


INTRODUCTION
In global health care,1 and within the UK NHS,2 providing accessible primary care remains a top-level priority for patients, politicians, healthcare planners, and health professionals. At its most basic, ‘access’ is simply the ability of an individual or population to obtain health care. Historical research3 has identified that strong primary care within national healthcare systems is associated with improved health outcomes, lower health system costs, and better patient experience of care compared with settings where primary care is more weakly represented. However, the simple provision of primary care is insufficient to ensure such beneficial outcomes — primary care services need to be made accessible to the population.
For example, Kringos and colleagues4 have recently shown that, across Europe, financial investment in health care at national level, and even financial investment in primary care, are in themselves not sufficient mechanisms to drive high-quality access to primary health care.
DEFINING ACCESS
Although a superficially obvious concept, several models of access to health care have been proposed.5–7 Access might usefully be seen as the smoothness of fit between demand for services and the organisation of those services.
In the UK, in 1995 a consultation rate of 3.9 per person per year was associated with an annual UK primary care consultation volume of 225 million consultations, by 2009 those figures had risen to 5.5 and 304 million respectively.8,9 This may in part be caused by supplier-induced demand related to more proactive health promotion and chronic disease management, and also by doctors themselves, with inequalities between patients and doctors in knowledge and power resulting in increasing patient demand for services.10 Changes in the provision of care will have an impact on demand and workload.
In the UK, the structure and organisation of primary care has changed substantially in recent years,11 but providing access to primary care has remained, at least notionally, a priority. However, providing high-quality access to primary care requires consideration of three additional important factors. First, services accessed should be effective in supporting and achieving the central goal of any healthcare system — health. Second, access should be based on a principle of equity in which healthcare provision is based on need for health care, and is not subject to ability to pay, or to sociodemographic factors that may be outwith the control and influence of the potential service user. Finally, the user’s experience of the service matters, and culturally sensitive health care needs to take account of the user’s ideas, concerns, and expectations12 regarding health and health care.
MODELS OF ACCESS
In 1981, Penchansky and Thomas6 identified the importance of access as a key concept in health policy and health policy research, proposing a model with five key dimensions of access (Box 1). More recently, Fortney and colleagues13 have identified the need to recognise a ‘digital dimension’ to access, incorporating the potential for synchronous and asynchronous virtual interactions with the evolving healthcare system.
Domains of access, after Penchansky and Thomas6
Availability — the fit between volume/type of services and the volume/type of patient needs.
Accessibility — geographical issues including travel time and cost associated with using health care.
Accommodation — resource organisation and client-perceived appropriateness.
Affordability — costs of services including client-perceived worth.
Acceptability — attitudinal ‘fit’ between client and the characteristics of providers and services.
MEASURING ACCESS
Given the potential complexity of the concept of access, many metrics might be applied in assessing whether any given model of care is providing accessible care. Historically, rates of service utilisation have been seen as measures of ‘revealed accessibility’7,14 — more service use being equated with improved access. However, such measures lack sophistication, it being unclear whether they reflect demand or organisation of services, and failing to account for the three domains identified above as markers of quality of access to health care. For example, service use in two neighbouring general practices might be the same if they both provide the same number of appointments, but there could be much more unmet need and a longer wait for an appointment in one practice than another. New metrics of access have been developed to complement those relating to demand and supply.
The English GP Patient Survey15 represents a good example of one such metric. Introduced in 2006 and extended in 2008, the survey includes 42 questions documenting primary care provision and characterising respondents. Apart from its role in providing an overview of patients’ experience of care in each of England’s 8000 practices, survey data also inform both Domain 5 of the NHS Outcomes Framework, focusing on improvements in people’s experience of care, and the Care Quality Commission’s framework for practice review (Box 2).16
The GP Patient Survey and access to care: some findings
The GP Patient Survey can be used to provide robust comparisons between healthcare providers such as practices.29,30
Improving the experience of patients in low-scoring practices will improve the quality of care provided to white patients, and reduce ethnic group differences in patient experience.31
Adjusting for case-mix generally has only a small effect on practice scores of patient experience of care.32
Interpersonal care provided by the doctor, not the availability of appointments, is the most important factor in determining overall satisfaction with primary care services.33
Of the domains included in the survey, the ability to see a doctor of the patient’s choice represents the biggest gap between what patients want and what is currently provided.34
There were good correlations between the availability of appointments and the GP Patient Survey access scores in a ‘mystery shopper’ study.35
The convenience of practice opening hours was the strongest single predictor of use of out-of-hours care.36
Commercial providers of out-of-hours GP care have somewhat lower scores on patient feedback than not-for-profit or NHS provider organisations.37
MANAGING ACCESS
In the UK, the Quality and Outcomes Framework has been used to provide financial incentives to practices, with the GP Patient Survey data being used as the basis of a practice-based pay-for-performance scheme between 2009 and 2011. In broad terms, there are three ways of improving access to primary care: increasing the capacity of the system, reducing the demands for care, or improving the efficiency and responsiveness of the system through new ways of working. In each case, there can be factors that enable or block these changes.
Increasing capacity
Perhaps the most obvious way to improve access to primary care is to provide more appointments, either through employing more doctors or through making better use of the skills of other professionals. In the face of an imminent workforce crisis,17,18 much attention has been given to increasing recruitment to careers in general practice, but what really matters is the number of full-time equivalents, not just the total number of GPs, and the productivity of these doctors in terms of number of patients seen per annum. A number of factors are likely to lead to decreased productivity for good reasons (for example, the need for longer appointments in the face of multimorbidity, and increased expectations for case management), and need to be understood and accounted for.
An alternative is to increase capacity through engaging the under-utilised skills of nurses and pharmacists. A recent scheme allowing patients who do not pay for prescriptions to obtain a range of treatments from pharmacists free of charge, without needing to visit a doctor, is a good example of how changes in policy can enable improvements in access.19 However, research suggests that attempts to improve access through providing alternatives to GPs do not necessarily have the desired effect. Substituting nurse practitioners for GPs does not appear to be more efficient than employing more doctors20 (and suitably trained nurses are in short supply, just like GPs). Similarly, creating NHS walk-in centres appeared to increase demand rather than reduce general practice workload, and were more expensive21 than the general practice care for which they were designed to substitute for.21
Decreasing demand
Demand for health care is not fixed: it is related to prior experience of care, patients’ expectations, the alternative routes to help that are available, and patients’ perceptions of their relative advantages and costs. Many of these factors can be influenced by policy, for example, by public education initiatives on appropriate use of services (for example, emergency departments), and alternative sources of healthcare advice (pharmacies), or by seeking to change expectations for particular treatments (for example, antibiotics).
In many countries, co-payments are used and different levels of payment for different services can modify how people use services,22 and, in the NHS, the length of time people have to wait to see different healthcare providers can have a similar effect.
Anticipatory care (for example, flu immunisation for vulnerable populations) can have a powerful effect on reducing the total number of people needing health care. However, paradoxically, that ambition is often only achieved through the introduction of complex protocols and schedules resulting in the need for additional workload in primary care.
Changing patient expectations, for example, in relation to antibiotic prescribing in upper respiratory infections, is potentially worthwhile,23 but may be challenging to implement and may achieve only modest change in practice.24
Moving from a culture of medical dependency — ‘a pill for every ill’ — to improved self-care utilising a range of formal and informal community-based resources is likely to be of importance in moderating demand for health care.
New ways of working
Although policy can influence public perceptions, the main factor driving the increased demand for health care is the ageing population. It seems unlikely that there will be a substantial increase in the supply of primary care in the near future. Therefore there will be a continued need to find ways to manage access to care through new ways of working. Several approaches have been tried, and some of them have been evaluated in research studies:
Triage
This is based on the assumption that through an initial assessment it is possible to stream individuals into the form of care that is likely to meet their needs as quickly and efficiently as possible, thus maximising the use of limited resources. This initial assessment might be made by telephone or by another professional who is less expensive or less scarce than a doctor, but overall effects are not always predictable, (such as implications across staff team in practice) and may not be considered desirable (such as potential increases in overall workload) (Box 3).
The ESTEEM trial:26 the effectiveness and costs associated with telephone triage in primary care
Large-scale cluster randomised trial of 21 000 patients requesting a same-day consultation with a GP.
Telephone triage, whether delivered by a doctor or by a nurse, was associated with an increase in the overall number of primary care contacts for patients in the 28 days following their original consultation request when compared with usual care.
Triage, especially where delivered by a nurse, was less acceptable to patients than usual care.
Costs to the health service per patient over 28-day follow-up were almost identical across the three trial arms.
Introducing telephone triage was associated with a shift in workload from face-to-face consultations to telephone consultations, and from doctors to nurses.
Some practices might consider triage to offer an effective means of managing workload, although such systems should be introduced with a degree of caution, and with an awareness of unintended system-wide effects that might arise in the process.
Advanced Access
This involved a variety of strategies to support same-day appointments including telephone triage, booked telephone consultations, advice about self-care for minor illnesses, and delegation of clinical work to nurses and healthcare assistants. Dramatic claims were made about improvements in access, but subsequent, more rigorous evaluations showed that results were much less dramatic and conclusions more nuanced (Box 4). The introduction of ideas from Advanced Access were over-shadowed by the introduction of a 48-hour access target, providing an example of how some potentially good ideas can be derailed by the blunt effect of simplistic targets.
Advanced Access: findings from evaluation38,39
Mixed-methods evaluation comparing 24 general practices that introduced Advanced Access and 24 that did not (control practices).
Practices that introduced Advanced Access used a variety of strategies, some of which were also used in control practices.
Practices of both types tailored their systems to suit their population — different patient groups had different priorities.
Most general practice consultations are about long-standing health problems, so speed of access is less important to most patients than being able to choose a convenient appointment time and/or a particular GP or nurse.
Advanced Access had only a minor impact on access, patient satisfaction, or staff satisfaction.
Several initiatives involve a more fundamental redesign of practice appointment systems. Rather than booking an appointment in advance, almost all patients have their initial consultation by phone, and the GP tries to manage their problem at the time or by arranging for them to see the appropriate person (often the same day). Advocates of this approach claim that it improves access and patient satisfaction, increases continuity of care, reduces patient use of emergency departments, and reduces GP workload and stress. However, the evidence is so far based on uncontrolled observational studies conducted by those who are promoting the schemes, and more robust independent research is needed and is underway.25–27
Alternatives to face-to-face consultations
Many policymakers and patients are enthusiastic about the potential of technology, such as e-mail or Skype, to improve access to health care, but GPs’ reactions have been varied and generally cautious, and implementation so far seems to be very limited. The concerns largely relate to the threat of supplier-induced demand. Clarity is needed about how alternatives to face-to-face consultations may lead to benefits or disadvantages for different groups of the population, and research is underway on this topic.28
CONCLUSION
Access is most appropriately considered as a system-level metric of healthcare provision that takes account of demand and organisational factors as well as other factors, all of which might impact on the outcomes of that healthcare provision in individual patients and in patient populations. There is a need for more sophisticated models than are currently widely used when considering access. Such new models (such as our schema in Figure 1) should capture within them considerations of equity, experience, and effectiveness alongside simple demand and organisational considerations. The accessibility of health care is never absolute, but reflects the balance and tension existing within a complex and dynamic social system.
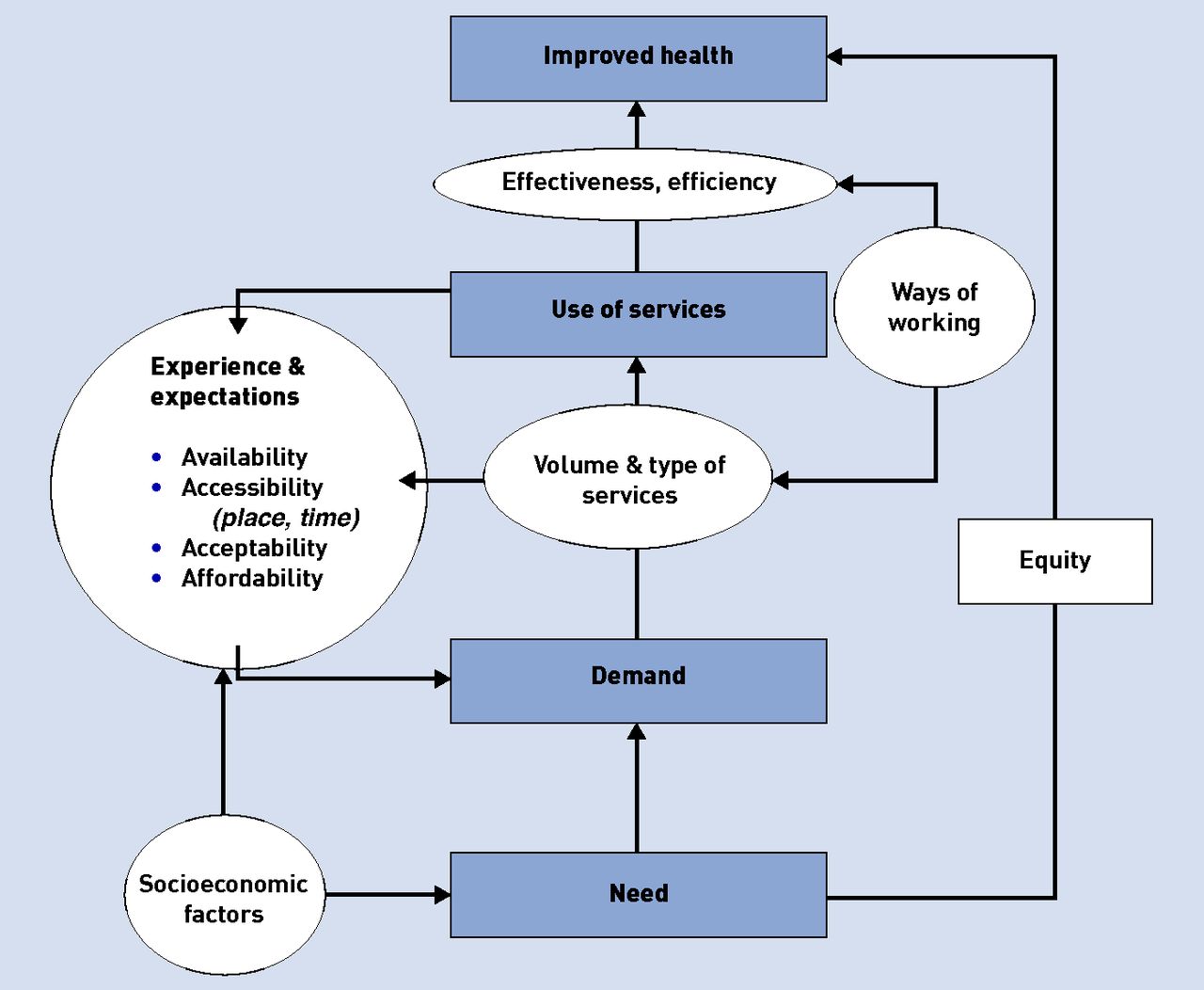
{kind=link}
Access to primary care: an overview.
Notes
Provenance
Freely submitted; externally peer reviewed.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received June 3, 2015.
- Accepted August 12, 2015.
- © British Journal of General Practice 2015
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

