


Abstract
Background Older patients differ from younger patients in their perceptions of trust in doctors; their sense of shared decision making is particularly associated with their trust in the GP. Enhancing trust and improving shared decision making are thought to have positive health outcomes. Older patients are sometimes reported as being less frequently involved in decisions about their health care, however, and in having more unmet healthcare needs than younger patients.
Aim This study explored older patients’ trust in their GPs and their perceptions of shared decision making.
Design and setting Qualitative methods were used. Systematic sampling identified 20 participants, aged ≥65 years, from three GP surgeries in Devon, UK.
Method A constant comparative approach was applied to thematic analysis of transcribed interviews.
Results All participants valued feeling involved in decisions but differed regarding how they felt involved. Trust influenced preferences for shared decision making: a trusted GP ‘ally’, to competently manage participants’ increasing health-information requirements throughout the vulnerable ageing process, was important. Trust was affected by factors contributing to the facilitation of involvement. GP characteristics, communication skills, consultation duration, and continuity of care were common themes.
Conclusion Although limited geographically and subsequently by ethnic group, the present sample allows for reasonable transferability of the study to other UK populations. A range of factors are highlighted for consideration when planning primary healthcare delivery: to facilitate the optimal involvement of older patients in decisions about their health care, while enhancing their trust in the GP; to help minimise potential health inequalities for this patient group.
INTRODUCTION
Patients require trust as a prerequisite for engagement with complex organisations such as the primary healthcare system.1,2 Patients’ trust in their GPs may facilitate effective clinical encounters,3 and studies have identified health-related benefits of a trusting GP–patient relationship.4–6 Older patients place particular value on this trust.7 Factors affecting older patients’ perceptions of trust differ, however, from those of relevance among younger patients.6
Patient-centred care facilitates trust8–10 and is associated with improved health outcomes, including patient adherence with treatment advice, and satisfaction with health care.11–14 Historically, GPs have been poor at recognising individualised healthcare requirements for older patients.15 More recently, the importance of involving older patients, when identifying unmet healthcare needs, has been acknowledged.16 However, further research is warranted to provide practical guidance to clinicians.17
Shared decision making, as an ethical way to enhance patient autonomy, has been recommended as a key feature of good clinical care by the World Health Organization18 and in NHS policy.19 Shared decision making can be considered to comprise five components facilitated by the GP: defining the problem; providing information; exploring patients’ ideas, concerns, and expectations; checking their desire for involvement in a decision about their health care; and arranging for a future review of the decision.20 Patient involvement in decisions may vary from ‘passive’ to ‘highly active’.21 Dissonance between patients’ actual preferences for involvement and the doctor’s perception of their preferences22,23 can negatively affect patient satisfaction, emotional wellbeing, and treatment effect.21,24
Involving the patient in the decision is an important step when considering referral to secondary care. Although older patients are more likely to consult with their GP,25 it is younger patients who are more often referred.25 These inequalities exist with respect to a variety of health problems,26 with links to reduced survival rates suggested for older patients with ovarian cancer.27 The literature regarding shared decision making for older patients is generally sparse,6,28 but it reports variability in their desire29,30 and frequency31 of participation, when compared with younger patients.
A recent quantitative study32 revealed that a sense of shared decision making was particularly associated with the expression of trust in doctors among older patients when compared with younger patients. This finding contrasts with previous literature suggesting that older patients may prefer a more passive focus on receiving information, rather than on active participation in decisions,29,33 and with literature suggesting that trust can impede, as well as facilitate, older patients’ involvement.30 This study aimed to investigate the association between older patients’ trust in their GP and their perceptions of shared decision making. It was not appropriate to generate hypotheses in advance, therefore a grounded-theory approach was applied.34,35
How this fits in
A sense of shared decision making is associated with patients’ trust in the GP, for older patients in particular; and shared decision making and trust are reported to have positive health outcomes for patients. Despite this, older patients are involved less often in decisions about their health care when compared with younger patients; communication interventions to facilitate this process for older patients are outdated; and there is some evidence to suggest that there may be associated health inequalities. The present study uses qualitative methods to address a gap in the literature, by bringing together previously reported concepts regarding patient trust, and preferences for shared decision making, and highlighting their significance within the context of the older patient and the GP. Several factors are outlined that could be addressed by future policy developers to allow GPs to improve older patients’ involvement in decision making while facilitating their trust in the doctor.
METHOD
Qualitative methods were used, interviewing patients registered with three general practice surgeries in Devon, UK (Table 1). Sampling took place on three successive mornings. Potential participants were systematically identified with receptionists prior to initial contact in the waiting room. Selection and inclusion criteria were patients aged ≥65 years, registered with the surgery for at least 6 months. Patients were then approached consecutively. Potential participants were provided with a patient information sheet, and a reply sheet asking about the last time they saw a GP, how good that GP was at involving them in decisions about their care, whether they had trust in the GP, the patient’s contact details, and the name of the GP they usually see. They were invited to reply within 4 weeks. After receipt of patients’ agreement, the usual GP was contacted regarding exclusion criteria, for example vulnerability after bereavement, severe mental illness, severe cognitive impairment, end-stage disease, communication difficulties, or a learning disability. If none applied, responders were contacted to arrange an interview.
Characteristics of participants (n = 20)
Written informed consent was obtained prior to undertaking semi-structured interviews. Interviews were aided by a topic guide, digitally audiorecorded, and transcribed in full. Field notes documented the interviewer’s thoughts and later aided coding. The topic guide (Appendix 1) initially consisted of four questions, used flexibly. Participants were encouraged to discuss their own ideas and to accumulate emergent themes,36 which became probes for later interviews and topic guide subheadings.34 Interviews were all conducted by the first author.
A constant comparative,34,37 inductive approach meant there were no predetermined variables for data collection. The first person acted solely as the transcriber and coder. Audiorecordings were listened to repeatedly to improve validity of transcription. Units of meaning were thematically analysed35 by hand, enabling greater immersion in the data. New fragments of coding were constantly compared with old data to construct common themes37 and cautious propositional statements. Disconfirming evidence was actively sought; new codes accounted for data that appeared contradictory to developing themes. The sample size was reviewed during analysis as the importance of a breadth of participants across the age group and social backgrounds became apparent. Data collection continued until there were no more new themes emerging and thereby saturation was achieved. An audit trail was available through saved audiorecordings, coded transcription, and the researcher’s diary.
RESULTS
Of 50 participants approached, 22 replied. These individuals varied by sex, age, and social background, but not ethnic group. All 22 potential participants fulfilled the inclusion criteria; none were excluded after GP review; two declined at the point of arranging interviews, one because of ill-health, and one did not have time to participate. This left 20 who participated (Table 1).
All but one participant reported trust in the GP they last saw, and all reported that the GP had involved them in decisions about their health care. Many were able to discuss occasions of less trust or of feeling less involved, however, sometimes when consulting with another GP.
Older patients’ perceptions of involvement
A spectrum of involvement was reported with regard to decisions about health care. Some participants expressed definite trust in a GP’s opinion, particularly those who had experienced continuity of care. An explanation of this opinion was usually valued, however, and perceived by participants to represent patient involvement, augmenting their trust:
‘Whatever advice he [the GP] gives me, I would never have said “no”. I got full trust in my doctor. I know some people say well they don’t, but with mine I’ve got 100% trust. [...] I likes to go in the room and I knows it’s my doctor and I can speak to him. He tries to explain things to me. I had a X-ray on the chest a little while ago and he says “your heart’s a bit out of shape” like, but he said “don’t worry, you’re still working!”. He explained everything, yeah, and I mean he put me on the right road and I took his advice.’
(77-year-old male)
The provision of patient choice as a method of involvement was frequently valued across the participant group. Some described feeling overwhelmed by the complexity of information relating to a particular decision, however, and expressed greater trust in a GP who provided a definitive view in respect of their care:
‘The main one was whether to go for the bypass as opposed to the gastric band. I mean I had long talks with Dr T over that, but Dr T was very clear about the advantages and disadvantages. He’ll make suggestions, but I don’t have to abide by them or agree. So at the moment I’m confident that Dr T is kind of funnelling information and we’re trying to make sense of things between us.’
(67-year-old female)
’Certainly my GP always makes me decide, you know, “What would you like to do?” Well, I don’t know, and I have sat there and said to him, “I don’t know, what would you suggest?” [...] Sometimes I don’t want to know what’s happening for an operation or something you know. He never pushed the line. It was up to you, you had to … He couldn’t make my mind up, but he could advise me, which he did.’
(77-year-old male)
A few participants reported occasions on which they had taken a decision into their own hands, without first consulting the GP. Those who reported self-management, self-referral, or non-compliance, however, also reported returning to a GP in whom they had trust, to keep the GP informed and to discuss their opinion. This process, of retrospectively returning to the GP, was also reported by participants to be a method by which they felt involved in decisions:
‘But I was very naughty I’m afraid, I’ll admit that. For a few months I was having the tablets and not taking them, because I thought they’d hurt me [...] I said, I haven’t been taking them. I think he [the GP] said there’s nothing in them to hurt you, you’re on a very low dose, and I’ve been taking them ever since, every day.’
(96-year-old female)
‘It was my knees really, I can’t afford to be away from the house and incapacitated so I’m not gonna have them done after all. So I tried these silly stockings. I checked with Dr D. afterwards and he said, “Well, that’ll be alright”.’
(78-year-old male)
Older patients’ preferences for involvement
Participants discussed trust in the context of factors that affected their preferences for involvement. The oldest participants acknowledged increasing awareness of their own health and self-confidence in older age, wishing for information about ever more complex healthcare requirements. They wanted to trust in a GP who would act in their best interests; as an ally through the vulnerable ageing process, competently managing these increasing needs within the complexities of the healthcare system:
‘No, I mean when I was working I had four children to look after. If I went to the doctor it was in and out. Now all the bits have started dropping off! I mean you can’t know about everything, all these illnesses. Sometimes you need someone you can just talk it over with though, you know?’
(94-year-old female)
Less elderly participants reported that life experience gave them confidence to engage with a trusted GP as an ‘equal’. Their expectations of health care had increased with age, and participants reported that society had lost its ‘awe’ for doctors:
‘If I think back to when I was younger, I’m not sure I would have had the confidence to ask questions, or to even say why are we doing this, you know? [...] Yes, old enough and confident enough. I suppose now, I’m grown up and mixed with some grown-ups, a doctor’s a doctor.’
(67-year-old female)
These participants expressed the view that changes in the doctor’s status were associated with patient preferences; for a less paternalistic and more patient-centred relationship with a trusted GP:
‘Today we expect an awful lot more out of the health service than when I had my children 40 years ago. But I think one’s attitude changes; you have a better overall view. The more you’re involved, the more you see what a vast and overwhelming organisation it is. You just hope they’re getting it right. [...] The sort of hierarchy of the medical profession was very different wasn’t it, and they very much made the decisions for you. I remember going with a very small baby and had a very scathing doctor. I think we always thought the medical profession knows best and there is only one answer. Now you know life isn’t black and white and there are so many different aspects of things they need to weigh up with you.’
(77-year-old female)
The facilitation of older patients’ involvement
All participants reported common factors that facilitated their involvement in decisions about their health care, while also increasing their trust in the GP (Box 1). GP characteristics included: a patient-centred, caring, attentive, and holistic approach; appearing open and honest; and treating the patient as an equal. Many participants reported less trust, and suboptimal involvement, if they did not feel listened to or given enough time. Time seemed of greater importance with increasing participant age:
‘I feel more as an equal than I ever used to and that helps me to have a sensible, constructive conversation with him. I think being asked to contribute treats you as a person with your own views and the ability to make that decision for yourself […] but also to realise that I use them to help me with my health care. [...] I’ve got one lady friend, aged 99, and sometimes I talk to her and her doctors don’t seem to care. They don’t seem to often allow her to follow-up on things. You’ve got to be careful with the elderly you know. I sometimes think you are lucky to have a doctor who will take a bit of an interest, and take time, it’s important.’
(71-year-old female)
Factors that facilitate an older patient’s preference for, and involvement in, decisions about their health care, which also nurture trust in the GP–patient relationship
| Patient factors Self-awareness and self-confidence Increasing healthcare and health-information requirements Vulnerability associated with ageing Increasing expectations of health care | |
| GP factors | |
| GP characteristics | GP communication skills |
| Patient-centred | Attentive listening |
| Caring | Provision of explanation |
| Holistic | Acknowledgement of the patient ‘as an equal’ |
| Open and honest | Provision of choice |
| Willing to discuss GP expertise | |
| Offering of expert opinion | |
| Willing to discuss uncertainties | |
| System factors Optimal access to a GP Optimal consultation duration Opportunities to find a GP–patient ‘match’ Continuity of care with a ‘usual’ GP | |
| Societal and cultural factors The status of the GP as perceived by society | |
Participants talked positively about continuity of care with an individual GP. Perceptions of an ideal GP–patient match differed between individuals, however; the well-educated valued a GP with whom they could discuss similar interests. Despite some frail participants’ frustrations regarding access difficulties affecting continuity of care, some participants reported not wanting to trouble their trusted doctor unduly. This perception adversely impacted on their involvement in decision making:
‘I would want to see my own doctor because I have experience with them; I’ve built up trust with them. He would say, “Well, how’s Bert?” and, “How’s so and so”, you know? I must admit I don’t like seeing them temporary ones down there. [...] So I explained what it was and he knew what he’d done before like, and he knew exactly what to do, and what he suggested I agreed. [...] I would always go through Dr G, although they others may be completely legit, and they could just read it off the computer screen. There’s always downsides of taking medications that needs to be discussed isn’t there, and I wouldn’t want to usurp Dr G’s role in looking after me. You do build a relationship with people.’
(77-year-old male)
Several participants expressed trust in GPs who appeared both competent and confident in their abilities. ‘Meeting in the middle’, with the trusted GP talking openly about their expertise, as well as their uncertainties, and with the patient bringing knowledge about themselves, facilitated patient involvement:
‘You know she [the GP] was very, very confident. She came across as if she would listen to you and explain, and try and sort you out. I’ve been into the hospital once or twice. Once for an endoscopy because I had stomach trouble and it turned out I had a duodenal ulcer. Another time I went in and she thought I had a spot, you know which wouldn’t go, and they always think it might be cancer. She sent me in for that. That was alright, but she’s always very thorough like that you know, she’ll always make sure you go.’
(89-year-old male)
DISCUSSION
Summary
When compared with younger patients, older patients particularly value trust in the GP–patient relationship.7 There are positive associations between patients’ trust and their involvement in decisions about their health care, which increase with patient age.32 Despite a greater frequency of GP consultations for older patients,25 and recognition of the importance of patient-centred care for this age group,16 there is variability in their participation in shared decision making33 and inequality in primary healthcare outcomes.17,26
This study involved detailed individual interviews with 20 older patients attending their GP. Older patients’ trust in the GP and the optimal facilitation of their involvement in decisions about their health care appear closely associated, and in a manner that is complex (Figure 1). Participants valued the sense of involvement in decisions but differed regarding how they felt involved. Trust influenced participants’ preferences for involvement, and was in turn affected by factors contributing to the facilitation of patient involvement.
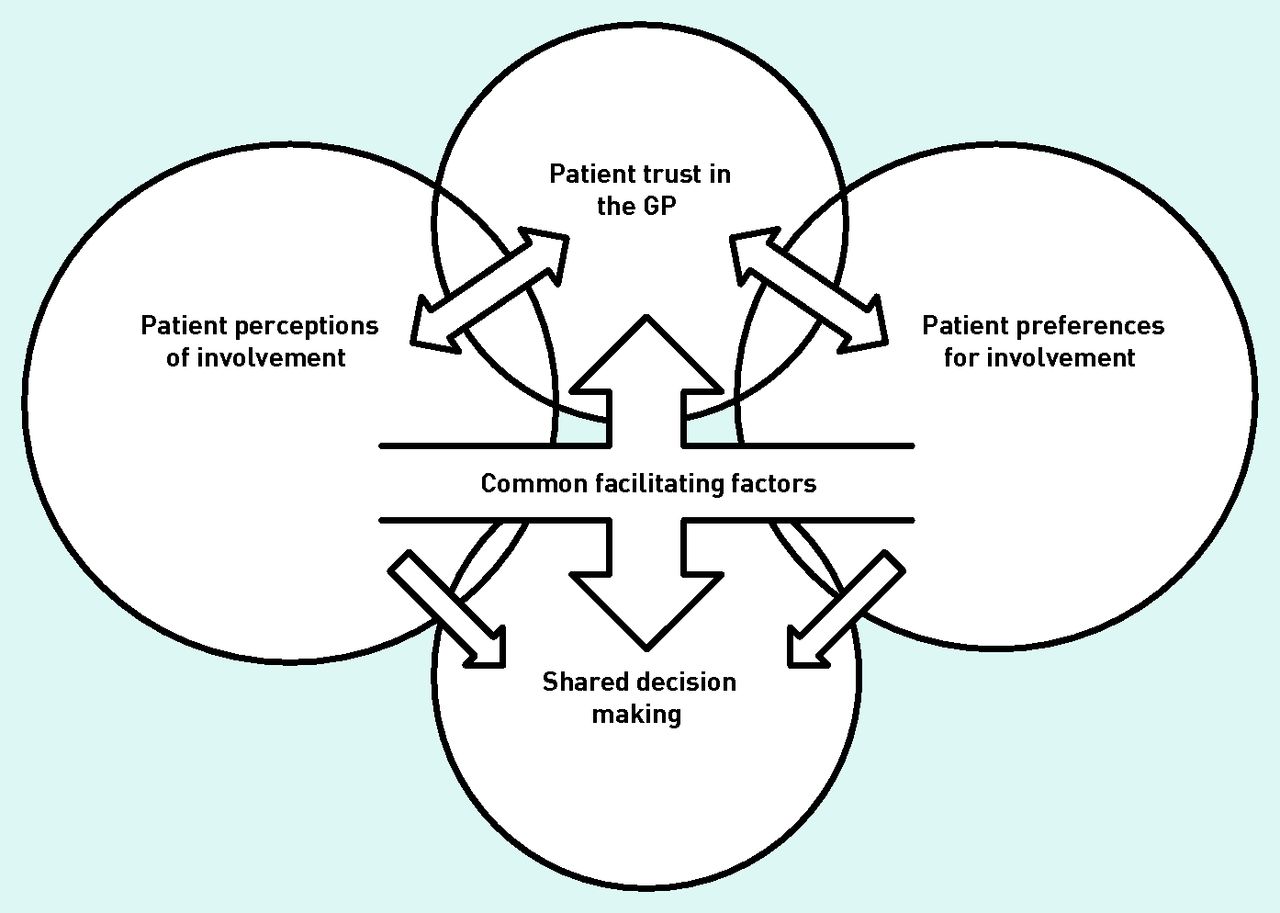
{kind=link}
Older patients and their GPs: associations and influences between shared decision making and enhancing trust.
Strengths and limitations
This study uses qualitative methods to address a gap in the literature and to inform potential changes in the way that GPs consult with older patients. There are few studies that explore shared decision making with older patients in depth.39 This study also contributes to the literature on identifying older patients’ unmet healthcare needs17 by highlighting factors that may facilitate this process, through shared decision making within a trusting GP–patient relationship.
The sample size was considered sufficient to achieve saturation40 and is comparable with previous studies using similar methodologies.41 The sample did not vary by ethnic group, as the majority of the Devon population are white.42 The possibility of findings being geographically context-specific, and that the sample may have contained more ‘frequent attenders’ than with another sampling method, was considered. However, the content of interviews spanned several years, locations, and discussed multiple GPs. Heterogeneity by age, sex, social background, and across practices allows applicability of emergent themes to be considered in a wider context.43 Consideration was given as to whether participants were referring to other factors, such as satisfaction, when discussing trust.44 Older patients have been reported to recognise these distinctions, however.45
Interviews were conducted by a GP. Participants were not informed of this unless they explicitly asked; this occurred on only three occasions, and at the end of interviews. Positional reflexivity, with consideration of how the researcher affected the analysis, was demonstrated through reflective notes and critical discussion between authors.46,47 Regrettably, there was a lack of independent researchers available for contemporaneous triangulation of data. The interviewing GP was usefully able to interpret interview content from an additional professional viewpoint, however.
Comparison with existing literature
The present study used detailed qualitative methods to explain apparent conflicts with findings from previous studies, which have suggested that older patients may not value feeling involved in decisions regarding health care,29,30,33 and that patients’ reported trust in doctors is most often associated with a preference to grant decisional authority.45
The present findings do, however, concur with the idea that patient perceptions vary regarding what it means to be involved in decisions.21,48 Firstly, some patients apply their perceived involvement paradoxically, by making a choice to let their trusted doctor make the clinical decisions.49 Secondly, the provision of explanation and choice to the patient, previously associated with patients’ trust,50,51 was reported to be a method of involvement, forming the ‘information giving’ part of the process recognised in the literature.20 Finally, a trusting GP–patient relationship increased the likelihood that participants would return to the GP, for a retrospective discussion of a decision made independently by themselves. Trusting GP–patient relationships have previously been associated with a sense of patient loyalty.20,52
The present study brings together previously reported concepts regarding patient trust and preferences for shared decision making within the context of older patients and their GPs. Participants recognised that increasing age is a risk factor for multimorbidity,53 a status known to increase preferences for shared decision making.54 The most older participants expressed a requirement for a GP ‘ally’ in the management of increasingly complex healthcare requirements. Participants recognised that, independent of multimorbidity, age brings greater expectations of health care,24 but that societal views can influence preferences for shared decision making.55
The particular influence of other factors on associations between patients’ trust is highlighted, and the facilitation of shared decision making, with respect to older patients and the GP. Continuity of care,56,57 and patient choice for a GP–patient ‘match’,51,58 have been associated with patients’ trust. Continuity with an available, approachable GP is particularly valued by older patients.59,60 Perceptions of the doctor’s competence, listening skills61 and holistic approach,62 are all known to affect trust.4 Perceptions of being given enough time28,59,63 appeared strongly associated with trust and patient involvement for the most older participants. The influence of societal factors on patients’ perceptions of access,64 and on trust in an individual practitioner,2 was particularly apparent for the present participants, who have lived through cultural change.
Implications for research and practice
The present participants did not all report each element of the shared decision-making process previously identified as being of importance in the literature.20 Patients’ perceptions of involvement are, however, considered important in predicting outcomes.48 Further research might usefully investigate whether it is the perception of patient involvement, or ‘actual’ patient involvement, that is of importance in determining patients’ trust. More consistency in training doctors in shared decision making has been suggested.65 There may be scope to harness the unique insight of older patients, who can reflect retrospectively on developments in doctors’ communication skills over time, for the purposes of training.
Current suggestions to empower older patients in shared decision making include involving a third person, and discussing the decision holistically.62 Previously developed communication interventions, designed to enable patients to initiate their own involvement in decision making,66 are not targeted specifically at older patients. Others,21,67 designed to assess older patients’ preferences for involvement,21,49,68 often appear outdated.69
Life expectancy is predicted to continue to rise.70 The present findings have the potential to inform future policy aimed at improving GPs’ care of older patients by facilitating shared decision making, through making adjustments to GP and system-related factors while taking account of the needs and characteristics of individual patients. Doing so may go some way towards addressing inequalities in healthcare outcomes for older patients visiting their GP.25,26
Acknowledgments
We thank the patients, GPs, and staff of St Leonard’s Practice, St Thomas’ Health Centre, and Ide Lane Surgery.
Appendix 1: Interview topic guide
Older patients and their GPs — exploring shared decision making in enhancing trust
This interview is part of a study exploring how trust is affected when GPs involve older patients in decisions about their health care.
Tell me about your last visit to your GP.
Can you think back and tell me about a time when there needed to be a decision made about your health care?
Prompt as necessary:This might have been starting or changing a medication, deciding whether to do an investigation or refer you to a specialist, or deciding whether you needed to be admitted to hospital.
Can you tell me about this decision and how you feel you were/were not involved?
How did your (lack of) involvement affect the way you thought and felt about the GP?
Can you tell me how your thoughts about your GP have changed over time and why you think that might be?
Prompt as necessary:Has your trust in your GP changed over time? Why do you think that is?
How could your GP improve the level of trust you feel in them?
Do you think the things you value in a consultation with your GP have changed as you have got older? If so, in what way? Why do you think that is?
Prompt as necessary:Has your involvement in decisions about your health care changed over time? In what way?
Would you like to be more or less involved in decisions about your health care now? Why is that?
Thank you for your participation in this interview. Is there anything else you would like to talk about that you think is relevant to the topic?
Notes
Funding
This study was conducted during a National Institute for Health Research (NIHR)-funded Academic Clinical Fellowship followed by an NIHR-funded In-Practice Fellowship for Joanne E Butterworth (IPF-2013-07-004).
Ethical approval
Ethical approval was obtained from the NRES Ethics Committee London — City & East (Ref 12L01585), as well as the local R&D Office, prior to commencement of the study.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org.uk/letters
- Received November 19, 2013.
- Revision requested February 13, 2014.
- Revision requested April 23, 2014.
- Accepted May 6, 2014.
- © British Journal of General Practice 2014
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

