


Abstract
Background Self-monitoring of blood glucose (SMBG) confers no benefit for many people with type 2 diabetes not being treated with insulin. It accounts for 21% of diabetes prescribing costs.
Aim To improve care quality at reduced cost for type 2 diabetes by reducing unnecessary SMBG.
Design and setting Non-randomised, observational controlled study in two intervention clinical commissioning groups (CCGs) and one control CCG in east London.
Method In total, 19 602 people with type 2 diabetes not being treated with insulin were recruited from two intervention CCGs; 16 033 were recruited from a control CCG. The intervention (from 2010 to 2013) comprised implementation of a locally developed guideline, including IT support and peer feedback of performance. Data on practice prescribing SMBG testing strips were gathered using GP electronic health records. Information on costs were obtained via the ePACT electronic database.
Results Over 4 years, in all non-insulin type 2 diabetes treatment groups, use of SMBG was reduced in the two intervention CCGs from 42.8% to 16.5%, and in the control CCG from 56.4% to 47.2%. In people on metformin alone or no treatment, intervention CCGs reduced SMBG use from 29.6% to 6.0%, and in the control CCG use dropped from 47.1% to 38.7% (P<0.001). From 2009 to 2012 the total cost of all SMBG prescribing (type 1 and type 2 diabetes, including users of insulin) was reduced by 4.9% (£62 476) in the two intervention CCGs and increased in the control CCG by 5.0% (£42 607); in England, the total cost increased by 13.5% (£19.4 million). In total, 20% (3865 of 19 602) fewer patients used SMBG in the intervention CCGs.
Conclusion This low-cost programme demonstrated a major reduction in unnecessary prescribing of SMBG, along with cost savings. If replicated nationally, this would avoid unnecessary testing in 340 000 people and prescribing costs that total £21.8 million.
INTRODUCTION
Self-monitoring of blood glucose (SMBG) has an important role in the management of type 2 diabetes in patients treated with insulin and in some people treated with other antihyperglycaemic therapies, particularly sulfonylureas and meglitinides (repaglinide and nateglinide). This study is concerned with the use of SMBG only in people with type 2 diabetes who are not on insulin.
The National Institute for Health and Care Excellence (NICE) recommends SMBG as part of an integrated strategy to improve management in some of these people, namely those who are at risk of hypoglycaemia or at such risk when they are starting new treatment, performing certain activities, changing treatment, or ill. NICE also recommends that ‘the continued benefit of self-monitoring should be assessed in a structured way each year’.1 Other organisations also endorse the use of SMBG, including the Driver and Vehicle Licensing Agency (DVLA) and Diabetes UK:
‘It may be appropriate to monitor blood glucose ... at times relevant to driving to enable the detection of hypoglycaemia.’2
‘Self-monitoring of blood glucose levels should be available to people receiving sulphonylurea and prandial glucose regulators ... [and] ... for people not in the above treatment groups based on an individual assessment.’3
For the majority of patients with type 2 diabetes who are not treated with insulin, the evidence does not support the use of routine SMBG, and trials have established no clinically meaningful improvement in either glycaemic control or hypoglycaemia.4 In addition, although SMBG confers no additional benefit to most people with type 2 diabetes not treated with insulin, it is associated with significant harms, including poorer quality of life, as well as increased depression and anxiety.5–9 Patients report that use of SMBG can be associated with feelings of blame or failure, and disappointment when clinicians are disinterested in readings.10,11 Technology appraisals have highlighted inconsistent analytical performance, large variations in type and quality of meter, and considerable confusion among both patients and professionals about the quality and interpretation of results.12 In addition, routine use of SMBG has not been shown to be cost effective.13,14
Despite these concerns, routine SMBG prescribing across all non-insulin treatment categories for type 2 diabetes is widespread and increasing steadily, with wide variation of use across England.15 SMBG meters are cheap and readily available for around £15, although the majority are issued free of charge from manufacturers via health professionals. The cost accrues from the lifetime use of testing strips, costing approximately £15 for a pack of 50. In 2011, SMBG cost the NHS £158 million in England, accounting for 21% of all diabetes prescribing costs.15 Worldwide, three companies account for 75% of sales, expected to reach US $20 billion by 2015.16
How this fits in
In many people who have type 2 diabetes but are not treated with insulin, self-monitoring of blood glucose (SMBG) is an often unnecessary task that confers no benefit, while being at very high, and increasing, cost. This is the first study to describe a systematic and major reduction in unnecessary use of SMBG. In people on metformin or no treatment, SMBG use was reduced from 29.6% to 6.0%; in all non-insulin users the rate fell from 42.8% to 16.5%. If replicated nationally, this would avoid unnecessary testing in 340 000 people and save £21.8 million that is currently spent on diabetes prescribing.
As SMBG lacks evidence of effectiveness in many people who are not treated with insulin and may be harmful, this study sought to implement NICE guidance through local interventions to reduce inappropriate SMBG use in patients in whom it is unlikely to be beneficial. Translating new evidence into practice faces multiple obstacles, including professional belief and organisational structures.17 One model for changing behaviours is the COM-B system, using three synergistic behavioural change elements — capability, opportunity, and motivation — that promote change.18 The model allows:
interventions to be planned at the design stage, using educational methods to improve knowledge and capability;
implementation to be supported with practice facilitation;
computer-based reminders to improve opportunities for change and enhance motivation through comparative feedback of performance.19–21
No specific payment was used to incentivise performances, although practices in Tower Hamlets Clinical Commissioning Group (CCG), one of the intervention CCGs, could submit a completed audit of SMBG as part of a wider prescribing incentive scheme, for which they received a payment. In 2012, a similar scheme was introduced in Newham, the control CCG.
To the authors’ knowledge, this is the first UK study to describe the results of an intervention to systematically modify professional behaviour, with the aim of reducing the inappropriate use of SMBG. The opportunity was taken for a natural experiment to be conducted to compare performance between the two intervention CCGs and a third local CCG that shares many similar demographic and provider features, but which declined, at the time, to participate in this programme. The third CCG, therefore, acted as a control, although in the third year of the programme some support for a reduction in SMBG was also implemented in the control group.
The total cost of SMBG (for both type 1 and type 2 diabetes derived from national prescribing data) was also compared between CCGs in London and England.
METHOD
Setting
The intervention was carried out in two adjacent east London CCGs: Tower Hamlets and City and Hackney. Prior to 2013, CCGs had been termed primary care trusts, but this did not alter the number of practices in the study. The adjacent CCG in Newham opted not to participate in the programme at the time and, therefore, provided a local control CCG. These three CCGs are among the most ethnically diverse and deprived in London and the UK. Their combined population comprises 821 000 individuals, over half of whom are from minority ethnic groups; the population is served by 143 GP practices with approximately 500 GPs.22
In 2012, rates of diabetes in people aged ≥18 years were 6.0% in England, 6.3% in Tower Hamlets, 5.4% in City and Hackney, and 7.2% in Newham. All but four of the 143 (n = 139) practices in these three CCGs use the same web-enabled electronic health record in which all prescribing for type 2 diabetes is recorded.
Intervention
A multimodal strategy was used to bring about a change in clinical behaviour, comprising:
local guideline development, with dissemination to all practices;
educational meetings explaining the guidance;
a patient leaflet;
IT support on practice computers; and
performance feedback.
This programme was supported by the university-based, and GP-led, Clinical Effectiveness Group. All GP practices in the two intervention CCGs were included.
In 2010, local guidelines on SMBG were developed and agreed among key local stakeholders, which included the GP clinical diabetes leads in the CCGs, local hospital consultants for diabetes, specialist diabetes nurses, GPs, CCG prescribing advisers, and patients. This guideline was consistent with NICE guidance on diabetes1 and also provided more up-to-date evidence on SMBG management in people with type 2 diabetes not treated with insulin. In 2010, it was sent to all GP practice staff, diabetes hospital consultants, and specialist diabetes nurses in the two intervention CCGs, and was also accessible online.23 Patients were further informed of these policies through a leaflet that had been developed in conjunction with local people with type 2 diabetes; the leaflet outlined the reasons for testing blood glucose levels and the decision to test.
The guidance advised case-by-case review of self-testing in patients with type 2 diabetes not treated with insulin. It neither advised withholding testing from patients who wished to undertake it, nor suggested that there should be a blanket ban of any kind on the use of testing. It advised testing as recommended by NICE and the DVLA, after an informed discussion with the patient about the relative benefits, risks, and utility of testing in regard to the risks of hypoglycaemia and glycaemic control. It advised improved staff training and improved testing in those at risk of hypoglycaemia, along with measures to be taken, including treatment reduction in those at risk or who are fasting for any reason, including Ramadan.
A baseline audit was undertaken in April 2010, before the intervention was conducted, to compare SMBG use in each named GP practice in the intervention CCGs by type 2 diabetes treatment type. The audit was sent to each practice in the intervention CCGs, along with the guidance. An educational meeting in each intervention CCG supported this new guideline, together with a patient information leaflet for clinicians to give to patients. IT support consisted of providing practices with the computer searches to allow easy identification of relevant patients for review, with prompts to encourage review of SMBG use, and encouragement to review all repeat prescription requests for SMBG. A repeat of the CCG and practice audit was run in 2012, at 2 years after the programme start; this was sent to all practices (including those in Newham, the control CCG), showing comparisons between all named practices and each of the three CCGs.
In 2013, the audit and dissemination of results was repeated. In 2011 in Tower Hamlets, the prescribing advisers also included SMBG prescribing as one of several options practices could choose to audit as part of a local prescribing incentives scheme encompassing a number of prescribing indicators for which practices received financial reimbursement. There was no available information on how many practices undertook such an audit.
The control CCG did not receive the guideline or take part in its development. No educational meetings on SMBG and no baseline audit were provided. In 2012, Newham practices were sent the data on changes in SMBG use in each of the three CCGs; Newham then included reduction of SMBG as an option for a practice audit in a prescribing incentives scheme. The researchers do not know how many practices participated.
Data sources, collection, and analysis
Data related to practice prescribing of testing strips for SMBG in people with diabetes were collected retrospectively, both before and after the intervention for all three CCGs. This information came from three sources:
data on prescribing for type 1 and type 2 diabetes came from the patient electronic health record;
data of cost of prescribing for both type 1 and type 2 diabetes came from ePACT; and
data on the number of people with type 1 and 2 diabetes came from the QOF database.
The Clinical Effectiveness Group accessed anonymised data from the electronic medical records (EMIS web) in 139 of 143 GP practices in the three CCGs for each year from 2008–2009 to 2013–2014. Four practices in City and Hackney CCG that participated in this programme used other computer systems, from which data were not available for technical reasons. Data were collected for all people with type 2 diabetes, including diabetes treatment type and SMBG prescribing.
ePACT, an independent source of data for prescribing costs (http://www.nhsbsa.nhs.uk/3230.aspx), was used. This calculates the cost of all self-monitoring strip use for diabetes and allowed for the costs of each CCG to be compared with those for London and England. From 2008–2009 to 2012–2013, total SMBG prescribing activity and cost data for both type 1 and type 2 diabetes, including insulin use, were obtained for each CCG from the ePACT database. Data from The Quality and Outcomes Framework 2012–13 on the prevalence of diabetes were used to obtain the denominator for the per capita cost of total SMBG prescribing of type 1 and type 2 diabetes in the three CCGs.24
Changes in the differences in the proportion of patients using SMBG by treatment type were analysed in each practice from 2010 to 2013 as the baseline audit in 2010 was conducted before the intervention took place. The year 2009–2010 was used as the comparative date for SMBG costs and the changes in total per capita cost of SMBG for diabetes in each CCG. Results from the intervention CCGs were compared with those from the control CCG, London, and England.
Stata (version 10) was used to estimate the differences in prescribing before and after the intervention in the intervention and control CCGs, and χ2 tests were used to compare differences in proportions. The study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidance.
RESULTS
Data were collected for 139 practices, 36 of which were in Tower Hamlets CCG, 40 in City and Hackney CCG, and 63 in Newham CCG. In 2012, 44 464 patients with type 2 diabetes were registered in the three CCGs: 24 978 in the two intervention CCGs (Tower Hamlets and City and Hackney), and 19 486 in Newham, the control CCG. Of the patients aged ≥18 years with type 2 diabetes, 18 441 in the two intervention CCGs and 15 522 in the control CCG were not being treated with insulin. In Tower Hamlets, 66% of those aged ≥18 years with type 2 diabetes were <65 years; this percentage was 67% in Newham and 59% in City and Hackney.
The number of people with type 2 diabetes on no treatment or metformin therapy, who were prescribed SMBG between 2010 and 2013, are shown in Table 1. The proportion prescribed SMBG in the no-treatment or metformin-only group was significantly reduced in Tower Hamlets from 26.8% in 2010 to 4.2% in 2013, a reduction of 22.6% (95% confidence interval [CI] = 21.6 to 23.3), and in City and Hackney from 33.1% to 8.5%, a reduction of 24.6% (95% CI = 23.0 to 26.1) (Figure 1). The combined reduction in both intervention CCGs was 23.6% (95% CI = 22.7 to 24.4); 29.6% in 2010 to 6.0% in 2013 (data not shown); this significantly exceeded the 8.4% (95% CI = 6.6 to 10.0) reduction in Newham, the control CCG, where the proportion fell from 47.1% to 38.7% (P<0.001).
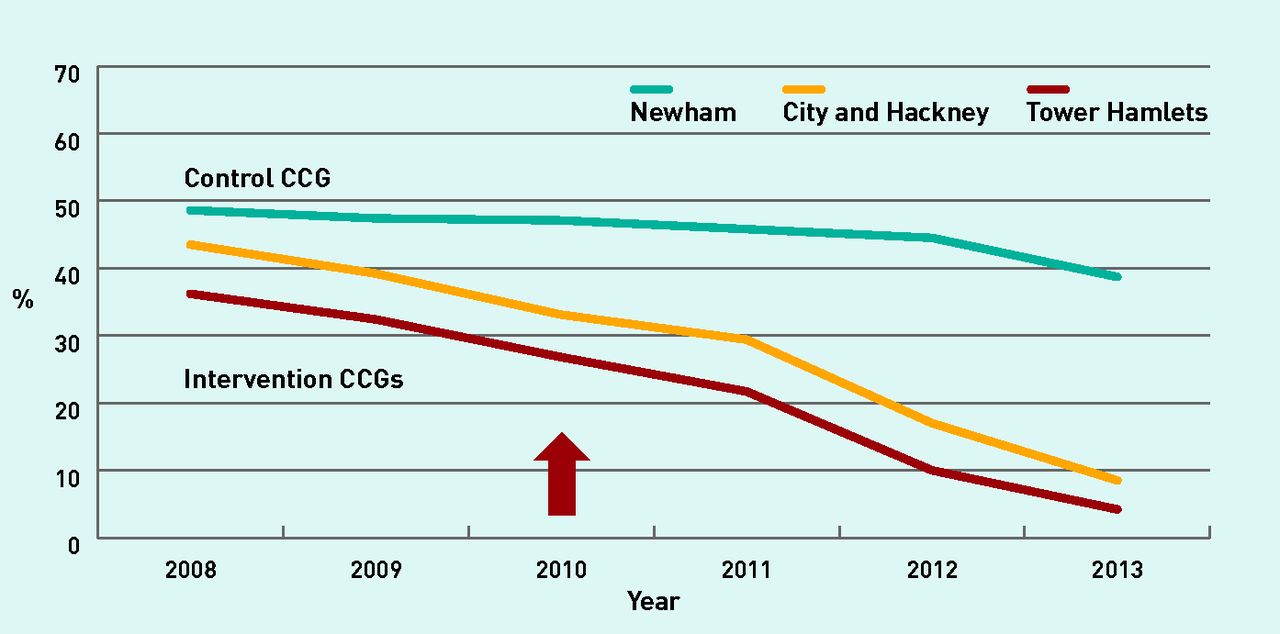
Proportion of patients with type 2 diabetes on no treatment or metformin only, who are prescribed self-monitoring blood glucose. The red arrow marks the start of the intervention.
CCG = clinical commissioning group.
Self-monitoring of blood glucose use in people with type 2 diabetes receiving no treatment or metformin only
The number of people with type 2 diabetes not treated with insulin, who were prescribed SMBG, are shown in Table 2. Significant reductions (2010 to 2013) were also shown in all non-insulin use of SMBG: the rate for Tower Hamlets fell from 41.5% to 14.9%, a reduction of 26.6% (95% CI = 25.4 to 27.7), whereas City and Hackney fell from 44.4% to 18.6%, giving a reduction of 25.8% (95% CI = 24.4 to 27.2) (Figure 2). The combined reduction in the two intervention CCGs was 26.3% (95% CI = 25.4 to 27.2), from 42.8% to 16.5%, which significantly exceeded the drop of 9.2% (95% CI = 8.0 to 10.3) in the control CCG, which fell from 56.4% to 47.2% (P<0.001).
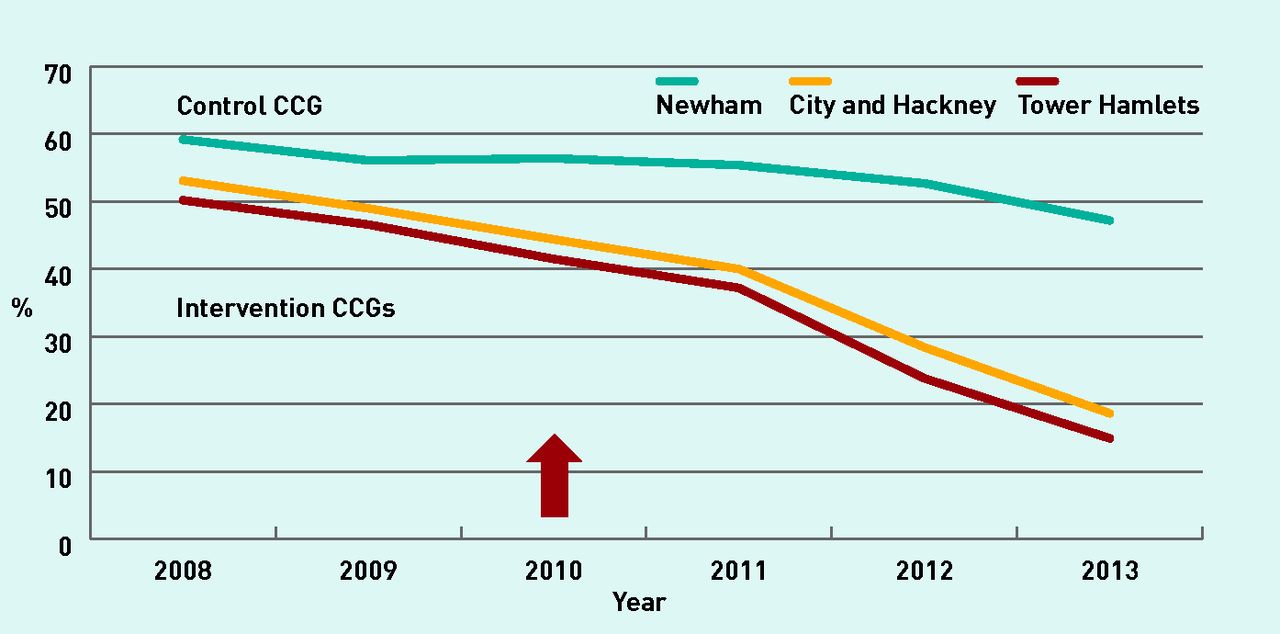
Proportion of patients with type 2 diabetes, excluding those treated with insulin, who are prescribed self-monitoring blood glucose. The red arrow marks the start of the intervention.
CCG = clinical commissioning group.
Self-monitoring of blood glucose use in people with type 2 diabetes, excluding all those on insulin therapy
In 2009–2010, the total cost of SMBG monitoring for both type 1 and type 2 diabetes, including users of insulin, in Tower Hamlets, City and Hackney, and Newham was £614 789, £663 772, and £859 595 respectively. By 2012–2013 this had reduced by £53 210 in Tower Hamlets and £9266 in City and Hackney (combined total), but had increased by £42 607 in Newham (Table 3). This is a reduction of 4.9% (£62 476) in the combined intervention CCGs, and an increase of 5.0% (£42 607) in Newham, the control CCG.
Cost of self-monitoring of blood glucose
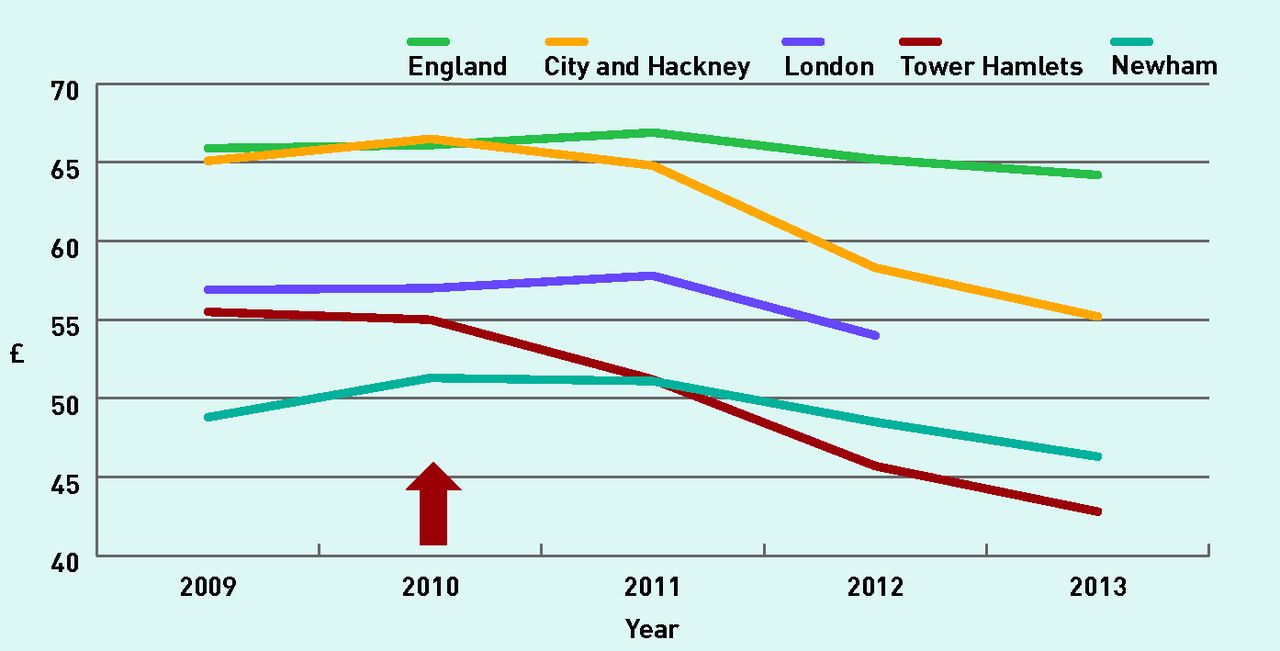
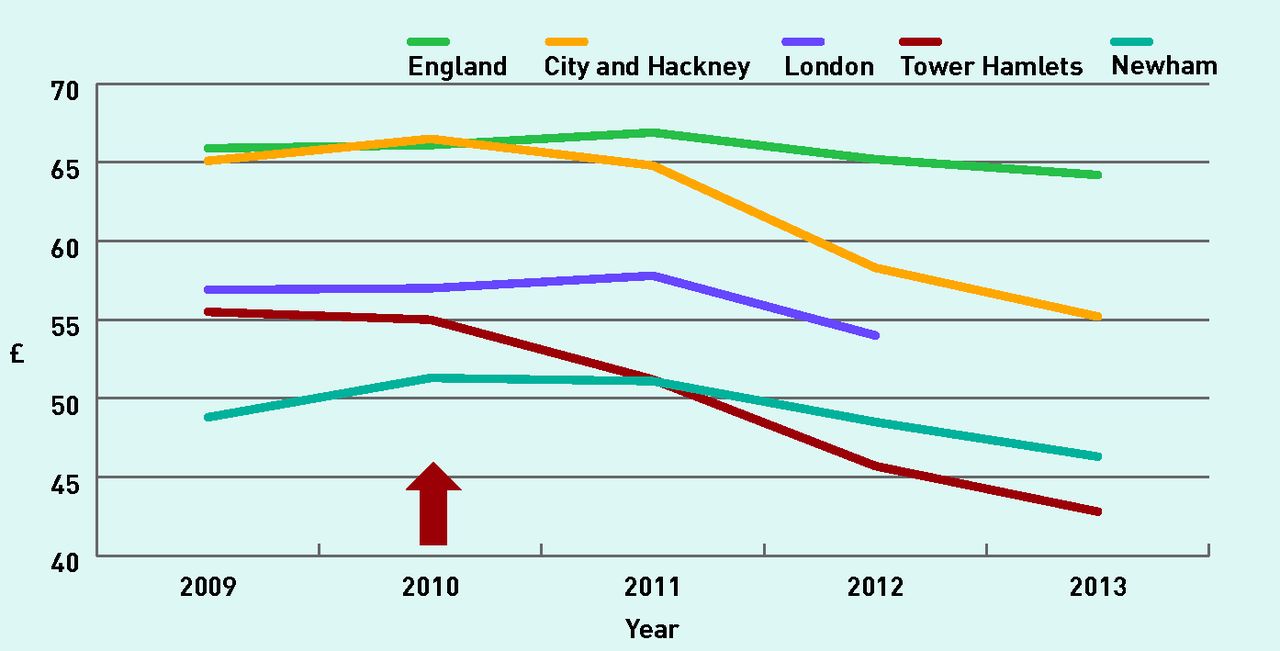
The cost of SMBG per head for people with diabetes in 2009–2010 was £55.00 and £66.50 in Tower Hamlets and City and Hackney respectively, reducing in 2012–2013 to £42.80 and £55.20, the latest date for which comparative data were available, a reduction of £12.20 and £11.30 per head of diabetes respectively (combined £11.70 from £60.40 to £48.70) (Figure 3). In comparison, costs in England reduced by £1.00 from £65.20 to £64.20 and in Newham by £5.00, from £51.30 to £46.30. Thus, the per capita cost of diabetes prescribing had reduced in relative terms by 28.5% and 20.4% in the two intervention CCGs respectively (19.4% combined), compared with England 1.5% and Newham 9.7%.
{kind=link}
{kind=link}
{kind=link}
Total diabetes (type 1 and type 2, including insulin) cost per capita for self-monitoring strips (data for London 2013 was not available). The red arrow marks the start of the intervention.
CCG = clinical commissioning group.
From 2010 to 2013, 20% (3865 out of 19 602) fewer patients with type 2 diabetes used SMBG in the intervention CCGs. Costs relating to the intervention comprised approximately £2000, spent on the production and mailing of guidance and audit results, and £10 000, which was spent on remunerating those who extracted the data and produced the reports.
DISCUSSION
Summary
Over 4 years, the proportion of people not treated with insulin who were prescribed SMBG was significantly reduced in the two intervention CCGs compared to the control CCG. There was also a significant reduction in the number of people on no treatment and metformin using SMBG in all three CCGs. The proportion of patients using SMBG in the two intervention CCGs in 2013, compared with 2010, fell by almost a fifth.
From 2009, the year preceding the intervention, to 2012, the total cost of SMBG (both type 1 and type 2 diabetes, including insulin) fell in the intervention CCGs but increased in the control CCG. The per capita cost of diabetes (type 1 and type 2, including users of insulin) reduced more in the intervention CCGs. The costs for England and Newham, the control CCG, also fell in the same period; as such, the per capita cost of diabetes monitoring strips had reduced in relative terms by 19.4% in the two intervention CCGs, compared with 9.7% in the control CCG and 1.6% in England.
In 2012, all three CCGs were given the results of the programme, which meant that GPs in the control CCG were made aware of the substantial changes that had taken place in the two intervention CCGs in comparison. In 2012, a prescribing incentives scheme aimed at reducing SMBG use was started in Newham; this was responsible for influencing a 5.5% reduction in use in 2012, which was greater than the 3.7% reduction in SMBG use in the preceding 2 years. The diffusion of the intervention into the control group reduced the between-group differences in the fourth year of the programme.
As the total cost of the intervention was £12 000 and savings totalled £62 475, the cost–benefit ratio was 1:5.
Strengths and limitations
To the authors’ knowledge, this is the first programme to evaluate the systematic reduction of inappropriate use of SMBG in people with type 2 diabetes not treated with insulin. A strength of this study is its application to entire local health economies and not simply selected practices. The inclusion of a natural control group strengthens the conclusions although, in the final year, some intervention took place in this control CCG that reduced the between-group differences.
Although data were not obtainable from four practices in one of the intervention CCGs, this is unlikely to have had any appreciable impact on the results as their patient lists represent fewer than 10% of people with type 2 diabetes in City and Hackney CCG.
Although patients in Newham, the control CCG, were slightly younger (67% aged <65 years, compared with 64% in the intervention CCGs), this is unlikely to have had any important impact on the results; differences in types of treatment were accounted for.
However, there is a ‘home advantage’ in that the intervention programme was supported by the university-based Clinical Effectiveness Group, which organised local guideline development and provided audit reports for different types of diabetes treatments using the same web-enabled computer system in almost all the GP practices. This detailed reporting by treatment type is not available through the national ePACT system. Within CCGs, the prescribing of glucose testing strips is almost entirely undertaken by GPs and all prescriptions are electronically recorded.
ePACT is prescription based and does not distinguish between testing strip use for type 1 and type 2 diabetes. This source was regarded by the researchers as indicative of the impact of this intervention on the total cost of SMBG; they are not suggesting that use in type 1 diabetes or those treated with insulin should be reduced.
The engagement of the hospital consultants and diabetes specialist nurses was a key aspect of the success of the programme, as glucose meters were previously given to a wide range of patients free of charge, encouraging a lifetime of use. The researchers recognise that, both nationally and internationally, SMBG monitoring for type 2 diabetes not requiring insulin is highly variable. Neither the literature nor UK NICE guidance supports the routine use of SMBG in people with type 2 diabetes who are at low risk of hypoglycaemia.
Two longer-term trends were apparent when looking at data from 2008 to 2013: the type 2 diabetes register size has increased steadily and differences between CCGs and the reduction in the proportions of people not treated with insulin using SMBG were already apparent before the intervention, with a lower rate of SMBG use in the intervention CCGs. These trends may have been influenced by increasing scepticism among many GPs about routine, untargeted SMBG use and increasing evidence of ineffectiveness following publication of the NICE guidance1 and major studies since 2008.5,12 Differences between CCGs may also reflect local clinical leadership, commercial marketing, and cultural perceptions of patients about the use of technology. Some of the reduction of SMBG use in the intervention CCGs during 2009–2010 may also have been influenced by extensive discussions with local stakeholders that took place on the topic in the year before the introduction of the programme.
Comparison with existing literature
The researchers are aware of one other study that reported reduced frequency of testing, which was achieved without impact on glycaemic control.8 The researchers did not examine HbA1c control in the patients who stopped SMBG or monitor hypoglycaemia; however, in those people known to be at risk of hypoglycaemia, there is a need to improve use of SMBG as it is poorly implemented by both clinicians and patients.25 Hypoglycaemia is a very serious adverse effect of treatment, remains one of the most common causes of admission to hospital from adverse drug effects, and is associated with increased mortality. There is no consistent trial evidence that this is reduced by routine monitoring in type 2 diabetes,12 although it is of importance on a case-by-case basis. Reduction of overtreatment, particularly in older people, may be a more effective strategy to reduce hypoglycaemia.26,27
Implications for practice
This study has demonstrated that inappropriate use of SMBG can be rapidly reduced by a simple and cheap programme, combining education, improved patient reviews, and evaluative motivation. If replicated in other CCGs, the impact on patient use of SMBG, NHS cost, and GP workload would be considerable. If replicated nationally, it is estimated that this would have reduced diabetes prescribing costs in 2013 by £21.8 million and avoided unnecessary testing in 340 000 people. This has positive implications for both patients’ quality of life and the NHS’s workload and financial resources.
Acknowledgments
The authors are grateful to the participating GPs for their cooperation, without which, such studies would be impossible.
Notes
Funding
No specific funding was received for this study. The principal investigator, John Robson, and colleagues Sally Hull, Kambiz Boomla, Jack Dunne, Isabel Dostal, and Rohini Mathur are all employed by the Clinical Effectiveness Group that supports quality improvement in east London, which is funded by the three CCGs: Newham, Tower Hamlets, and City and Hackney. This study constitutes research that is independent of funders.
Ethical approval
Ethical approval was not required as patient-level data are anonymised and aggregated patient data are reported in this study. All GPs in the participating east London practices consented to the use of their anonymised patient data for research and development for patient benefit.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received August 28, 2014.
- Revision requested October 15, 2014.
- Accepted November 4, 2014.
- © British Journal of General Practice 2015
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

