


Abstract
Background Kawasaki disease is a rare childhood illness that can present non-specifically, making it a diagnostic challenge. The clinical presentation of Kawasaki disease has not been previously described in primary care.
Aim To describe how children with an eventual diagnosis of Kawasaki disease initially present to primary care in the UK.
Design and setting The Clinical Practice Research Datalink was used to find cases coded as Kawasaki disease. Hospital Episode Statistics, hospital admissions, and hospital outpatient attendances were used to identify the children with a convincing diagnosis of Kawasaki disease.
Method Questionnaires and a request for copies of relevant hospital summaries, discharge letters, and reports were sent to GPs of the 104 children with a diagnosis of Kawasaki disease between 2007 and 2011.
Results Most children presented with few clinical features typical of Kawasaki disease. Of those with just one feature, a fever or a polymorphous rash were the most common. By the time that most children were admitted to hospital they had a more recognisable syndrome, with three or more clinical features diagnostic of Kawasaki disease. Most GPs did not consider Kawasaki disease among their differential diagnoses, but some GPs did suspect that the child’s illness was unusual.
Conclusion The study highlighted the difficulty of early diagnosis, with most children having a non-specific presentation to primary care. GPs are encouraged to implement good safety netting, and to keep Kawasaki disease in mind when children present with fever and rashes.
INTRODUCTION
Kawasaki disease is an acute febrile illness of unknown aetiology that mainly affects children under 5 years old. Although rare, it is the commonest cause of acquired heart disease in children in the UK, with an incidence estimated to be 8 per 100 000 children under 5 years.1 The illness is characterised by the presence of a constellation of typical clinical features. The American Heart Association clinical diagnostic criteria are persistent fever (for more than 5 days) plus at least four of the following: changes in extremities, polymorphous rash, bilateral conjunctivitis, oral cavity involvement, and cervical lymphadenopathy.2 There is no diagnostic test.
The underlying pathology is a small- and medium-vessel vasculitis from which the coronary arteries are particularly susceptible to damage. Coronary artery aneurysms occur in 30–50% of cases as a complication of the disease.2 Treatment with intravenous immunoglobulin within the first 10 days relieves the fever in most cases and reduces the risk of coronary artery aneurysms by more than 75%.3
In its early stages it is hard to distinguish Kawasaki disease from the many other causes of self-limiting febrile illness seen in children. Delay in diagnosis results in late treatment, thus missing the opportunity to prevent cardiac complications.4 Most existing research into Kawasaki disease has been carried out in a secondary care setting, where the diagnosis is usually made and treatment given. A better knowledge of the early presentation of Kawasaki disease to primary care may help with earlier diagnosis and treatment.
This article describes a descriptive study of Kawasaki disease using cases that were identified in the Clinical Practice Research Datalink (CPRD) between 2007 and 2011, with the aim of describing how children with an eventual diagnosis of Kawasaki disease initially present to primary care in the UK.
METHOD
The CPRD was searched to find children under the age of 12 years who had had a diagnosis of Kawasaki disease between 1997 and 2011. The linked Hospital Episode Statistics was also searched for children under 12 years who were in the CPRD and had a hospital discharge diagnosis of Kawasaki disease. From these two sources of information, 755 children were identified as having had a diagnosis of Kawasaki disease. Identified cases were labelled with a unique study code and events recorded in the CPRD were reviewed for each case. The recorded clinical consultations and hospital admissions were examined, with particular focus on the diagnostic features of Kawasaki disease and cardiac investigations. Based on collation of this evidence, a list was produced of 528 children in whom the diagnosis of Kawasaki disease was convincing. Convincing cases were defined as those for whom the entry of the diagnosis of Kawasaki disease in the GP records correlated with a hospital admission, a discharge diagnosis, and hospital outpatient attendances, and there were no entries that suggested another diagnosis for the illness. There were insufficient data in the CPRD records to examine the presentation in primary care, so we decided to collect specific information on the more recent cases.
How this fits in
Kawasaki disease is a rare but serious cause of acute febrile illness in children and it is difficult to distinguish it from other self-limiting causes of fever. Coronary artery aneurysms are more likely as a consequence of the disease without treatment within 10 days. This study highlights the challenge of early diagnosis, with most children having a non-specific presentation to primary care. GPs are encouraged to implement good safety netting, and to keep Kawasaki disease in mind when children present with fever and rashes.
To study cases involving children who were likely to be remembered by GPs and to be still registered in the same practice, cases were selected from the most recent 5 years of data (2007–2011). This selection gave a set of 104 children. Short questionnaires (Appendix 1) were sent to the GPs of these children requesting further information about time to diagnosis, sequential order of symptoms, and whether they had considered Kawasaki disease among their differential diagnosis. There was an opportunity for free text to describe whether there was anything about the child’s illness that had made the GP suspect that it was unusual.
GPs were also asked to provide copies of relevant hospital summaries, discharge letters, and reports that could help verify the diagnosis. Any additional information provided by these, such as features seen in hospital, were combined with the questionnaire data. Where provided, consultation transcripts were used to check and complete the record of symptoms. Where the presence of clinical features recorded in the GP questionnaire conflicted with hospital records, the GP’s answers were used in the analysis, based on the assumption that the GP answered accurately using their electronic records. The hospital data on admission dates were used to correct some of the dates recorded by the GPs on the questionnaire, when it was possible that there had been a delay in coding in the GP electronic system.
GP, patient, practice, and hospital details were anonymised by the CPRD in the returned questionnaires and accompanying documents. All purely observational research using CPRD data is covered by ethical approval from a multi-centre research ethics committee.
RESULTS
Patient characteristics
The selection of cases produced 104 children who had been diagnosed in the most recent 5-year period (2007–2011). The GPs of these children were sent the study questionnaire.
Of the 104 questionnaires sent out, 89 were returned (86% response rate). From these responses, 15 cases were excluded: 5 cases had an alternative diagnosis, 3 cases had never been confirmed as Kawasaki disease, and 7 cases had inadequate or incomplete questionnaires. Thus there were 74 questionnaires completed for confirmed cases of Kawasaki disease. Ten of these questionnaires were returned without copies of hospital letters, but the quality of the information contained within the questionnaires was deemed sufficient to include these cases.
Of the 74 confirmed cases with completed questionnaires, 39 (53%) were boys and 35 (47%) were girls. Age at diagnosis ranged from 2 months to 8 years, with a peak at 3 years. Five children over the age of 5 (7%) were diagnosed with Kawasaki disease (Figure 1).
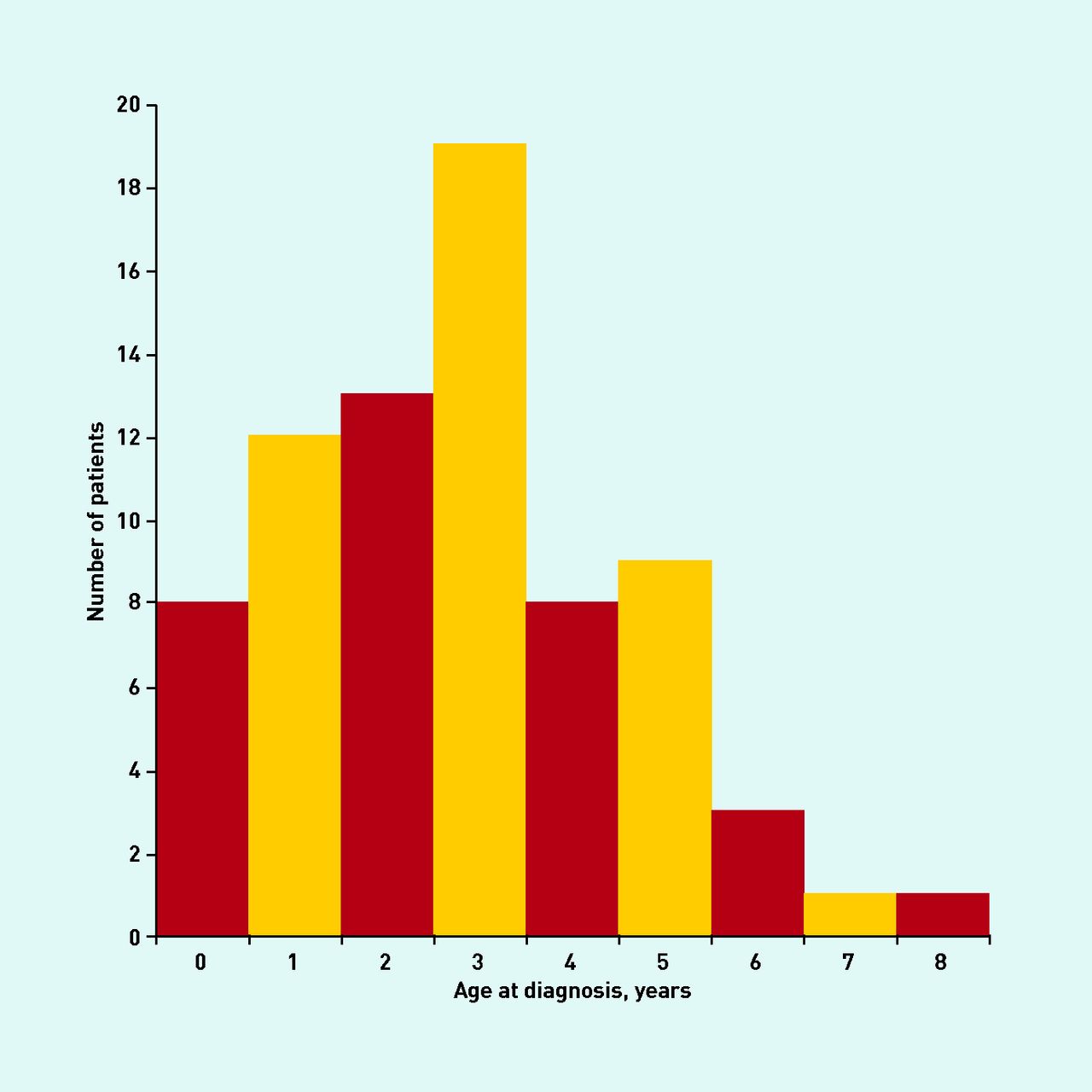
Age of diagnosis of Kawasaki disease.
Time to hospital admission
The number of consultations in primary care with the child before the illness was eventually diagnosed as Kawasaki disease ranged from one to seven consultations, but 41 children (55%) were seen only once before diagnosis.
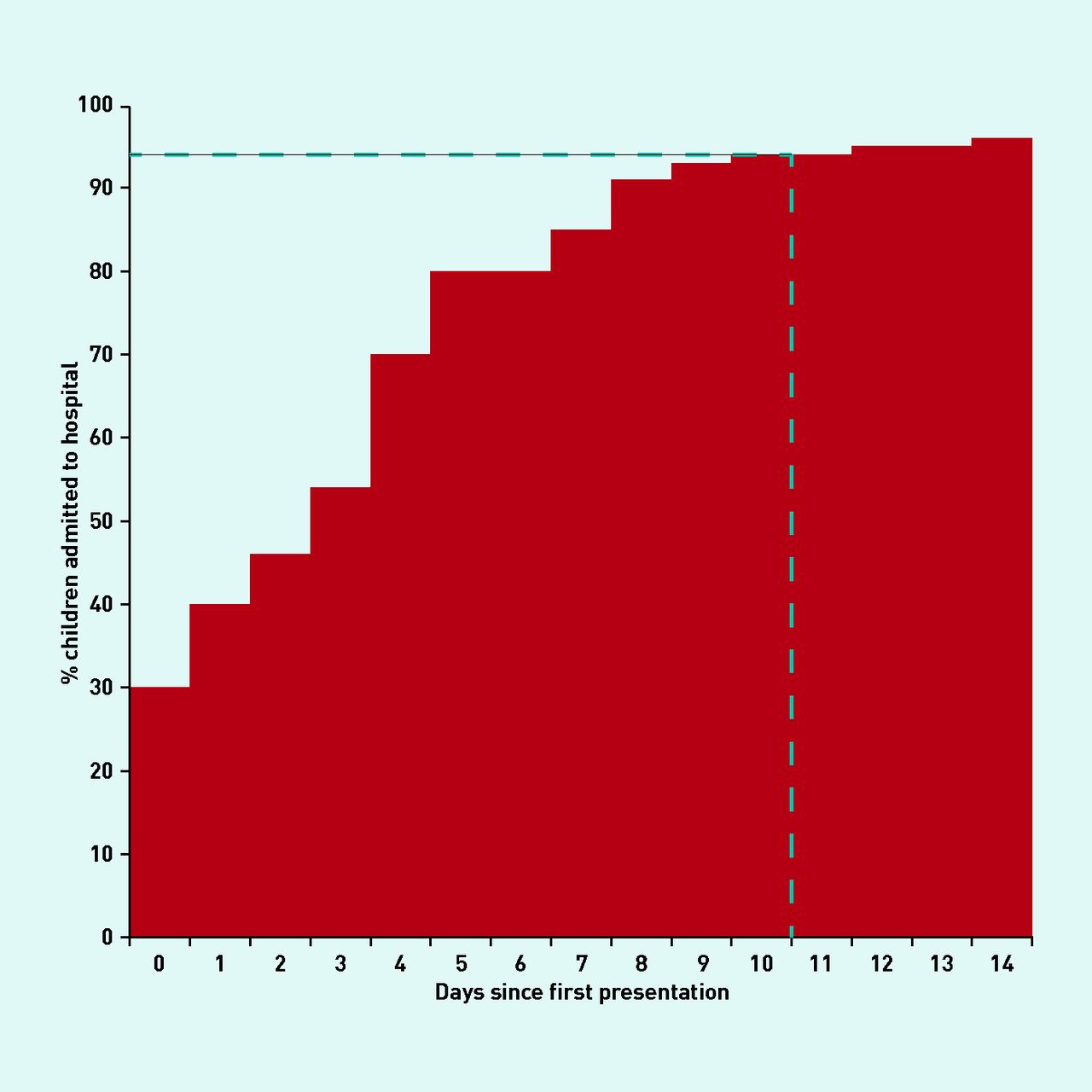
The duration of time between first presentation and admission to hospital ranged from 0–86 days. Median time to admission was 3 days. There was a delay of over 10 days between first presentation and admission for 7% of children (n = 5) (Figure 2).

The proportion of children admitted to hospital over time from first presentation.
Clinical features
At first presentation of the illness that was eventually diagnosed as Kawasaki disease, 21 children (28%) had none of the typical clinical features and 29 (39%) had only one feature (Figure 3).

{kind=link}
{kind=link}
{kind=link}
Number of Kawasaki disease clinical features at first presentation.
Of the 29 children with just one initial clinical feature, fever was most common (16 patients, 55%), followed by a polymorphous rash (eight patients, 28%). Other features seen in isolation at first presentation were lymphadenopathy (four children, 14%) and redness in the mouth (one child, 3%).
At the consultation in primary care (GP or A&E) that resulted in admission to hospital, only one child displayed none of the typical features of Kawasaki disease, and 11 children had one feature. Most children had three or more clinical features.
Apart from 5 days of fever, which is necessary for the diagnosis of Kawasaki disease, the feature that was most commonly found in patients in primary care was a polymorphous rash (n = 47, 64%). Other features encountered in primary care were cervical lymphadenopathy (n = 26, 35%), bilateral conjunctivitis (n = 23, 31%), and dry, cracked lips (n = 23, 31%). The rarest finding in primary care was oedema of the hands or feet (n = 10, 14%). Table 1 gives a summary of the clinical features and in which setting they were first noted.
Summary of clinical features evident across all cases
Clinical suspicion
Kawasaki disease was in the GP’s differential diagnosis for 17 patients (23%). Kawasaki disease was not considered by the GP for 41 patients (55%). This information was marked as not applicable for four patients (5%) and was unknown for 12 patients (16%).
Twenty-one GPs (28%) suspected that the child’s illness was unusual and 31 GPs (42%) did not. This information was marked as not applicable for two patients (3%) and unknown for 20 patients (27%). Reasons given for GP suspicion as free text fell into a number of categories (Table 2).
Reasons given for suspecting that there was something unusual about the child’s illness
DISCUSSION
Summary
At first presentation, most children who go on to have a diagnosis of Kawasaki disease have no features or only one clinical feature typical of the disease (Figure 3). Of those with just one feature, a fever or a polymorphous rash are the most common. Around one-third of children get admitted to hospital straight away (Figure 2), meaning that some children with a non-specific presentation are considered sick enough to warrant immediate admission. Overall, by the time most children were admitted to hospital they had a more recognisable syndrome, with three or more clinical features diagnostic of Kawasaki disease. Most GPs did not consider Kawasaki disease among their differential diagnoses. However, some GPs did suspect that the child’s illness was unusual, with duration of illness and typical or concerning symptoms being the most common reasons for this. It was notable that, according to the hospital letters for many cases, Kawasaki disease was also not diagnosed immediately on admission, with the child instead treated for another likely diagnosis. This demonstrates the difficulty of recognising Kawasaki disease, even in secondary care.
It is important that Kawasaki disease is treated within 10 days of onset to minimise cardiac complications. As GPs do not routinely record when symptoms start, it is not possible to calculate the proportion of children who met this target. However, time to admission from initial presentation could be calculated for all cases and the earlier the child was admitted, the more likely it would be that they were able to receive treatment on time. The median time to admission from initial presentation was 3 days. Sixty-nine children (93%) were admitted at or before 10 days, and five children (7%) definitely missed the treatment target as they were admitted after 10 days from initial presentation. Delay to admission may not be solely attributable to GPs, but is likely confounded by parental factors and access to care.
Limitations of the study
There are a number of limitations of this study. As it was a case series without a control group it is not possible to determine the predictive value of the clinical features seen in children early in the disease. The quality of information returned in questionnaires was variable: a number were incomplete, including missing dates, and others contained information that did not match accompanying hospital letters. This was compensated to some extent by using the attached letters and transcripts to fill in the missing data. Additionally, it was clear that some questionnaires were not filled in by the GP who originally consulted the child, so they were relying on the accuracy and completeness of GP records. This also prevented them commenting on the differential diagnosis and impression of the child. Finally, data on date of symptom onset could not be collected, meaning that it was not possible to comment on the number of children who received intravenous immunoglobulin within 10 days. Instead, time between initial consultation and hospital admission was used as a surrogate marker of the time delay.
Comparison with existing literature
Kawasaki disease is primarily a diagnosis made in secondary care and this is reflected in the setting of most of the current literature. Focus of current research includes epidemiology and risk factors,5–7 genetic aetiology,8,9 and treatment strategies and efficacy.10,11 No studies have yet specifically addressed the clinical decision making leading to diagnosis and treatment.
A large Chinese descriptive case series of 942 secondary care patients identified cracked lips (94%), conjunctivitis (93%), and a rash (88%) as the most commonly seen clinical features of the disease; all of which feature in the top four features identified by GPs in the current study. A rash and lymphadenopathy were the earliest emerging features (3.4 days and 3.6 days, respectively), which correlate to their common identification in primary care.12
A 2005 US retrospective study sought reasons for delay of diagnosis using the medical records (primary and secondary) for 104 consecutive cases of Kawasaki disease seen in Colorado during an outbreak of the disease. The study found that delay to diagnosis was not linked to the specialty of medical provider seen, number of antibiotics given for a misdiagnosis, or the total number of interactions with health care. However, it did identify two subgroups of patients with Kawasaki disease: one with clustered symptoms and early diagnosis, and the other with symptoms more dispersed over time and a delayed diagnosis.13 In both groups, mouth involvement, rash, lymphadenopathy, and conjunctivitis were the earliest features, which is consistent with results of the current study. The study was also able to relate each feature to the onset of the fever and the various interactions of the patient with the health service and depict this on a timeline. This shows that the average ‘clustered’ subgroup patient usually had one to two features in addition to the fever by the first visit to a doctor, potentially facilitating earlier diagnosis.
Implications for future research and clinical practice
Kawasaki disease is a challenging and difficult diagnosis to make in primary care. A GP may only see one case within their working lifetime, and most children may present initially with only a rash or fever. However, it is essential that these children be selected out from others with common self-limiting illness because without early treatment Kawasaki disease can cause serious cardiac complications. Despite its rarity, GPs should be supported to maintain Kawasaki disease within their differential diagnosis. GPs are encouraged to implement good safety netting; in this way children who develop subsequent clinical features can be identified. Therefore, it is worth having a low index of suspicion for Kawasaki disease in children with fever and rashes, as the potentially life-saving treatment has minimal risk.
As the first study of Kawasaki disease in primary care in the UK, this study offers new insight into the challenges of early recognition of a rare disease. This research has highlighted the need for better understanding of what makes a child with Kawasaki disease ‘unusual’ at presentation, especially when they have only a few clinical features. A follow-up interview study may help to tease out some of the additional factors that could aid earlier recognition. Kawasaki disease is one of many rare conditions that present in primary care for which a large-scale prospective study of its early presentation is likely to be of great interest and practical use to practising clinicians.
Acknowledgments
Thanks to the CPRD team for their help in administering the questionnaire.
Appendix
Questionnaire sent to GPs
Notes
Funding
This study presents independent research funded by the National Institute for Health Research School for Primary Care Research (NIHR SPCR). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health.
Ethical approval
Not applicable.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: www.bjgp.org/letters
- Received January 7, 2014.
- Revision requested January 25, 2014.
- Accepted March 11, 2014.
- © British Journal of General Practice 2014
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

