


Abstract
Background Demand management defines any method used to monitor, direct, or regulate patient referrals. Strategies have been developed to manage the referral of patients to secondary care, with interventions that target primary care, specialist services, or infrastructure.
Aim To review the international evidence on interventions to manage referral from primary to specialist care.
Design and setting Systematic review.
Method Iterative, systematic searches of published and unpublished sources public health, health management, management, and grey literature databases from health care and other industries were undertaken to identify recent, relevant studies. A narrative synthesis of the data was completed to structure the evidence into groups of similar interventions.
Results The searches generated 8327 unique results, of which 140 studies were included. Interventions were grouped into four intervention categories: GP education (n = 50); process change (n = 49); system change (n = 38); and patient-focused (n = 3). It is clear that there is no ‘magic bullet’ to managing demand for secondary care services: although some groups of interventions may have greater potential for development, given the existing evidence that they can be effective in specific contexts.
Conclusions To tackle demand management of primary care services, the focus cannot be on primary care alone; a whole-systems approach is needed because the introduction of interventions in primary care is often just the starting point of the referral process. In addition, more research is needed to develop and evaluate interventions that acknowledge the role of the patient in the referral decision.
INTRODUCTION
Demand management defines any method used to monitor, direct, or regulate patient referrals, including the methods by which patients are referred from primary care to specialist, non-emergency care provided in hospital. This interface between primary and secondary care is a pivotal organisational feature in many healthcare systems, including the NHS.1
As demand outstrips resources in the UK, the volume and appropriateness of referrals from primary care to specialist services has become a key concern in the NHS. The NHS needs to make recurrent efficiency savings of up to £20 billion over 4 years,2 but current policy direction means that primary care funding is prioritised. This desire to shift resources to primary care means that demand management of secondary care services is needed.
As a result, several strategies have been developed to manage the referral of patients to secondary care. Referral management should not focus solely on reducing demand, but on ensuring that the right patients receive the right care, at the right time.3
A previous Cochrane review 4 in this area was limited to high-quality, controlled studies and found only 17 published papers. The authors concluded that there was insufficient evidence on organisational and financial interventions aimed at primary care, and inconclusive evidence on effective educational interventions. A report by the King’s Fund5 also highlighted the concerns of many with regard to the risks of managing demand without taking account of patient safety, and acknowledging that referral management has the capacity to increase clinical risk, as well as to reduce it. The current study aimed to go beyond previous reviews in the area by conducting an inclusive review of a broad range of evidence (from multiple sources) encompassing all study designs.
METHOD
This research was designed to answer the following question: what can be learned from the international evidence on interventions to manage referral from primary to specialist care? The inclusion criteria were:
Participants: primary care physicians, hospital specialists, and their patients.
Interventions: interventions that aim to influence and/or affect referral from primary care to specialist services by having an impact on the referral practices of the primary physician.
Comparators: the main comparator condition was the usual method of referral practice that is undertaken in the location where the intervention is being implemented. However, alternative comparators have not been excluded. Studies with no concurrent comparator (such as non-controlled before and after studies) were also included.
Outcomes: all outcomes relating to referral were considered including: referral rate, referral quality, appropriateness of referral, impact on existing service provision, costs, mortality and morbidity outcomes, length of stay in hospital, safety, effectiveness, patient satisfaction, patient experience, and process measures (such as referral variation and conversion rates).
Study design: with the increasing recognition in the literature that a broad range of evidence is needed to inform review findings, no restrictions were placed on study design. The criterion for inclusion in the review was that a study was able to answer or inform the research question. However, it has been noted that the quality of the study design and execution may affect the reliability of the results generated.
How this fits in
Demand management defines any method used to monitor, direct or regulate patient referrals, including referral from primary care to hospital. Previous reviews in the area have taken a focused inclusion criteria; this study took an inclusive approach to include all study designs and a broad range of public health, health management, management, and grey literature databases. Despite identifying 140 intervention papers, it is clear that there is no ‘magic bullet’ to managing demand for secondary care services: the perfect solution does not exist. To tackle demand management of primary care services, the focus cannot be on primary care alone: a whole-systems approach is needed because the introduction of interventions in primary care is often just the starting point of the referral process.
Iterative6,7 systematic searches of published and unpublished sources from health care and other industries were undertaken to identify recent, relevant studies. Searches were limited by date (January 2000 to July 2013). An initial search was generated with free text and subject heading terms combined to address the concepts of ‘primary care’ and ‘referral’ (Box 1). A broad range of public health, health management, management, and grey literature databases were searched (Box 2). After the initial search, phrase searches were undertaken for ‘referral management centres’ and ‘patient-focused interventions’ to make sure that papers had not been missed that were relevant to demand management. Citation searches of included articles and systematic reviews, and reference list checking of included articles, were also undertaken.
Main search strategy
Database: Ovid MEDLINE® In-Process & Other Non-Indexed Citations and Ovid MEDLINE® < 1946 to present>
*Primary Health Care/ (31226)
(primary care or general practitioner$ or gp).ti. (38162)
*Family practice/ or *General practitioners/(38225)
1 or 2 or 3 (83924)
(referral or referred or refer).ti. (10316)
demand management.ti,ab. (141)
*”Referral and Consultation”/ (17682)
Specialization/ (20898)
5 or 6 or 7 or 8 (43885)
4 and 9 (4328)
limit 10 to yr = ”2000–Current” (1978)
Data sources
MEDLINE In-Process and Other Non-Indexed Citations and MEDLINE via Ovid <1946 to present>
Cochrane Database of Systematic Reviews
Cochrane Central Register of Controlled Trials
Cochrane Methodology Register
Database of Abstracts of Reviews of Effects
Health Technology Assessment Database
NHS Economic Evaluation Database
All accessed via the Cochrane Library, published by John Wiley and Sons Ltd <from inception>
CINAHL via EBSCO <from inception>
Embase via Ovid <1974 to 2012 November 13 >
PsycINFO via Ovid <1806 to November Week 1 2012>
Science Citation Index, Social Science Citation Index, Science Conference Papers Index, Social Science
Conference Papers Index via Web of Science published by Thomson Reuters <from inception>
Scopus via Elsevier <from inception>
Applied Social Sciences Index and Abstracts (ASSIA) via ProQuest <from inception >
Sociological abstracts via ProQuest <from inception >
Social policy and practice via Ovid <1890s to October 2012>
International Bibliography of the Social Sciences (IBSS) via Proquest <from inception >
HMIC via NHS Evidence <from inception>
Health business Elite via EBSCO <from inception>
Business source premier via EBSCO <from inception >
Emerald management reviews via http://www.emeraldinsight.com/products/reviews/index.htm <from inception>
EPPI Centre databases: Bibliomap, Database of Promoting Health Effectiveness Reviews (DoPHER), Trials
Register of Promoting Health Interventions (TRoPHI) via http://eppi.ioe.ac.uk/ <from inception >
OpenGrey via http://www.opengrey.eu/ <from inception>
Opensource via http://www.greynet.org/greysourceindex.html <from inception>
Google Scholar via http://scholar.google.co.uk/ <from inception >
Titles and abstracts (where available) of papers were independently screened for inclusion by two reviewers, with disputes resolved by consulting other team members. Full paper copies of potentially relevant articles were retrieved for systematic screening. A data extraction form was developed using the previous expertise of the review team, trialled using a small number of papers, and refined for use here. Data extractions were completed by one reviewer and checked by a second. Non-English language articles with English abstracts were considered for translation.
The internal and external validity of studies was assessed using quality appraisal checklists based on work by the Cochrane Collaboration on risk of bias.8 Each paper was assessed by one reviewer and checked for accuracy by a second. Each paper was graded on a 3-point scale as being at higher risk of bias, lower risk of bias, or unclear risk of bias.8 Quality criteria for inclusion in the review were not set because the work was intended to be broad-based and inclusive; however, an account was taken of quality standards in the synthesis and presentation of the evidence as outlined below.
The strength of the evidence was also considered for each element of the intervention typology. Each group of papers was graded as stronger evidence, weaker evidence, inconsistent evidence, or no evidence (using criteria from Hoogendoorn et al ).9
RESULTS
The heterogeneity of the interventions’ aim, design, and outcome measures used preclude a meta-analysis. A narrative synthesis of the data was therefore undertaken to generate a typology of interventions and to explore the evidence for impact (or lack of impact) on outcomes.
One hundred and forty studies met the inclusion criteria for the review (Figure 1).10–150 Most studies (n = 121) were considered to be at lower risk for bias. Nineteen intervention studies were considered to be at higher (or unclear) risk of bias. The main risks for increased bias were related to a lack of participant details, only narrative results, single-point percentages reported without supporting statistics, data reported as charts only, inconsistencies in data reporting, poor response rates, attrition rate not reported, weak outcome measures, unclear study design, and evaluation tools that asked questions that strongly led responders towards positive answers.
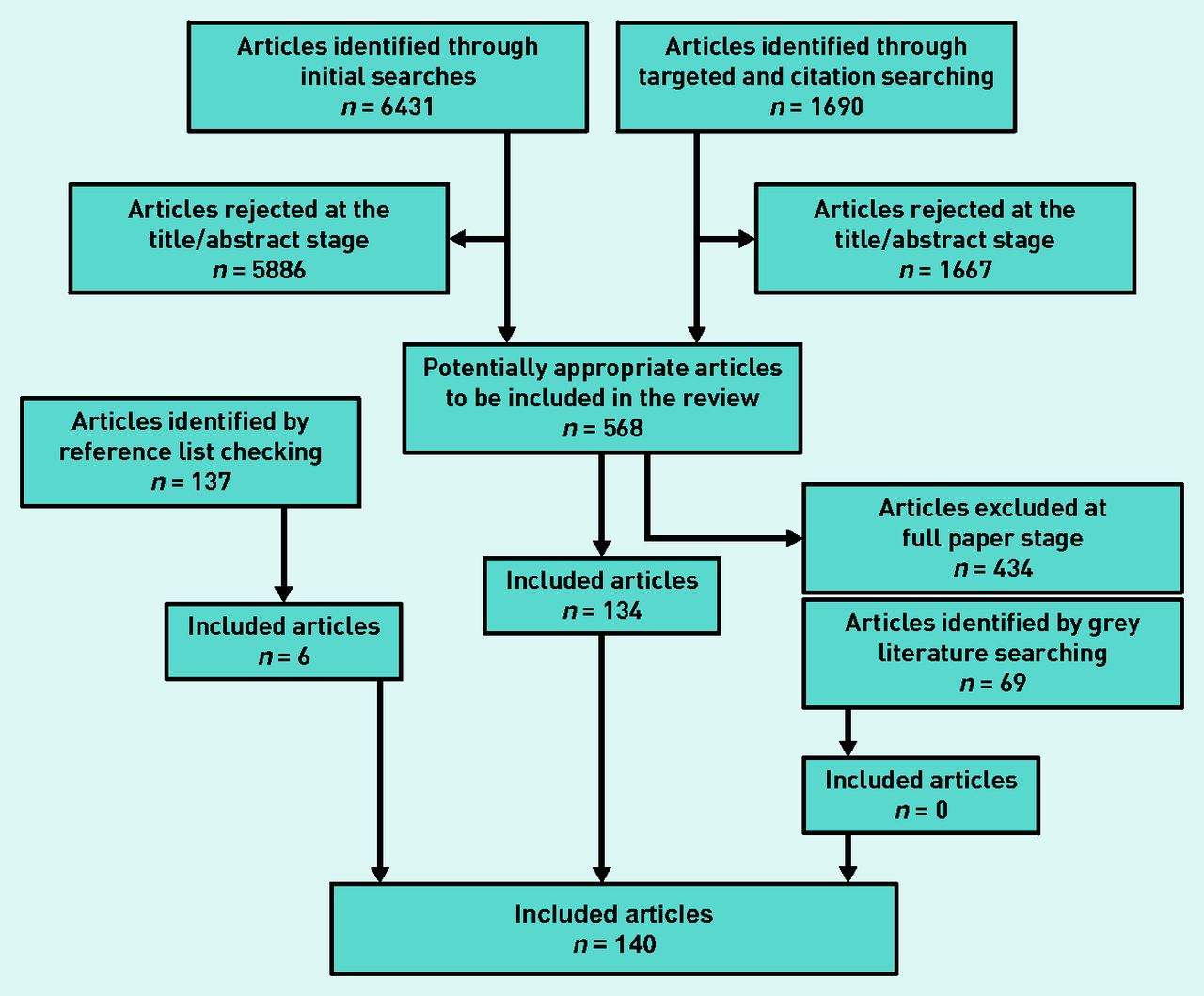
{kind=link}
Quorum diagram of included articles .
Studies included 44 randomised controlled trials (including 19 of cluster design), five non-randomised controlled trials, 43 before and after studies (without a concurrent control group), three controlled before and after studies, one case-control study, one economic analysis, five cohort studies, and 38 evaluation studies (described variably as audits, review, evaluation, and retrospective data analysis). Most were conducted in the UK (n = 83) or the US (n = 20). There were 10 studies from the Netherlands and nine from Australia. Additional studies were conducted in Canada (n = 3), Israel (n = 3), Italy (n = 3), Denmark (n = 2), Spain (n = 2), Finland (n = 1), Norway (n = 1), Hong Kong (n = 1), UK/China (n = 1), and one study where the country of origin was unclear.
The 140 studies were used to create a typology of studies by intervention. The studies were grouped into four intervention categories: GP education (n = 50); process change (n = 49); system change (n = 38); and patient-focused (n = 3). Table 1 gives a summary of the number of papers identified and the quality grading given to the evidence for each type of intervention.
Summary of intervention typology and quality appraisal
GP education interventions were defined as any intervention with a primary focus on GP education or training. The GP education intervention group included peer review and feedback (n = 4),10–13 interventions which consisted of formal GP training (including continued professional development) (n = 17),14–30 and the issuing of guidelines (without [n = 12]31–42 or with [n = 17]43–59 additional formal training and support for practitioners). The overall picture for interventions that aim to moderate referral processes by educating GPs is mixed, but some groups of interventions with more positive outcomes have been identified, including in particular peer review and feedback interventions (positive effects on referral, expenditure, and referral letter quality), as well as some elements of formal GP training (positive effects on referral rate, appropriate referrals, GP knowledge, consultation quality, and patient waiting time). However, given the variety of interventions reported, more research is needed to identify key successful interventions or particular elements of interventions that are more likely to be successful.
Process changes were defined as small-scale changes to some aspect of the individual referral process that did not involve the movement of staff or relocation of clinics, the methods in which referrals were triaged at hospital, or financial arrangements for referral. Process change interventions included: designated appointment slots and fast-track clinics for primary care referrals (n = 6),60–65 direct access to screening (n = 9),66–74 specialist consultation prior to referral (individual contact between a specialist and GP) (n = 11),75–85 electronic referral systems (n = 10),86–95 decision support tools (n = 10),96–105 and waiting list review or watchful waiting (n = 3).106–108 The overall picture for interventions that aim to moderate referral outcomes by changing an element of the referral process is mixed. Stronger evidence exists for electronic referral interventions (positive effects on referral, appropriate referral, GP satisfaction, reduction in non-attendance, waiting times, and transfer of information) and interventions including specialist consultation prior to referral (positive effects on number of referrals [referrals avoided], time to treatment, accuracy of diagnosis, and patient evaluation of services). These interventions are designed to provide better quality information to the specialist, either before or as part of a formal referral process.
System changes were identified as large changes impacting on all referrals made that involved the movement of staff or relocation clinics, the methods in which all referrals were triaged at hospital, or financial arrangements for referrals. System change interventions included the community provision of specialist services by GPs (n = 9),108–117 outreach or community provision by specialists (whole-scale provision of a hospital service within the community) (n = 10),118–127 return of inappropriate referrals (n = 2),128,129 the provision of additional primary care staff (n = 3),130–132 the addition or removal of gatekeeping systems (requiring a primary care provider to give access to secondary care services) (n = 4),133–136 changes to payment systems (n = 4),137–139 and referral management centre or other major triage systems (n = 6).140–146 The overall picture for interventions that aim to implement large system changes to impact on referral is mixed. Two of the types of interventions for which stronger evidence was identified involved the provision of specialist services in the community: either outreach/community provision by specialists or community provision of specialist services by specially trained GPs (positive effects on referral rate, appropriate referrals, patient satisfaction, and service accessibility). Stronger evidence also existed to suggest that the provision of additional staff in primary care (for example, nurses or counsellors) had a negative effect on referral outcomes. Some system change interventions conducted internationally such as those based on US healthcare payment systems, or where enormous change to the NHS system would be required (such as the removal of gatekeeping to secondary care services) would be impractical to implement in the NHS.
Very few examples were found of patient-focused interventions with outcomes relevant to managing demand. There is of course a large literature on patient education and activation measures, but this reports different outcome measures and was beyond the scope of the current review. The patient-focused interventions included the provision of health information/education (n = 2),146,147 and an intervention to address patient concerns and satisfaction (n = 1).148 The education interventions were graded as inconsistent and the patient concern intervention was graded as no evidence. This highlights a significant lack of evidence for patient-focused interventions, despite the huge potential impact that patients may have on the referral process.
DISCUSSION
Summary
It is clear that there is no ‘magic bullet’ to managing demand for secondary care services: the perfect solution does not exist and issues such as the context of a particular specialty or the location of a service impacts on the generalisability of interventions. In addition, the balance of the evidence is hard to interpret because some interventions that were reported frequently (such as referral guidelines) are supported by a contradictory evidence base and also receive mixed support from GPs and specialists. However, some groups of interventions may have greater potential for development, given the existing evidence that they can be effective in specific contexts.
It appears that GP peer review and feedback within a practice can be successful in changing referral practice and that providing training (or reinforcement) of guidelines can go some way to improving effectiveness. Process changes appear to be most effective when they result in the specialist being provided with more or better quality information about the patient; either electronically or through specialist consultation prior to the formal referral being made. The same is true in the most part for larger system changes. The community provision of specialist services by GPs (having been previously trained by specialists), outreach or community provision by specialists, and the return of inappropriate referrals, all engage the specialist and show the strongest positive effect on referral outcomes.
However, the evidence suggests that the addition of other primary care staff (such as nurses or counsellors) into a GP practice can increase the referral rate and reduce appropriateness of referral (although the amount of evidence was limited). The evidence for gatekeeping systems overall was very inconsistent and appeared to suggest that adding or removing a gatekeeping system had no positive impact on referral (although there were possibly small negative effects), although the evidence here was weaker. The same was true of payment system changes. However, it is also true that most of these US interventions would not be applicable or relevant in the UK within the NHS context.
Despite additional targeted searches, there was a significant lack of an evidence base to support referral management centres or other large triage systems. It was also surprising to find an almost complete lack of patient-focused interventions. This is particularly relevant given the potential impact that the patient may have on the referral decision.
Strengths and limitations
At times it was difficult to establish which outcome measures should be considered as positive, for example where interventions encourage referrals irrespective of their appropriateness, or where quicker referral processes are created, because these have a cost implication.
Deliberately inclusive search criteria were chosen including all study designs and grey literature sources in order to identify the most evidence and to develop the evidence base beyond previously conducted reviews. However, it is important to acknowledge that this creates an evidence base of mixed quality, for example, where study designs differ. This variation in quality has been considered as discussed above.
Although the evidence identified here is international in nature and some of it originates from countries with very different healthcare systems and processes to the UK, most studies have relevance in the UK within an NHS setting. It is likely that differences between specialties, UK demographic variation, and the impact of individual patients and practitioners will have an even stronger impact on the effectiveness of the interventions identified than their country of origin. There are two exceptions to this, namely, the addition or removal of gatekeeping systems and changes to healthcare payment systems. It would not be possible to make these types of changes in the UK; however, very few studies were identified in either of these categories and the evidence in both cases was conflicting.
Comparison with existing literature
The current study builds on previous reviews in the area4,5 by taking much broader inclusion criteria to create a more complete picture of interventions to manage referral from primary to specialist care. An inclusive approach was taken to include all study designs and a broad range of public health, health management, management, and grey literature databases. Consideration of a wider range of evidence helps to explain the mixed outcomes from more carefully controlled evaluations, and demonstrates the complexity and range of types of interventions that might be explored to address the overall problem of how to improve the referral process.
Implications for research and practice
To tackle demand management of primary care services, the focus cannot be on primary care alone; a whole-systems approach is needed because the introduction of interventions in primary care is often just the starting point of the referral process. Patton150 identified a ‘systems perspective as becoming increasingly important in dealing with and understanding real-world complexities’. With the introduction of interventions in primary care there are likely to be implications for secondary care. Furthermore, in a climate of ‘payment by results’, any intervention that reduces secondary care activity means a loss of income to secondary care and the implications of this would require consideration.
There are limitations in adopting this approach to demand management, because of the complexity of health systems. System designers need to be more mindful of the multitude of influencing factors and potential consequences from any given intervention. With this in mind, the authors have developed a logic model to illustrate the complexity of managing this demand.151
More research is needed to develop and evaluate interventions that acknowledge the role of the patient in the referral decision. Demand management is driven by the desire to reduce patient numbers and costs. It is therefore focused on process not outcome. Research is needed to examine what effect interventions focused on patient outcomes may have on demand (for example, would better care lead to less need for services?).
Acknowledgments
The authors would like to acknowledge the members of their steering group for their invaluable contribution to this research: Dr Martin McShane (NHS England), Professor Danuta Kasprzyk (Department of Global Health, University of Washington), Professor Helena Britt (Family Medicine Research Centre, University of Sydney), Ellen Nolte (RAND Corporation Europe/international), Jon Karnon (School of Population Health and Clinical Practice, University of Adelaide), Christine Allmark (Patient and Public Involvement [PPI]), and Brian Hodges (PPI).
Notes
Funding
This project was funded by the National Institute for Health Research (Health Service and Delivery Research Programme; project number11/1022/01). The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Health Service and Delivery Research Programme, NIHR, the NHS or the Department of Health. This paper represents emerging findings from a larger systematic review and logic model development project (http://www.nets.nihr.ac.uk/projects/hsdr/11102201).
Ethical approval
Ethical approval was not required for the secondary data analysis presented here.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have no competing interests to declare.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received February 13, 2014.
- Revision requested April 15, 2014.
- Accepted June 11, 2014.
- © British Journal of General Practice 2014
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.
- 12.
- 13.↵
- 14.↵
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.↵
- 31.↵
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.↵
- 43.↵
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.↵
- 60.↵
- 61.
- 62.
- 63.
- 64.
- 65.↵
- 66.↵
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.↵
- 75.↵
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.↵
- 86.↵
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.↵
- 96.↵
- 97.
- 98.
- 99.
- 100.
- 101.
- 102.
- 103.
- 104.
- 105.↵
- 106.↵
- 107.
- 108.↵
- 109.
- 110.
- 111.
- 112.
- 113.
- 114.
- 115.
- 116.
- 117.↵
- 118.↵
- 119.
- 120.
- 121.
- 122.
- 123.
- 124.
- 125.
- 126.
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.
- 132.↵
- 133.↵
- 134.
- 135.
- 136.↵
- 137.↵
- 138.
- 139.↵
- 140.↵
- 141.
- 142.
- 143.
- 144.
- 145.
- 146.↵
- 147.↵
- 148.↵
- 149.
- 150.↵
- 151.↵
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

