


Abstract
Background In the UK, approximately five people are diagnosed with Hodgkin lymphoma (HL) daily. One-tenth of diagnoses are in those aged >75 years.
Aim To establish a symptom profile of HL and quantify their risk in primary care patients aged ≥40 years.
Design and setting Matched case–control study using Clinical Practice Research Datalink patient records.
Method Putative clinical features of HL were identified in the year before diagnosis. Results were analysed using conditional logistic regression and positive predictive values (PPVs) calculated for the consulting population.
Results Two-hundred and eighty-three patients aged ≥40 years, diagnosed with HL between 2000 and 2009, and 1237 age, sex, and general practice-matched participants were studied. Six features were independently associated with HL: lymphadenopathy (OR 280, 95% confidence interval [CI] = 25 to 3100), head and neck mass not described as lymphadenopathy (OR 260, 95% CI = 21 to 3200), other mass (OR 12, 95% CI = 4.4 to 35), thrombocytosis (OR 6.0, 95% CI = 2.6 to 14), raised inflammatory markers (OR 5.2, 95% CI = 3.0 to 9.0), and low full blood count (OR 2.8, 95% CI = 1.6 to 4.8). Lymphadenopathy per se has a positive predictive value (PPV) of 5.6% for HL in patients aged ≥60 years.
Conclusion Consistent with secondary care findings, lymphadenopathy is the clinical feature with the highest risk of HL in primary care and warrants urgent investigation.
INTRODUCTION
Lymphoma is a cancer of the lymphatic system. Approximately 10% of lymphomas are Hodgkin lymphoma (HL), the remaining being non-Hodgkin lymphoma (NHL). Annually in the UK, more than 1800 people are diagnosed with HL, with 300 deaths.1 It has a bimodal pattern of incidence by age, with a peak at ages 20–24 years and a second peak in females aged 70–74 years and males aged 75–79 years.1 More than 80% of HL cases survive for at least 5 years.2
The UK compares unfavourably with the European average for cancer survival. Between 1995 and 1999, 11% of HL deaths were deemed avoidable.3 The main source of delay in HL occurs during diagnosis: over 40% of HL patients consulted their GP with symptoms three or more times before being referred.4
Current guidance for suspected haematological malignancies lists weight loss, abdominal pain, fever, fatigue, and lymphadenopathy as warranting further investigation. A full blood count, blood film, and inflammatory markers are recommended for people with fatigue or unexplained lymphadenopathy. Immediate investigation is recommended for persistent lymphadenopathy for over 6 weeks, lymph nodes of over 2 cm diameter, increasing size or widespread nature, or accompanied by weight loss, splenomegaly, or night sweats.5
Nearly 87% of HL patients have reported symptoms before their diagnosis, although these have rarely been studied in primary care, the setting in which most patients initially present.6 One primary care study investigated the 15-year period before a lymphoma diagnosis and reported increased infections in HL patients.7 In secondary care studies, painless lymphadenopathy has long been recognised as a feature of lymphoma, with painful lymphadenopathy also recently noted.6 Abdominal pain, fatigue, stomach/ bowel problems, infection, back pain, and pain on drinking alcohol are also reported, although the alcohol-induced pain findings reported almost 50 years ago have not been reliably re-reported.6,8,9 General symptoms, sometimes called B symptoms, of intermittent fever, weight loss, and night sweats are also recognised.10 Associations with anaemia up to 2 years before diagnosis have been reported (OR 1.26, 95% CI = 1.00 to 1.59 per standard deviation reduction from the mean haemoglobin).11
This study aimed to identify and quantify the early clinical features (symptoms, signs, and abnormal investigations) of HL in primary care, with the aim of expediting selection of patients for definitive investigation.
METHOD
This study is part of a project looking at the clinical profile of 13 common cancers among primary care patients aged ≥40 years (see the associated article in this issue).12 The matched case–control design used UK primary care electronic patient records from the Clinical Practice Research Datalink (CPRD). The CPRD contains anonymised patient data collected from over 680 general practices, covering 8.8% of the UK population. Data include primary care clinical events such as symptom reporting, investigations, diagnoses, prescriptions, and specialist referrals. The CPRD applies stringent quality standards for data entry.
How this fits in
Over 40% of patients with Hodgkin lymphoma (HL) visit their GP three or more times before being referred to a specialist. Lymphadenopathy is a known feature of HL and a primary indicator for referral in the National Institute for Health and Care Excellence guidance for haematological cancer, though based on little primary care research. In this study patients aged ≥60 years with lymphadenopathy have a 5.6% risk of having HL. The current guidance advising a 6-week wait for unexplained lymphadenopathy may be unnecessarily long.
Cases and controls
A list of 172 lymphoma codes (available from authors) was collated with 29 codes applied to HL. Cases were selected if aged ≥40 years and diagnosed with HL between January 2000 and December 2009. Up to five age, sex, and, practice controls were matched to each case. The first HL code was taken as the date of diagnosis. The index date for controls matched their case’s diagnosis date. Exclusion criteria were cases with NHL, mycosis fungoides, or Sézary syndrome and their matched controls; any case or control with <1 year of records before the index date; cases without controls; controls with HL; and controls who had not sought medical care after registration.
Selection of putative clinical variables
A list of potential HL clinical features (symptoms, signs, and abnormal investigations) was compiled from existing literature and online patient support group threads. Google Scholar, PubMed, and EBSCO were used with the search terms ‘Hodgkin lymphoma symptoms’, ‘Hodgkin lymphoma primary care’, and ‘early signs/indications/symptoms of Hodgkin lymphoma’. Over 100 000 medical codes are recorded in the CPRD; several relevant codes relate to each feature, which were collated into symptom libraries. Instances were identified in the year before the index date, and variables found in at least 2% of cases were retained. Recording bias was tested on a condition thought to have no association with HL: varicose veins. Abnormal investigation results were defined as the patient having a test value falling outside their local laboratory’s normal range. Patients with a normal laboratory result were grouped with those without testing.
Composite variables
Some tests were grouped together.13,14 The raised inflammatory markers variable included any of: abnormal erythrocyte sedimentation rate, plasma viscosity, or C-reactive protein. Abnormal liver function tests reflected a raised value of any of the hepatic enzymes. Low full blood count included any of: low haemoglobin, low white cell count, or low platelets. Three categories of mass variables were compiled. First, masses in the head or neck incorporating cervical lymphadenopathy were identified; next, masses labelled as lymphadenopathy were identified (this included generalised lymphadenopathy and lymphadenopathy with no site mentioned); finally, all masses from elsewhere in the body were included as ‘other mass’. Exact information relating to the size, location, or duration of mass was unavailable. To indirectly estimate the duration of a patient reporting a mass variable (duration is rarely recorded, so direct measurement was impossible), the first and last report of any of the three mass variables in the year before diagnosis was identified. Those masses having an apparent duration of at least 42 days were reported in a sub-analysis (42 days is the duration of lymphadenopathy recommended for investigation in current NICE guidance).5
Analysis and statistical methods
The main form of analysis was conditional logistic regression.13,14 Non-parametric methods were used as the data were not normally distributed. Univariable analysis was performed on all features present in at least 2% of either cases or controls. Those features associated with HL at P≤0.1 were then grouped into small clinically coherent groups (such as back pain, abdominal pain, and chest pain) for multivariable analyses. Those variables with an association at P≤0.05 entered the final stage of modelling, with a P-value threshold of 0.01 used for retention in the final model. Variables omitted at these earlier stages were checked against the final model, and restored if a likelihood ratio test comparing the models had P≤0.01. Clinically plausible interaction terms were added to the final model and retained if their P-value was also ≤0.01.
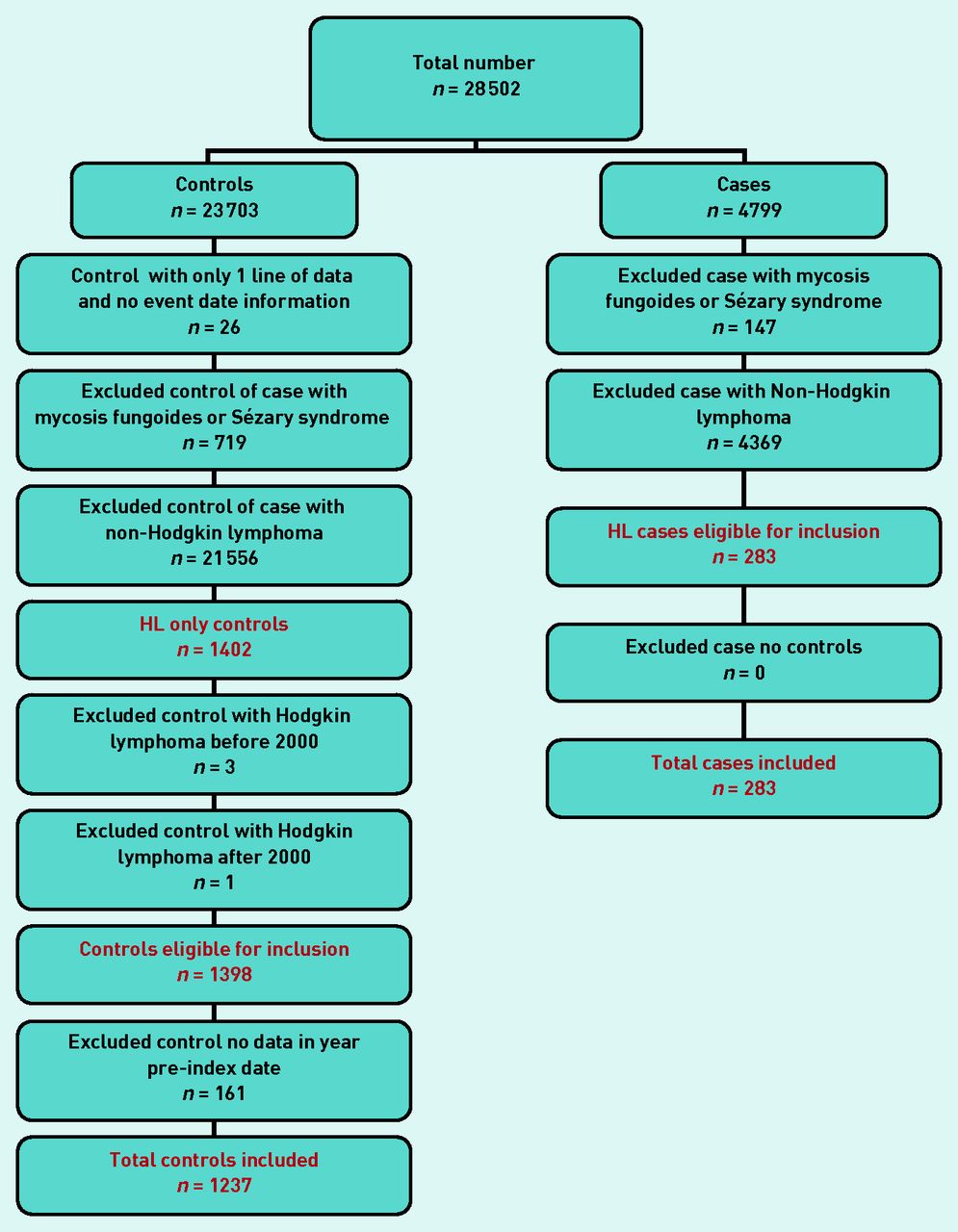
Risk estimates in the form of positive predictive values (PPVs) were calculated using Bayes’ theorem (prior odds × likelihood ratio = posterior odds). Prior odds were calculated from the age-specific national incidence of HL for 2008, expressed as odds. PPVs for pairs of features and repeated attendances for the same feature were calculated where indicated. PPVs were estimated for consulting patients only; thus, the posterior odds were divided by 0.885 as 161 (11.5%) of 1398 eligible controls were non-consulters (Figure 1).

{kind=link}
Hodgkin lymphoma exclusion data.
No sub-analysis by histological subtype was possible because of the small sample size.
Power calculation
Because of the fixed number of participant numbers received from the CPRD (300 cases and 1350 controls), power calculations were used instead of sample size calculations. The numbers provided >86% power (5% two-sided alpha) to detect a difference in a rare variable present in 4% of cases compared with 1% of controls. For a more common variable, the study had >83% power to detect a change in prevalence of 20% in cases and 13% in controls. Data analysis was conducted using Stata software (version 13.1).
RESULTS
The CPRD provided 28 502 patients (4799 cases; 23 703 controls). This included all subtypes of lymphoma cases and their controls. Application of the exclusion criteria is shown in Figure 1, leading to a final number of 1520 in this study (283 HL cases; 1237 controls).
Patient demographic and consultation information is given in Table 1. Cases consulted significantly more frequently than controls in the year before diagnosis (P≤0.001; rank-sum test).
Patient demographics and consultation rates in the year before diagnosis
Clinical features
Forty-three symptoms and 22 abnormal test results were considered initially. Six remained significant in the final model: lymphadenopathy, head and neck mass not described as lymphadenopathy, other mass, thrombocytosis, raised inflammatory markers, and low full blood count. Their frequencies, univariable likelihood ratios, and multivariable odds ratios are shown in Table 2. Of the three B symptoms reported with lymphoma—fever, sweating, and weight loss-sweating and weight loss were common enough to proceed to multivariable analysis. There were only three (1.1%) cases and six (0.5%) controls with recorded fever. The proportion of patients with varicose veins did not differ between cases and controls (P<0.62) — suggesting any recording bias was minimal. In total, nine (2.1%) cases and zero controls had multiple consultations with one of the mass variables at least 42 days apart. No interaction terms, including with sex, were found. From the 283 cases, 187 (66%) had at least one of the final model features from Table 2 recorded.
Features of Hodgkin lymphoma (all ages)
Positive predictive values
PPVs were not calculated if fewer than five cases had the feature. The PPV figures for those aged ≥60 years are presented here, for two main reasons. First, they formed most of the cohort (mirroring the expected epidemiology); second, an over-60s Risk Assessment Tool for NHL has been published (see the associated article in this issue).12 By estimating figures for the same age group, the PPV values can be added together to give estimated risks for each symptom. Where fewer than 10 cases or controls had the combined features, CIs were omitted. In those aged ≥60 years, lymphadenopathy, head and neck mass, and other mass as single symptoms had PPVs of 5.6%, 2.3%, and 0.03%, respectively. Lymphadenopathy combined with a low full blood count or raised inflammatory markers produced PPVs of 2.5% and 2.2%, respectively. Thrombocytosis as a single feature produced a small PPV of 0.04% (95% CI = 0.02 to 0.07). The remaining PPVs were either under 0.05% or could not be calculated because of small numbers.
DISCUSSION
Summary
This is the first study to identify and quantify the clinical features of primary care HL in patients aged ≥40 years. Three symptoms and three abnormal investigations were associated with HL in the whole cohort. The highest risk estimate for HL in those aged ≥60 years was lymphadenopathy, although masses elsewhere in the body had lower risks. Using the whole cohort, risk estimates were between 0.9% and 2.8% when combining raised inflammatory markers or low full blood count with the three mass variables.
Strengths and limitations
This study is the first to investigate the primary care features of HL patients, separately from NHL, in the year before their cancer diagnosis. By doing so, important differences in symptom profiles could have been identified (although no surprising differences were identified). Equally, it is possible to sum the PPVs within the same age band, to give an overall ‘lymphoma risk’ for specific features. The advantage of using CPRD data is well known.15,16 The data are generalisable and representative of the UK population. The comprehensive methods used here for identifying putative features of HL, including use of online support forums to search for patient-reported symptoms, mean it is unlikely that relevant features were omitted. Furthermore, the study’s primary care setting is important. The clinical problem of whom to select for cancer investigation resides in primary care, so requires primary care research.
This study is part of a programme looking at the cancer prodrome in primary care patients aged ≥40 years. The starting age of 40 years was chosen for two reasons. First, for most cancers, the median age of cancer diagnosis is in the early 70s. Additionally, cancer in those aged <40 years disproportionately represents familial syndromes, with the possibility of atypical presentations. Thus the programme as a whole selected a lower age of 40 — a figure that has been problematic only for HL and testis. Despite this, there is no published evidence to suggest that the clinical features of HL differ by age, although this remains a possibility. Survival from HL is superior in the young, although this does not equate to them having a different symptom profile.17 The present sample was relatively small, thus precluding any sub-analysis and restricting the number of risk estimates which it was possible to reliably generate. Data recording may not be consistent among GPs, although this is somewhat mitigated through the limited number of codes available to the GPs, who generally selected a particular ‘dominant’ code for each symptom. Additionally, relevant clinical information can be recorded in a hidden ‘free text’ section, opening up the possibility of preferential recording for cases over controls.18 Cases have more opportunities to report symptoms because of their higher consultation pattern; however, the present test for recording bias did not support this. Finally, as in previous studies, the problem of estimating PPVs from a case–control study design was overcome by calculating the prior odds of HL from registry data.13,19
Comparison with existing literature
Consistent with secondary care literature, the main finding here was lymphadenopathy as conferring the highest risk for HL; head and neck masses had a lesser but considerable association.6,20,21 These results are concordant with those found in the associated article on NHL.12 Cervical lymphadenopathy in primary care has been investigated in three previous studies.22–24 In the first, no malignancies were found from a group of 80 primary care patients with lymphadenopathy, 44% of whom had isolated cervical node enlargement.24 A second study of 249 patients also found no malignancies, and in most patients no final diagnosis was established.22 These two studies had younger patients; in such patients, lymphadenopathy of infectious origin will predominate. The large PPVs in the present study were seen only in those aged ≥60 years, when infection becomes relatively less important. The third study examined GP referrals for lymph node biopsy. Twenty-nine malignancies were found in 82 referred patients, with a prior probability for lymphadenopathy presenting to primary care of 1.1% calculated from these results.23 All three studies emphasised the ability of GPs to identify lymphadenopathy of malignant origin. An association with anaemia has been reported previously in the secondary care literature.25
No association was found with the so-called B symptoms — this may simply reflect the relatively small sample size, or the exclusion of the younger patients. This is part of a bigger problem in cancer diagnostic research: the symptoms that span several possible cancer sites, such as weight loss or thrombocytosis. At a single cancer site level the risk may be small (even so small that it cannot be identified), but across cancer as a whole it may be important. To study these features, cohort studies starting with the symptom are required; this has been done for jaundice and hypercalcaemia, and is under way for thrombocytosis.26,27
Implications for practice
The main finding in this study is the importance of lymphadenopathy and head and neck masses. When combined with NHL, the risks with these symptoms are high, and warrant serious consideration of lymphoma. It was not possible to examine persistence of the mass directly, as duration of symptoms is poorly recorded in medical records including the CPRD.28 The proxy for duration, two mass codes 6 weeks apart, had a PPV of 1.3% (0.0 to 94), in those aged ≥60 years. The word ‘unexplained’ is used in referral guidance, including the latest revision.5 As with the associated NHL article in this issue,12 it is likely that many of the masses were unexplained, as GPs prefer to document diagnoses where possible. Thus, much of the ‘explained’ lymphadenopathy may well be unrecorded.
When the results of this study are added to those for NHL in the associated article,12 the PPVs rise to 18.6% for either NHL or HL for lymphadenopathy, 4.6% for head and neck mass, and 1.1% for other mass elsewhere. Thus the risk estimates for the three mass variables indicate that the default decision should be referral of patients aged ≥60 years with lymphadenopathy or a head and neck mass, unless there is a clear alternative explanation.
Lymphadenopathy and head and neck masses in adults aged ≥60 years are strong predictors of both HL and NHL, and warrant urgent investigation, particularly if they have been present for ≥6 weeks. No blood test or other symptoms change that. This largely accords with current guidance, although it could be argued that the need to wait 6 weeks — to allow resolution or an alternative diagnosis to emerge — is unnecessarily long.
Acknowledgments
The authors would like to acknowledge the contribution to the research presented in this paper made by the Discovery Programme Steering Committee comprising: Roger Jones (chair), Jonathan Banks, Alison Clutterbuck, Jon Emery, Joanne Hartland, Sandra Hollinghurst, Maire Justice, Jenny Knowles, Helen Morris, Tim Peters, Greg Rubin.
Notes
Funding
This article presents independent research funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research Programme (Grant Reference Number RP-PG-0608-10045). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health. Fiona M Walter is part-funded by a NIHR Clinician Scientist award. Richard D Neal is part-funded by Public Health Wales and Betsi Cadwaladr University Health Board.
Ethical approval
Independent Scientific Advisory Committee — protocol 09-110.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
William T Hamilton is clinical lead on the ongoing revision of the NICE guidance on investigation of suspected cancer. His contribution to this article is in a personal capacity, and is not to be interpreted as representing the view of the Guideline Development Group, or of NICE itself. Peter W Rose reports personal fees from GP Update Ltd, outside the submitted work. All other authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received October 22, 2014.
- Revision requested January 8, 2015.
- Accepted January 23, 2015.
- © British Journal of General Practice 2015
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

