


In England >15 million people have a long-term condition and there are >5.4 million caregivers. Caregivers provide unpaid care by looking after an ill, older, or disabled family member, friend, or partner. The care provided includes aspects of medicine taking, making caregivers important stakeholders in patients’ adherence to prescribed treatments.
We argue that there is a lack of evidence on factors affecting adherence to medications in patients with long-term conditions who are relying on others for medicine taking while living in the community. These patients and their caregivers are often excluded from adherence studies. Clinicians treating non-adherence in these patients therefore lack evidence on which to base their practice.
AN EXAMPLE ANALYSIS OF THE STROKE POPULATION
To illustrate this, we have focused on survivors of stroke as an exemplar of other conditions. We propose a framework of research questions to address this knowledge gap, based on the theory of intentional and non-intentional non-adherence. We believe this framework could be applied to other patient populations who are dependent on others for medicine taking, for example, older patients with physical or cognitive impairments suffering from hypertension, type 2 diabetes, and other cardiovascular diseases, or patients suffering from severe psychiatric disorders/neurodegenerative diseases.
FACTORS AFFECTING MEDICATION ADHERENCE IN STROKE
Stroke recurrence is associated with higher disability and mortality than first-time stroke, and accounts for one-third of all events. Secondary prevention medicines can reduce risk of recurrence by three-quarters,1 making medicine taking an important daily activity in this patient group. Adherence studies have so far concentrated on those survivors of stroke who are responsible for their own medicine taking. They have revealed that absence of concerns about medications, knowledge of side effects, clear understanding of the consequences of non-adherence, and good routines of taking medications minimise non-adherence.2 Interventions aimed at these factors have indeed shown promising results.3
LACK OF INVOLVEMENT OF PEOPLE WITH SIGNIFICANT DISABILITY AND CAREGIVERS IN ADHERENCE RESEARCH
A recent systematic review of trials to improve adherence to blood pressure tablets after stroke found that survivors of stroke with significant physical, communication, or cognitive impairments were excluded from most studies, including eight ongoing studies.4 Caregivers were included in only a minority of trials and their degree of involvement was not reported. These excluded groups represent an important population.
The percentage of survivors of stroke with severe disability ranges between 17% in the 65–74-year-olds, 25% in the 75–84-year-olds, and 45% in those >84 years.5 A third of all people who have suffered stroke have difficulty with communication6 and at least a fifth have cognitive impairment (MMSE score <24).7 People with stroke of all ages may experience deficits in short-term memory and comprehension.8,9 Overall, 400 000 to 600 000 survivors of stroke in the UK suffer from severe physical, communication, and cognitive impairments. These disabilities make it difficult for survivors of stroke to participate in research, including providing informed consent and completing questionnaires and interviews. Perhaps for these reasons, survivors of stroke with severe disability are often excluded from studies of adherence,4 even though they have the capacity to participate.10 However, ways are emerging to allow patients with severe disability to take part in research.11 For people who lack mental capacity, inclusion in research studies in the UK can be obtained through personal consultees or nominated consultees, according to the Mental Capacity Act 2005.12
There is evidence that disability and impairment in mobility and communication decrease medication adherence in patients suffering from hypertension.13 Deficits in attention, mental flexibility, or working memory have been linked with non-adherence to medications in other patient groups.5
THE IMPORTANCE OF CAREGIVERS
Although the exact percentage of survivors of stroke relying on caregivers for some or all aspects of medicine taking is not known, around half of survivors of stroke are dependent on others for everyday activities.14 Caregivers of older patients have reported difficulties with tablet administration.15 A postal questionnaire study found that, if the questionnaire was completed by the stroke patient rather than a caregiver, this was associated with better persistence with medications.16 In older adults with memory problems, it has been found that whether patients depend on themselves or a caregiver can have a significant impact on adherence. Not all caregivers take responsibility for a patient’s medication, and family members’ beliefs about a medication can affect adherence.17 Some caregivers are themselves disabled or suffer from cognitive impairments. Moreover, other variables such as frequency of visits, relationship to the patient (for example, unpaid or paid support), and carer agencies’ policies for managing medications can also affect patients’ adherence.
These findings were brought alive by three workshops we organised with a total of 26 survivors of stroke and 12 caregivers, in the context of gathering Patient and Public Involvement (PPI) input into research grant applications. Taking medicines emerged as an important issue: nearly half of patients reported that a family member or friend was supporting them with daily medicine routines, especially in relation to prompting tablet taking. Six out of 10 patients in one workshop admitted missing doses due to forgetting. Several patients were using dosette boxes. Taking medicines out of safety bottles and blister packs was generally considered difficult due to physical disabilities and required support.18 Only a small proportion of survivors were actually handling their own prescriptions, most relying on support from family members and/or community services.
THEORETICAL FRAMEWORK: INTENTIONAL NON-ADHERENCE AND NON-INTENTIONAL NON-ADHERENCE
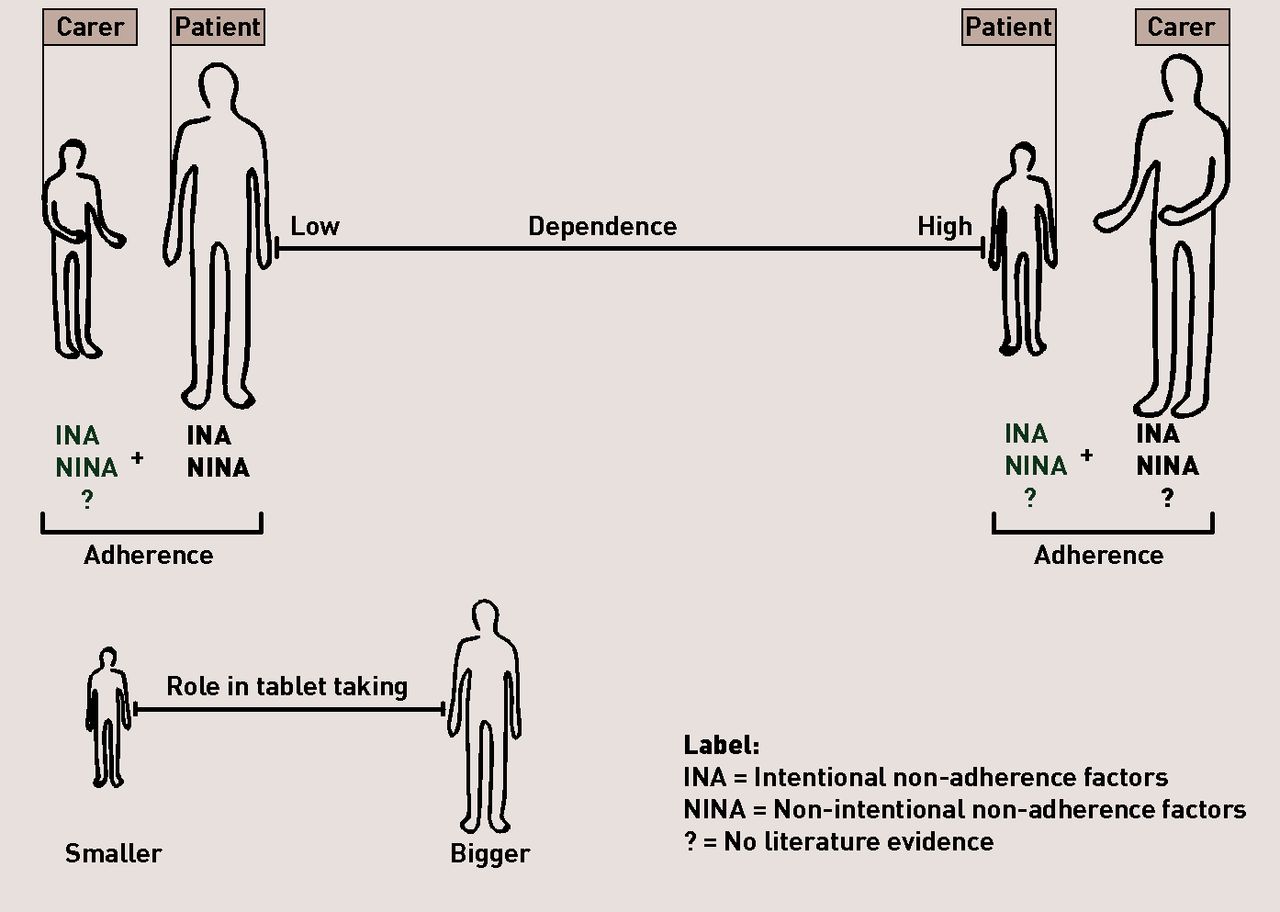
Two kinds of non-adherence to medication have been identified: intentional non-adherence (INA) and non-intentional non-adherence (NINA).19 INA refers to non-adherence that arises from the patient’s decision to take less medication than prescribed or to miss a dose or a day of medication; NINA refers to non-intentional barriers to adherence such as forgetting to take medication in spite of an intention to do so. In patients who have suffered stroke, NINA may also arise from neurological deficits such as hemiplegia, visual field defects, unilateral neglect, and dysphagia. In the case of a survivor of stroke who has a caregiver, it is also important to consider the caregiver’s INA and NINA. For example, the caregiver may withhold medication from the patient or give them a lower than recommended dose (INA), or forget to refill the prescription, or to give the patient their medication at the right time (NINA). Thus, the patient’s non-adherence to medication may be determined to a greater or lesser extent by their own INA and NINA or by their caregiver’s INA and NINA (Figure 1).
{kind=link}
Intentional and non-intentional non-adherence factors in stroke survivors and their caregivers. The larger the figure, the greater the role in determining patient overall adherence. Examples of INA factors: concerns about medications, lack of understanding of secondary prevention treatment. Examples of NINA factors: forgetfulness, physical and cognitive impairments.
As the patient’s dependency on others for medicine taking increases, the caregiver’s INA and NINA become more relevant in determining the patient’s adherence (right side, Figure 1). For example, consider a survivor of stroke with severe cognitive disabilities who is willing to take their medication and a caregiver who is reluctant to give the medication to the patient because they believe it would increase the risk of falls. In this case, the patient’s non-adherence might be due to the caregiver’s INA.
In other situations, the patient may show poor adherence because they forget to take their tablets or fail to swallow them due to dysphagia, even though the caregiver has supplied the medication.
Although INA/NINA provides a potentially useful framework for considering adherence in those who have suffered stroke, we currently know very little about the factors that influence adherence in survivors of stroke with severe disabilities and the role of their caregivers in patients’ adherence to medication. This is a knowledge gap that needs to be addressed (Box 1). The INA/NINA model of adherence should be extended to include the INA and NINA of caregivers. In this approach, each patient/carer dyad can be considered as a unit of adherence with each member of the dyad making a distinct contribution.
Key messages
There is lack of evidence on factors affecting adherence to medications in patients with more disabling strokes (at least a third of survivors of stroke).
Patients with disability may rely on caregivers for tablet-taking routines, though the exact proportion of dependent patients in this respect is unknown.
There is a need to investigate intentional and non-intentional adherence factors in caregivers of survivors of stroke with severe disability and how they interact with patient factors to determine adherence.
Novel interventions should be developed that address both caregivers’ and patients’ adherence factors.
MEASURING ADHERENCE IN PEOPLE WITH DISABILITY
Electronic monitoring devices are regarded as the ‘gold standard’ for assessing medication adherence in research. However, patients with significant disabilities might not be able to handle electronic bottles and instead rely on caregivers for the handing out of tablets. Family members or caregivers might not supervise tablet ingestion. The medicines carefully prepared by the caregiver might be forgotten, dropped accidentally and not be retrieved, or lodge in the patient’s mouth due to swallowing problems. Neither the patient nor the caregiver may be fully aware of the patient’s true level of non-adherence.
Therefore, clinical outcomes like blood pressure or cholesterol might be more appropriate ways to assess medication adherence in survivors of stroke with severe disability. However, these are indirect measures of medication adherence that may be influenced by other factors. There is therefore interest in novel approaches such as the Ingestible Sensor System, a device for measuring adherence by directly measuring ingestion of medications through a wearable sensor.20
We conclude that future studies are needed to characterise adherence to medications in patients dependent on others for medicine taking (Box 2). These could inform the development of novel interventions to improve adherence to medications in this group by addressing both patients’ and caregivers’ adherence factors. These studies could also inform the development of better measures of adherence in patients dependent on others for medicine taking.
Key research questions
Research is needed to address the following questions:
What proportion of survivors of stroke get support with daily medicine taking?
What proportion of survivors of stroke feel they need more support with daily medicine taking, and how is this associated with level of disability and number of daily medications?
What are the intentional and non-intentional adherence factors in caregivers of survivors of stroke with severe disability, and how do they interact with patient factors to determine adherence?
What are suitable measures of adherence in survivors of stroke with severe disability who are dependent on others for medicine taking?
Notes
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The author has declared no competing interests.
- © British Journal of General Practice 2015
REFERENCES
In this issue









Jump to section
- Top
- Article
- AN EXAMPLE ANALYSIS OF THE STROKE POPULATION
- FACTORS AFFECTING MEDICATION ADHERENCE IN STROKE
- LACK OF INVOLVEMENT OF PEOPLE WITH SIGNIFICANT DISABILITY AND CAREGIVERS IN ADHERENCE RESEARCH
- THE IMPORTANCE OF CAREGIVERS
- THEORETICAL FRAMEWORK: INTENTIONAL NON-ADHERENCE AND NON-INTENTIONAL NON-ADHERENCE
- MEASURING ADHERENCE IN PEOPLE WITH DISABILITY
- Notes
- REFERENCES
- Figures & Data
- Info
- eLetters

