Smartphone use is set to continue to increase rapidly as non-smartphone upgrades will be increasingly rare in the future.32 Meanwhile, the number of health-related smartphone apps available is over 13 000 and rising, of which 16% are exercise related.33
Several previous studies have used the SMS capability of mobile phones and smartphones in intervention and observational studies but the capability of smartphone apps themselves in research has rarely been exploited.34
The rapid penetration of smartphones throughout society and the ready availability of multiple apps promoting physical activity represent a unique opportunity in population health to use these devices to explore, understand, and positively change human behaviour. Such inexpensive, accessible, and user-friendly technologies should be considered a component of any future intervention to promote physical activity in primary care.
Acknowledgments
The authors are deeply indebted to: the staff of the North Clare Primary Care Team; staff of the Discipline of General Practice at the National University of Ireland, where the study was coordinated; the study collaborators in the National Centre for Biomedical Engineering and Science and the Health Research Board Clinical Research Facility; and all the trial participants.
Notes
Funding
Funding was awarded by the European Union’s Northern Periphery Programme 2007–2013, through the Implementing Transnational Telemedicine Solutions project (reference number: 7.13). The funder had no role in: the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Ethical approval
Ethical approval was granted by the Galway Regional Hospitals Research Ethics Committee (reference number: CA 760, 14 August 2012) and all participants provided written informed consent. This study is registered at Current Controlled Trials (reference number ISRCTN99944116; 1 August 2012). The design, conduct, and reporting of the trial follows Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: www.bjgp.org/letters
- Received January 7, 2014.
- Revision requested March 5, 2014.
- Accepted March 20, 2014.
- © British Journal of General Practice 2014
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

