


Abstract
Background Selection of primary care patients for investigation of potential oesophagogastric cancer is difficult, as the symptoms may represent benign conditions, which are also more common.
Aim To review systematically the presenting features of oesophagogastric cancers in primary care, including open-access endoscopy clinics.
Design and setting Systematic review and meta-analysis.
Method MEDLINE®, Embase, the Cochrane Library, and CINAHL were searched for studies of adults who were symptomatic and presented in primary care or open-access endoscopy clinics. Exclusions were being asymptomatic, screening, or recurrent cancers. Data were extracted to estimate the diagnostic performance of features of oesophagogastric cancers and summarised in a meta-analysis.
Results Fourteen studies were identified. The strongest summary sensitivity and specificity estimates were for: dyspepsia 0.42 (95% confidence interval [CI] 0.29 to 0.56) and 0.48 (95% CI = 0.31 to 0.65); pain 0.41 (95% CI = 0.24 to 0.62) and 0.75 (95% CI = 0.51 to 0.89); and dysphagia 0.32 (95% CI = 0.17 to 0.52) and 0.92 (95% CI = 0.81 to 0.97). Summary positive likelihood ratios (LR+) and diagnostic odds ratios were: dyspepsia 0.79 (95% CI = 0.55 to 1.15) and 0.65 (95% CI = 0.32 to 1.33); pain 1.64 (95% CI = 1.20 to 2.24) and 2.09 (95% CI = 1.57 to 2.77); and dysphagia 4.32 (95% CI = 2.46 to 7.58) and 5.91 (95% CI = 3.56 to 9.82). Corresponding LR+ were: anaemia 4.32 (95% CI = 2.64 to 7.08); nausea/vomiting/bloating 1.07 (95% CI = 0.52 to 2.19); reflux 0.78 (95% CI = 0.47 to 1.78) and; weight loss 5.46 (95% CI = 3.47 to 8.60).
Conclusion Dysphagia, weight loss, and anaemia show the strongest association but with relatively low sensitivity and high specificity. The findings support the value of investigation of these symptoms, but also suggest that, in a population of patients who are low risk but not no-risk, investigation is not currently recommended.
INTRODUCTION
More than 15 000 new diagnoses of oesophageal or gastric cancers are made annually in the UK. From a diagnostic viewpoint, the two cancers are generally considered together, as the main diagnostic test, upper gastrointestinal endoscopy, is the same for both. For both cancers, 5-year survival is relatively poor, as many are diagnosed at an advanced stage. Diagnostic delays are common, with 29% and 36% of patients with oesophageal and gastric cancer respectively having three or more primary care consultations before diagnosis;1–3 furthermore, 22% and 33% of patients are diagnosed with oesophageal and gastric cancer respectively following emergency presentation.4
An estimated 600 deaths in the UK from oesophagogastric cancer annually are deemed ‘avoidable’ by comparison with mean European figures.5 Expedited diagnosis may be beneficial either by identifying the tumour at a less-advanced stage, or by avoiding the emergency presentation, with its extra mortality.6 Two main prospects for expediting the diagnosis (in the absence of screening) are:
improved selection of patients for endoscopy (investigate ‘smarter’); or
liberalisation of endoscopy recommendations (investigate ‘more’).
The latter may help: UK general practices with a high gastroscopy rate have lower emergency admission rates and mortality for oesophagogastric cancer.7
The main recommendations for endoscopy are those of the National Institute of Health and Care Excellence (NICE), which cover two topics: dyspepsia8 and cancer diagnosis.9 Much of the evidence behind these recommendations came from secondary care. In contrast, here the authors sought to use primary care evidence in a systematic review of the diagnostic performance of oesophagogastric symptoms and likelihood of cancer, as it is in primary care that the clinical problem exists.
METHOD
Data sources and search methods
With the OVID platform, comprehensive searches of electronic databases were conducted using:
MEDLINE® (1950 to May 2014);
Embase (1974 to May 2014);
CAB Abstracts (1973 to May 2014); and
MEDLINE In-Process (May 2014).
The Wiley interface was used to search the Cochrane Library (Database of Reviews of Effectiveness, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, May 2014); and CINAHL (1998 to May 2014). The terms were used to:
identify upper gastrointestinal neoplasia;
identify common symptoms, for example, dyspepsia, dysphagia, reflux, weight loss, pain, vomiting, anaemia, haematemesis, and ‘alarm’; and
for primary care settings, including spelling variations.
How this fits in
Oesophagogastric cancer is relatively common in the UK, but most patients are diagnosed late, with a poor prognosis. National guidance for upper gastrointestinal endoscopy is largely based on secondary care data, which will not pertain to the primary care decision on whether or not to refer. Dysphagia, weight loss, and anaemia show a relatively strong association with oesophagogastric cancer even in primary care populations. Each is of relatively low sensitivity, but high specificity. Other features, such as dyspepsia and other types of abdominal pain, were less likely to be associated with cancer. Despite supporting current referral recommendations, these findings also demonstrate that such recommendations miss a group of patients with symptomatic cancer. Any expansion to identify such patients would need rigorous health-economic evaluation.
All sets included Medical Subject Heading (MeSH) and free-text terms, without language restrictions; the search terms are available from the authors on request).
Further searches were made of databases from relevant cancer websites. These were:
European Organisation for Research and Treatment of Cancer: http://www.eortc.be;
National Cancer Institute of Canada Clinical Trials Group: http://www.ctg.queensu.ca;
Cancer Research UK Directory of Funded Research: http://www.cancerhelp.org.uk/trials/trials/; and
UK Clinical Research Network Study Portfolio: http://public.ukcrn.org.uk/search/.
Reference lists of included studies were screened for relevance; personal literature collections and contacts with authors were also used.
Inclusion and exclusion criteria
Diagnostic studies of any design in Westernised countries with well-developed primary and secondary healthcare systems were eligible; as cancer incidence differs in Asian and African countries, where environmental factors may also differ, these were excluded. Eligible studies were those of patients who were:
adult;
symptomatic; and
within primary care or referred by GPs for investigation to secondary care open-access endoscopy clinics.
Patients’ symptom(s) had to be documented. The target condition was upper gastrointestinal (GI) cancers of the oesophagus, stomach, or duodenum of any stage (including carcinoma in situ). Lymphomas were excluded, as were studies of:
individuals who were asymptomatic;
screening;
recurrent cancers;
secondary causes of upper GI symptoms (from drug therapy and cancer treatment); and
patients referred from secondary or tertiary care for endoscopy.
Study selection
One researcher ran the electronic searches and screened all titles and abstracts against inclusion and exclusion criteria. All potentially relevant abstracts were then reviewed independently by two researchers. Any disagreements including the healthcare setting were resolved by consensus; if uncertainty remained, the full article was obtained to assess its eligibility. Full articles of included studies were obtained and reference lists of all studies were checked for eligibility.
Data extraction and quality assessment
Definitions of dyspepsia (Appendix 1) and ‘alarm’ symptoms varied across studies, increasing clinical heterogeneity. Similar symptoms reported with different synonyms were grouped where possible (Box 1). In some studies, several discrete symptoms were reported;10–16 these were collated separately.
Symptoms grouping
| Classification for analysis | Symptom(s) reported |
|---|---|
| Dysphagia | • Dysphagia |
| Dyspepsia | • Dyspepsia |
| Reflux | • Regurgitation, heartburn, reflux-like symptom |
| Pain | • Upper abdominal pain, epigastric or retrosternal pain, cardiac-like symptom, ulcer-like symptom |
| Weight loss | • Weight loss, appetite loss, anorexia |
| Anaemia | • Anaemia, low haemoglobin, gastrointestinal bleeding |
| Haematemesis | • Haematemesis, if reported separately from anaemia |
| Nausea/vomiting/bloating | • Nausea, vomiting, bloating, dysmotility-like symptom |
| Bloating | • Abdominal distension, bloating, dysmotility-like symptom |
Diagnostic accuracy methods with symptoms representing ‘tests’ were used to predict oesophagogastric cancer. Symptoms could be recorded by the clinician, self-reported by questionnaire, or coded. Valid reference standards were endoscopy, histology, double contrast barium meal, cancer registration, or clinical follow-up of 1 year.
Data extraction was conducted by one researcher and checked independently by a second researcher. The authors were contacted for further information when necessary. Methodological quality of full text included articles was ascertained using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool at the study level.17 One question, relating to the adequacy of the description of symptoms, was added to the QUADAS and one question on the presence of clinical information was removed; as symptoms were used as a ‘test’, it was assumed that clinical information was available.
Data synthesis and analysis
The authors completed 2×2 contingency tables using the counts of true–positives, false–positives, true–negatives, and false–negatives for each symptom. Review Manager (version 5.2) was used for data collation and Stata (version 12) to analyse diagnostic performance with bivariate mixed-effects binary regression modelling, in line with the findings of Reitsma et al.18 Sensitivity, specificity, positive and negative likelihood ratios (LR+, LR−), and diagnostic odds ratios (DORs) were calculated as outcome measures. Univariate random effects meta-analysis of DORs were used to explore heterogeneity between studies. Summary receiver operating characteristic (SROC) curves were generated for each symptom when four or more studies were available.
Heterogeneity was examined from Forest plots of DORs of individual studies, subgrouped by study design (primary care referrals to endoscopy clinics and national database studies); if heterogeneity was observed, subgroups were compared. For symptoms without heterogeneity by study design, outliers were examined using bivariate box plots of sensitivity–specificity pairs, and sensitivity analyses were performed excluding outliers.
Analysis of possible factors influencing heterogeneity between studies (such as prospective versus retrospective designs, clinic settings, and sample sizes) was planned by univariable meta-regression, when ≥10 studies of each symptom were available. The effects of QUADAS items scoring <50% were assessed by univariable meta-regression, comparing the ratio of DORs across all studies meeting a criterion versus not met or unclear.
RESULTS
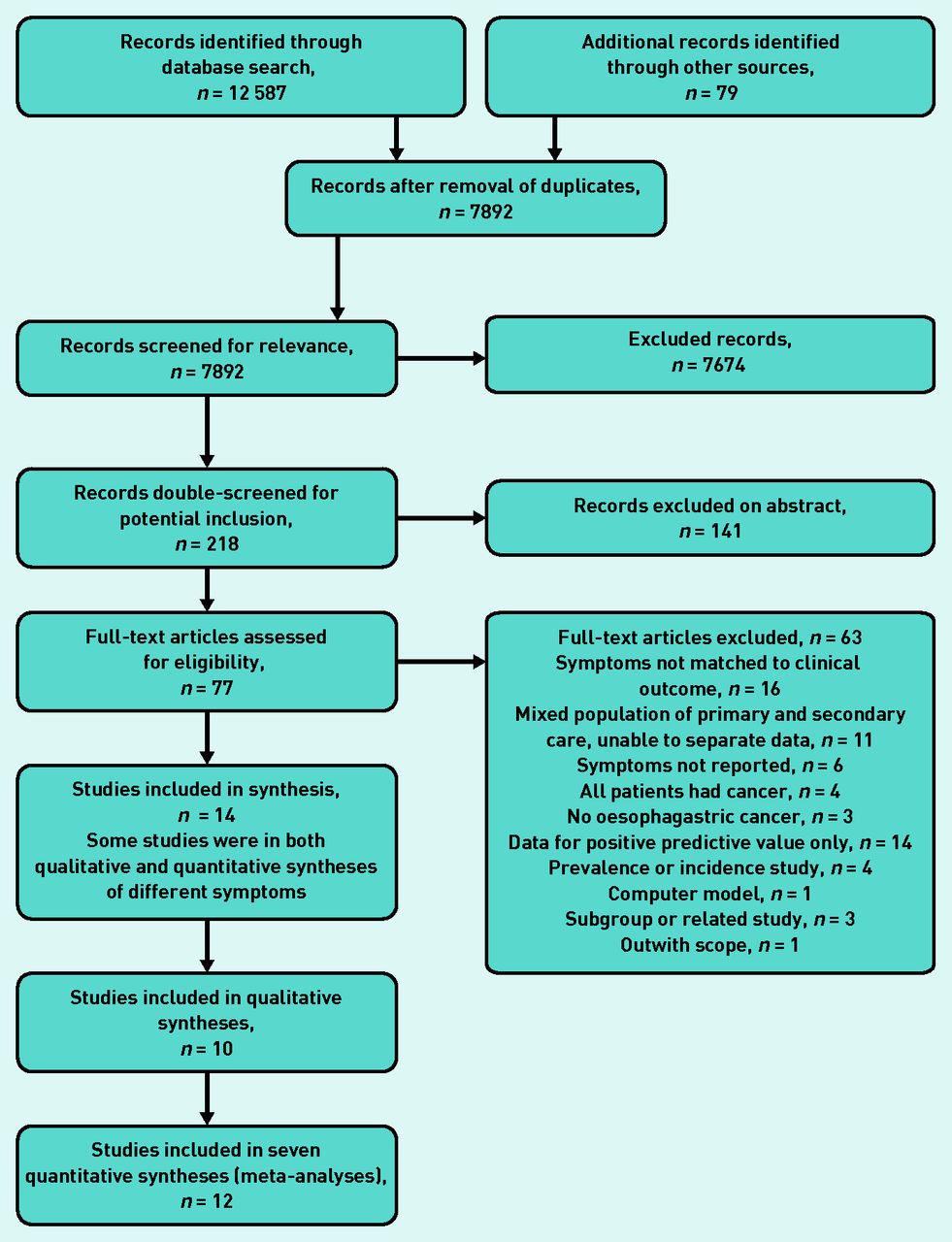
The electronic searches identified 7892 records after de-duplication; one additional study was identified from reference lists. In total, 77 studies were obtained for appraisal and 14 met inclusion criteria for evidence syntheses (Figure 1).

Flowchart of study inclusion.
More than 22 600 participants were recruited in primary care cohort studies; another 3 142 582 participants were identified from three large retrospective studies using primary care databases. Study characteristics are shown in Appendix 2. Most originated in the UK (n = 6) or Europe (n = 7), and one was from Canada. Eight studies were prospective, two involved consecutive samples, and four were retrospective, including three national database studies. Sample sizes ranged from 100 to 10 061 in prospective and consecutive studies; and from 1000 in a locally-based retrospective study to between 40 348 and 2 140 194 in three database studies.
All studies except those of the national databases were of primary care referrals to endoscopy clinics; henceforth termed endoscopy clinic studies. The point prevalence of oesophageal and gastric cancers ranged from 0.08% to 7.14%, with a median 0.68% (Appendix 2). Studies were conducted between 1985 and 2010; data collection varied between 6 months and 129 months.
Heterogeneity
Methodological heterogeneity due to the presence of the database studies10,11,16 was found for dysphagia, dyspepsia, reflux, and nausea/vomiting/bloating; conversely, no heterogeneity for anaemia, weight loss, or pain was identified. As the databases reported stronger diagnostic performance than small studies when heterogeneity between study designs was present, meta-analyses of the smaller studies, representing endoscopy clinics separately, was performed. There were insufficient studies to examine publication bias or to conduct meta-regression analyses.
Anaemia
Anaemia was reported in seven studies evaluating over 3 million patients.10,11,13,15,16,19,20 It was defined as a recorded haemoglobin of <11 g/dl over the previous year in two studies10–11 and grouped with gastrointestinal bleeding in another.15 Sensitivity of anaemia for oesophagogastric cancer was low, with high specificity; LR+ ranged between 1.32 and 8.33, excluding one study20 where few patients presented with anaemia, cancer was rare, and most patients were aged <50 years (Table 1).
Sensitivity, specificity, LR+, and LR− of symptoms associated with oesophagogastric cancer
LR− estimates were close to 1.00. The area under the curve (AUC) of 0.50 (95% confidence interval [CI] = 0.45 to 0.54) indicates poor discrimination of anaemia for oesophagogastric cancers. However, summary estimates for specificity (0.97), LR+ (4.32), and DOR (4.79) suggest that cancer cannot be ruled out (Table 1).
Meta-analysis of the studies in endoscopy clinics found a statistically significantly lower DOR (Table 1). No outliers were present from a bivariate box plot. Removing two endoscopy clinic studies13,20 with no cancers identified moderately increased the summary sensitivity to 0.16 (95% confidence interval [CI] = 0.10 to 0.26, data not shown).
Pain
Pain was grouped to include upper abdominal, epigastric, retrosternal, cardiac-like, and ulcer-like pain; seven studies involving over 3 million patients evaluated these symptoms.10–12,14,16,20,21 Studies reporting epigastric or retrosternal pain are reported separately (Table 2). Sensitivity was low with the exception of two endoscopy clinic studies;12,14 specificity varied widely from 0.26 to 0.96. LR+ values were ≤3.04.
Meta-analyses of all studies, and for a subgroup of endoscopy clinic studies, showed poor discrimination of pain for oesophagogastric cancer (Table 1). When three outliers12,14,16 were excluded, the summary sensitivity for pain reduced to 0.28 (95% CI = 0.18 to 0.41, data not shown); other metrics changed little.
Weight loss
Weight loss was evaluated in nine studies of 3 159 817 patients.10–16,19,20 Sensitivity ranged between 0.00 and 0.78, and was <0.50 in two-thirds of studies; specificity was more precise ranging between 0.72 and 0.99 (Table 1). The LR+ ranged between 1.87 and 9.81, with the exception of one study (Table 1).20
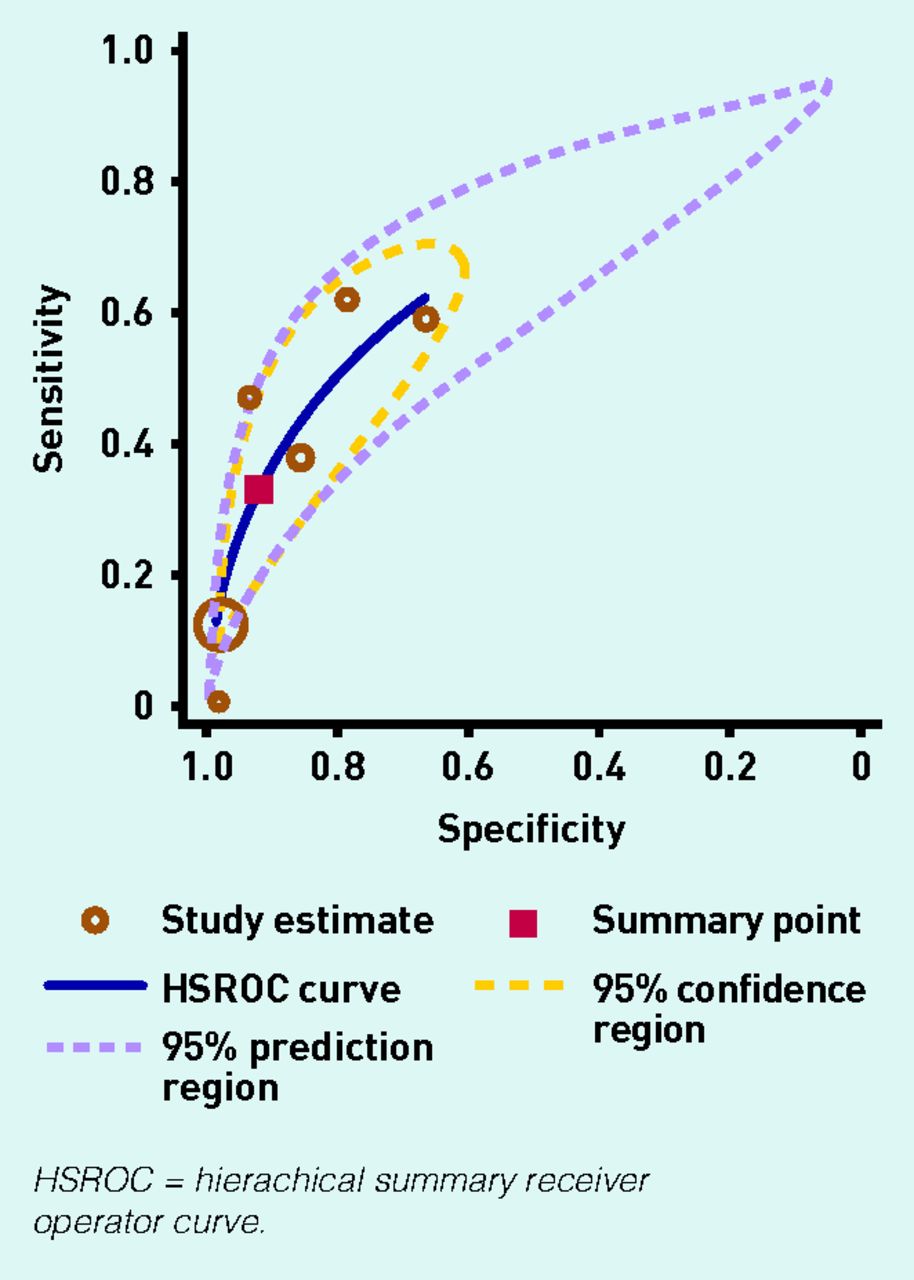
The SROC curve shows some discriminatory value of weight loss to detect oesophagogastric cancer (Figure 2). A meta-analysis of endoscopy clinic studies increased the summary estimate for sensitivity (Table 1).

SROC curve for sensitivity and specificity of weight loss.
One outlier was identified;19 exclusion of this study increased summary estimates of LR+ and DOR (sensitivity 0.24 [95% CI = 0.16 to 0.35], specificity 0.97 [95% CI = 0.94 to 0.98], LR+ 7.13 [95% CI = 5.67 to 8.95], LR− 0.78 [95% CI = 0.70 to 0.87], DOR 9.52 [95% CI = 7.19 to 11.54], data not shown).
Dysphagia
Nine studies reported dysphagia, evaluating over 3 million patients.10,11,13–16,19,20 The sensitivity of dysphagia to detect oesophagogastric cancers ranged from 0.12 to 0.62 excluding one study of few patients presenting with dysphagia (Table 1), and detection of only one oesophageal cancer. Specificity was stronger, ranging between 0.67 and 0.99. LR+ ranged between 1.77 and 7.81 in endoscopy clinic studies, excluding Thomson et al’s study,20 and was much larger from the database studies (Table 1).10,11,16
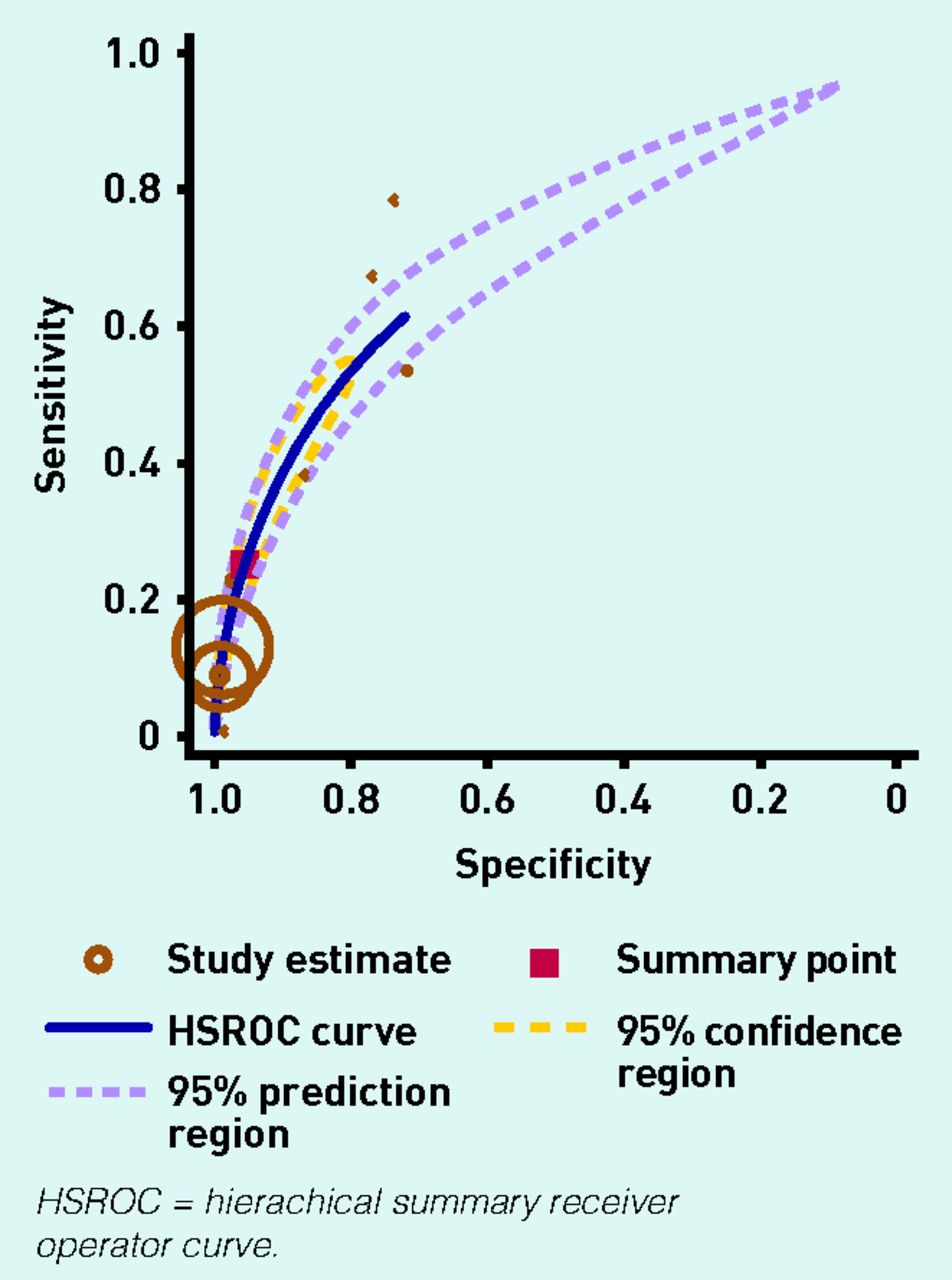
LR− estimates ranged from 0.48 to 0.9 (Table 1). Findings between the databases were consistent. A Forest plot (data not shown) of DORs showed marked heterogeneity between the endoscopy clinic studies and the database studies. An SROC curve for the subgroup of endoscopy clinic studies showed moderate discrimination of dysphagia to detect oesophagogastric cancers with an AUC of 0.68 (95% CI = 0.64 to 0.72) (Figure 3).
SROC curve for sensitivity and specificity of dysphagia.
Dyspepsia
Dyspepsia was reported in seven studies evaluating over 58 000 patients.13–16,22–24 The sensitivity of dyspepsia to detect oesophagogastric cancers ranged from 0.17 to 0.70; however specificity varied across endoscopy clinics, possibly reflecting different dyspepsia definitions and study settings.
LR+ were generally low ranging from 0.45 to 2.55 in endoscopy clinic studies (Table 1), and was strong in one large national database study.16 LR− estimates were low, ranging from 0.62 to 2.34. An AUC of 0.42 (95% CI = 0.38 to 0.46) and summary estimates from meta-analysis of the subgroup of endoscopy clinics suggested low discrimination of dyspepsia for oesophagogastric cancers.
Both low sensitivity and specificity values suggest a weak association of dyspepsia as a sole symptom with oesophagogastric cancers.
Nausea, vomiting, or bloating
This group encompassed the symptoms classified as dysmotility-like; bloating was also collated separately when data was available. Six studies of over 53 000 patients reported any of these symptoms.12,14–16,20–21 The sensitivity was low, ranging from 0.00 to 0.38; specificity varied between 0.56 and 0.99 (Table 1). The LR+ ranged between 0.37 and 1.56 for endoscopy clinics, although it was 6.76 in one database study. An AUC of 0.50 (95% CI = 0.45 to 0.54) and meta-analysis of endoscopy clinics, suggests low discrimination of these symptoms for oesophagogastric cancer.
Reflux
Reflux symptoms were reported as regurgitation, heartburn, and ‘reflux-like’ symptoms in nine studies of over 59 000 patients.12,14–16,20–24 Sensitivity overall was low, ranging between 0.0 and 0.57, excluding the study by Thomson et al because only one patient in the whole series had upper GI cancer (and had reflux); specificity was higher ranging from 0.49 to 0.98. The LR+ were, in the main, <2.00; an exception being one database study (Table 1).16 An AUC of 0.55 (95% CI = 0.50 to 0.59) and summary estimates from meta-analysis of endoscopy clinics suggests low discrimination of these symptoms for oesophagogastric cancers.
Other symptoms
One study from a dyspepsia clinic reported ‘alarm’ symptoms as a single entity;25 these included weight loss, dysphagia, anaemia, and vomiting. Sensitivity was relatively high, although specificity, LR+, and LR− were low in comparison.
Although appetite loss and haematemesis were of low sensitivity, both specificity and LR+ were strong in two national database studies;10,11 the LR+ values of all other remaining symptoms were relatively low, with the exception of one database study reporting an LR+ of 10.2 for epigastric pain (Table 2).16 Diagnostic performance for failure of antacid medication from three studies22–24 showed a low association with oesophagogastric cancer (Table 2).
Sensitivity, specificity, LR+, and LR− of other symptoms associated with oesophagogastric cancer
Quality of studies
The reporting of QUADAS items is shown in Figure 4, with more detail in Appendix 3. QUADAS items met by <50% of studies were:
acceptable delay between index and reference tests; and
blinded interpretation of the index test without knowledge of the reference standard.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Methodological quality graph of proportions of studies for each QUADAS item.
Forty-three per cent of studies were considered not to be representative samples (patients at high risk with alarm symptoms, or a majority of patients aged ≤50 years). Appendix 4 shows the meta-regression of the ratio of DORs, suggesting little evidence of an effect of these factors on the summary estimates; however, heterogeneity between studies was substantial.
DISCUSSION
Summary
This systematic review examined studies undertaken in primary care (including open-access endoscopy clinics) of the features of oesophagogastric cancer. A low sensitivity for detection of these cancers was found in all studies, with the highest sensitivity symptoms being dysphagia, weight loss, dyspepsia, and any pain symptom. From the DORs, all clinical features showed an association with cancer, with dyspepsia and reflux having the weakest associations. However, the LR+s suggest the symptoms of dysphagia, weight loss, and anaemia would be the most useful in the selection of patients for investigation. Pain, nausea/vomiting/bloating, reflux, and dyspepsia were less likely to be associated with cancer.
Each of the clinical features assessed in this review was associated with cancer, with the notable exceptions of dyspepsia and reflux. The strength of the associations varied, with summary DORs highest in weight loss, moderate in dysphagia and anaemia, and lowest for pain and nausea/vomiting/bloating.
Strengths and limitations
Systematic review findings are only as good as the data reported from the candidate studies. The assessment of study quality using the QUADAS tool was adequate across seven of 11 items (63.6%); ratio of DORs showed no effects of study quality on the meta-analyses.
Differences in diagnostic performance between the large database studies (all from the UK) and smaller endoscopy clinic studies were found. The diagnostic performance was consistent across the three database studies; however, LR+s were larger for most symptoms than in endoscopy clinic studies; there are several possible reasons for this. The database studies used coded symptoms in the medical records of confirmed cases of oesophagogastric cancer, and from other patients without cancer. These data are likely to differ from those collected in smaller prospective studies using questionnaires or patients’ self-reported symptoms; these differences may underpin the methodological heterogeneity identified for some symptoms between the databases and endoscopy clinic studies.
The symptoms of anaemia, weight loss, and pain are easier to define uniformly and were unaffected by study design, while more complex symptoms like reflux, dyspepsia, nausea/vomiting/bloating, and dysphagia produced stronger diagnostic outcomes in the databases than endoscopy clinic studies.
Another factor almost certainly influencing investigation decisions, and contributing to clinical heterogeneity, is symptom severity. No studies reported this factor. Similarly it was not possible for the authors of this review to analyse the findings by age or sex, as the data were limited.
Another possible limitation is that some studies of patients who were symptomatic were identified but excluded from the review as none developed oesophagogastric cancer. These studies may represent a different population. Similarly, the prevalence of cancer was as high as 7.14%; again, this is likely to reflect different populations, especially for selection by age criteria.
One methodological improvement may be individual patient data meta-analysis: this would require considerably more resources than the authors had available and the need for authors of included studies to be able and willing to release their patient data.
The decision to report measures of relative association, such as DORs and LRs, followed current best practice. Absolute measures of risk, such as positive predictive values (PPVs), are also useful metrics. However, absolute measures of risk depend not only on the strength of the association between the symptom and cancer, but also on the prevalence of cancer in the study population. This latter parameter varied considerably, despite restriction to primary care, so summary PPV estimates could obscure, rather than enlighten, the strength of association between a symptom and cancer.
Open-access endoscopy clinics were included where the clinical responsibility was retained by primary care. This may have increased the strength of association with oesophagogastric cancer, especially for dyspepsia, as it is unlikely that all patients presenting to primary care were investigated; as a result, those in the endoscopy clinic had undergone a selection process, thereby increasing the population risk.
Gastric and oesophageal cancers were not separated as a pre-hoc decision; furthermore, only two studies did separate these. Some symptoms may be more relevant to oesophageal cancers, especially dysphagia; this is of minor clinical relevance, as the same main diagnostic test is used for both cancers.
Comparison with existing literature
This review overlaps with another systematic review by Vakil et al.26 The review reported here included some of the same studies, but excluded those with mixed cohorts of patients from primary and secondary care for which the data could not be separated. Unlike Vakil et al, study selection was restricted to primary care settings.
The summary sensitivity and specificity values in this review were similar to those of Vakil et al for dysphagia, weight loss, and anaemia, presumably because most patients with these symptoms would be referred. An earlier meta-analysis of eight studies (four included in the current analysis) by Fransen et al 27 reported summary sensitivity and specificity values for weight loss, nausea/vomiting, anaemia, and dysphagia that are comparable to the meta-analyses in this review.
Implications for research and practice
Many of the symptoms reported in this review are found in a range of clinical conditions. It was unlikely that any would exhibit strong specificity; similarly, symptoms are usually not as precise as laboratory measures, because of their subjective nature. However, quantification adds some value, by highlighting the symptoms with the strongest associations with cancer, and comparing relative diagnostic values. It also allows consideration of which symptoms warrant specialist investigation.
Current UK guidance suggests investigation for possible cancer in patients with dyspepsia and additional chronic gastrointestinal bleeding, unintentional weight loss, persistent vomiting, iron deficiency anaemia, or an epigastric mass.8,9 At any age, dysphagia and, in patients aged >55 years, persistent unexplained dyspepsia, are recommended for investigation. The findings of this review clearly support investigation for patients with dysphagia, weight loss, or anaemia.
No studies reported epigastric masses, but investigation appears uncontroversial. For dyspepsia and reflux, the summary diagnostic ORs in this review were close to 1.0 (with upper CIs as high as 2.0); even accepting that some selection bias was introduced by the decision to include open-access endoscopy clinics, it remains clear that these symptoms have a lower association with oesophagogastric cancer.
Nausea/vomiting and abdominal pain represent small risks; the so-called ‘low-risk-but-not-no-risk’ symptoms.28 If recommendations for endoscopy were liberalised to include these, then some cancers would be detected earlier; this would, however, come with a clinical and economic cost, which may be considerable.8
Currently, there is a 2.7-fold difference in the rate of gastroscopy between the highest and lowest clinical commissioning groups, which is hard to justify clinically.29 Even so, a policy decision to expand criteria for investigation would need rigorous health economic evaluation. Nonetheless, if the UK is to narrow the mortality gap with Europe, this is worthy of consideration, alongside improvements in awareness, waiting times, and possible biomarkers and reduced costs of endoscopy. Expecting GPs to exercise ‘better’ selection of patients with existing resources is unrealistic, however, as current guidance already identifies those patients who are most at risk.
Acknowledgments
We would like to thank Professor Julian Higgins for statistical support.
Appendix 1. Definitions of dyspepsia used in included studies
| Study | Definition |
|---|---|
| Boulton-Jones et al 22 | Based on British Society of Gastroenterology guidelines |
| Collins & Altman10 | Dyspepsia not reported |
| Hansen et al 21 | Epigastric or retrosternal pain or discomfort, with or without heartburn, nausea, vomiting, and any other symptom related to the proximal alimentary tract |
| Hippisley-Cox & Coupland11 | Dyspepsia not reported |
| Johannessen et al 12 | No definition |
| Kapoor et al 19 | No definition |
| Melleney & Willoughby25 | No definition |
| Meineche-Schmidt & Jørgensen13 | Pain or discomfort in the abdomen judged by the GP to be related to the gastrointestinal tract |
| Numans et al 14 | Disease history |
| Salo et al 15 | Chronic and recurrent pain, discomfort in upper abdomen, abdominal distension or postprandial upper gastrointestinal complaints |
| Stapley et al 16 | General Practice Research Database coding for dyspepsia or indigestion |
| Thomson et al 20 | Upper gastrointestinal symptom complex characterised by epigastric pain or discomfort, and may include heartburn, acid regurgitation, excessive burping/belching, abdominal bloating, feeling of abnormal or slow digestion, early satiety, or nausea |
| van Kerkhoven et al 23 | Upper abdominal complaints, nausea, vomiting, pain, belching, or fullness |
| Voutilainen et al 24 | Epigastric pain and/or other chronic or recurrent symptoms centred in the upper abdomen (bloating or distension, belching, nausea, or early satiety) |
Appendix 2. Study characteristics
| Study authors | Country | Design | Setting | Age, years | Categories of presenting symptoms | Participants, n Alarm symptoms, % | Prevalence of oesophogeal cancer | Data collection tool | Reference standard |
|---|---|---|---|---|---|---|---|---|---|
| Boulton-Jones et al22 | UK | Retrospective cohort (audit), 1997–1999 (29 months) | GP referrals to open access endoscopy, according to BSG guidance, at a district general hospital | Not reported |
| Total cohort, n = 1000 Single symptom, n = 471 Multiple symptoms, Alarm symptoms 15% | Gastric cancers, n = 8 Oesophageal cancers, n = 9 Prevalence, n = 529 1.70% (95% CI = 0.99 to 2.71) | GP used standard tick-box form listing commonly accepted indications for referral from BSG guidance | Endoscopy and histology |
| Collins & Altman10 | UK | Retrospective cohort, 2000–2008 (90 months) | Primary care validation study of QResearch data using THIN database. Exclusions: history of gastrooesophageal cancer, registration <12 months with practice, invalid dates, aged <30years or ≥85years | Range 30–84 | Alarm symptoms
| Validation set n = 2 140 194 Cases, n = 1256 Controls, n = 2 138 938 Alarm symptoms 100% | Gastric and oesophageal cancers, n = 1256 Prevalence 0.08% (95% CI =0.08 to 0.09) | THIN database | Read Clinical Classification (version 2) |
| Hansen et al 21 | Denmark | Prospective cohort, 1991–1992 (13 months) | 66 GPs in a Danish city referred all patients with dyspepsia, of any severity to open-access endoscopy. Exclusions: upper GI bleeding jaundice, abdominal surgery, previous upper GI surgery | 47 (SD 17) 62%>40 |
| n = 612 Alarm symptoms: unknown | Upper GI cancers, n = 3 Unclassified, n = 1 Prevalence 0.65% (95% CI= 0.18 to 1.67) | Structured interview by endoscopist | Endoscopy and histology when indicated |
| Hippisley-Cox & Coupland11 | UK | Retrospective, cohort 2000–2010 (129 months) | Primary care population of all practices in England and Wales, recorded in QResearch database. Exclusions: history of gastro-oesophageal cancer, registration <12 months with a practice, invalid dates, aged <30years or ≥85years | 50 (SD 15) Range 30–84 | Alarm symptoms
| Validation set n = 963 040 Alarm symptoms 100% | Gastric and oesophageal cancers, n = 986 Prevalence 0.14% (95% CI = 0.13 to 0.15) | QResearch database. Incident diagnosis of gastric or oesophageal cancer >2 years after study entry, recorded in GP record or linked ONS record | ICD-9 or 10 recording of disease classification |
| Johannessen et al 12 | Norway | Prospective cohort, 1985–1987 (18 months) | Mainly GP referrals to open-access endoscopy at a regional hospital. Exclusions: jaundice, upper GI haemorrhage, acute abdominal pain, previous gastric surgery or endoscopy | 50 (SD 15) 67%>40 |
| n = 930 Alarm symptoms: not calculable, >1 symptom/patient | Gastric cancers, n = 9 Prevalence 0.97% (95% CI = 0.44 to 1.83) | Self-administered questionnaire of 112 items including demographic, medical history and present symptoms | Endoscopy and histology if suspicion of malignancy |
| Kapoor et al 19 | UK | Prospective consecutive cohort, 2000–2002 (20 months) | GP referrals of patients at high risk with pre-determined alarm features to rapid access endoscopy according to NHS 2-week rule criteria | Mean 59, range 17–96 63% >55 |
| Evaluation cohort n = 1852 Alarm symptoms: not calculable, >1 symptom/ patient | Gastric cancers, n = 25 Oesophageal cancers, n = 45 Prevalence 3.78% (95% CI = 2.96 to 4.75) | Standardised referral proforma completed by GPs noting the presence/absence of each designated alarm feature | Gastroscopy and histology |
| Meineche-Schmidt & Jørgensen 13 | Denmark | Prospective cohort, 1991–1993 (36 months) | General practice referrals of patients with dyspepsia from 63 centres in Denmark | Range 18– ≥65 74% >38 50% >51 |
| Uncomplicated and complicated cohorts n = 1491 Alarm symptoms 41% | Gastric and oesophageal cancers, n = 8 Prevalence 0.54% (95% CI = 0.23 to 1.05) | Diagnostic chart based on structured interview by GPs; included 18 dyspepsia symptoms and six alarm symptoms. Follow-up by postal questionnaire to GPs | Endoscopy, radiograph, ultrasound |
| Melleney and Willoughby25 | UK | Prospective audit, 1999–2000 (6 months) | ‘One-stop’ unrestricted dyspepsia clinic for GP referrals at single hospital. Proton pump inhibitors and H2-receptor agonists were stopped ≥2 weeks before clinic appointment | Median 59 Range 15–84 | 1. Any alarm | n = 100 (84 analysed) Alarm symptoms 42% | Upper GI cancers, n = 6 Prevalence 7.14% (95% CI = 2.68 to 14.91) | Special referral form designed in consultation with local GP practices | Endoscopy, blood tests and abdominal ultrasound if needed. Histology if endoscopy uncertain |
| Numans et al 14 | Netherlands | Prospective, consecutive cohort, 1986–1988 (25 months) | GP referrals of patients with dyspepsia for first-time gastroscopy at nine hospitals in one city | Not reported |
| Study population n = 861 Alarm symptoms: not calculable, >1 symptom/patient | Gastric and oesophageal cancers, n = 21 Prevalence 2.44% (95% CI = 1.52 to 3.70) | GPs referred patients on basis of disease history and symptoms for endoscopy. Gastroscopy views were reported uniformly | Gastroscopy and histology if suspicion of malignancy |
| Salo et al 15 | Finland | Consecutive cohort, 1998–2000 (24 months maximum) | Primary care referrals to open-access endoscopy in one city | Range 11–93 52% >55 |
| n = 10 061 Alarm symptoms 13% | Gastric cancers, n = 52 Oesophageal cancers, n = 15 Duodenal cancers, n = 1 Prevalence 0.68% (95% CI = 0.53 to 0.86) | Experienced physicians who performed endoscopies interviewed patients. Alarm symptoms considered most. significant when present. gastrointestinal complaints also reported | Endoscopy, Finnish registry, histology |
| Stapley et al 16 | UK | Retrospective matched case–control, 2000–2009 (120 months) | GPRD contains copies of anonymised medical records of participating UK general practices. Exclusions: metastatic, cancers controls who had ever had gastro-oesophageal cancer | Range 40– ≥85 |
| n = 40 348 Cases, n = 7471 Controls, n = 32 877 | Gastric cancers, n = 28 Oesophageal cancers, n = 18 Prevalence not available | GPRD database searched using codes for 18 oesophageal and 28 gastric cancers. Five controls matched on year of birth, sex, and practice; also identified using computer-generated random sequence | GPRD coding for gastro-oesophageal cancers |
| Thomson et al 20 | Canada | Prospective cohort, 1999–2001 (16 months) One of the CADET series of studies | 49 family physician practices across Canada linked to gastroenterology unit referred patients with uninvestigated dyspepsia. Exclusions: patients with heartburn or acid regurgitation as sole symptom, recent Helicobacter pylori eradication, previous endoscopy or radiology | Mean 46, range 18–84 64% of endoscopy patients<50 |
| n = 1040 Alarm symptoms 3% | Oesophageal cancers, n = 1 One patient with dyspepsia had a gastric MALToma, this was not a target condition for the review. Prevalence 0.10% (95% CI = 0.02 to 0.54) | Patients completed 14-item symptom checklist ranking the three most bothersome symptoms | Endoscopy (urea breath test if refuse] and histology |
| van Kerkhoven et al 23 | Netherlands | Prospective, consecutive cohort, 2002–2004 (36 months) | GP referrals for open-access upper GI endoscopy at a single general hospital. Exclusions: age <18 years, failed/previous endoscopy | Mean 54 (SD 15) |
| n = 1298 Alarm symptoms: not calculable, >1 symptom/ patient | Gastric and oesophageal cancers, n = 23 Prevalence 1.77% (95% CI = 1.13 to 2.65) | GPs completed referral indications on standardised form. Endoscopic findings recorded in database | Endoscopy |
| Voutilainen et al 24 | Finland | Consecutive cohort, 1996 (12 months) | GP referrals of patients with dyspepsia for upper GI endoscopy at two hospitals and eight healthcare centres. Exclusions: previous Helicobacter pylori eradication or gastrooesophageal surgery | Mean 58 (IQR 25) |
| n = 3378 Alarm symptoms 33% | Gastric cancers, n = 17 on symptoms, 0.50% Prevalence (95% CI = 0.29 to 0.80) | GPs completed structured questionnaire duration, and medication. Endoscopic data recorded on pre-structured questionnaire | Endoscopy, biopsy and histology. Cancer registries |
BSG = British Society of Gastroenterology. CADET = Canadian Adult Dyspepsia Empiric Treatment. GI = gastrointestinal. GPRD = General Practice Research Database. ICD = International Classification of Diseases. IQR – interquartile range. ONS = Office of National Statistics. SD = standard deviation. THIN = The Health Improvement Network.
Appendix 3. QUADAS item scoring of individual studies.

Appendix 4. Ratio of DOR of low-scoring QUADAS items
| QUADAS item | Studies meeting the criterion, n | Ratio DOR (95% CI) | P-value | Heterogeneity, T2 |
|---|---|---|---|---|
| Representative sample | 8 | 0.40 (0.05 to 3.26) | 0.36 | 2.76 |
| Acceptable delay | 5 | 0.73 (0.08 to 6.96) | 0.76 | 2.67 |
| Blinding of index test | 6 | 0.58 (0.081 to 4.08) | 0.55 | 2.38 |
DOR = diagnostic odds ratio. QUADAS = Quality Assessment of Diagnostic Accuracy Studies
Notes
Funding
This review was funded by Cancer Research UK (grant number A12218). Richard D Neal receives funding from Betsi Cadwaladr University Health Board and Public Health Wales.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
William Hamilton is the clinical lead for the current revision of guidance from the National Institute for Health and Care Excellence (NICE) on the topic of selecting patients for cancer investigation. His contribution to this article is in a personal capacity and is not to be interpreted as representing the view of NICE’s Guideline Development Group, or of NICE itself. He has received travel support to give lectures and attend conferences, plus occasional speaker’s fees from conference organisers in the charitable and educational sector, although none have come from commercial sources. William Hamilton, Peter W Rose, and Richard D Neal were co-authors of one of the articles included in the review. An abstract of an oral presentation of this article is cited in: Eur J Cancer Care 2014; 23(S1): 24–33.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received March 5, 2015.
- Revision requested March 30, 2015.
- Accepted April 9, 2015.
- © British Journal of General Practice 2015
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

