


Abstract
Background Self-management support is an important component of the clinical management of many chronic conditions. The validated Self-Management Screening questionnaire (SeMaS) assesses individual characteristics that influence a patient’s ability to self-manage.
Aim To assess the effect of providing personalised self-management support in clinical practice on patients’ activation and health-related behaviours.
Design and setting A cluster randomised controlled trial was conducted in 15 primary care group practices in the south of the Netherlands.
Method After attending a dedicated self-management support training session, practice nurses in the intervention arm discussed the results of SeMaS with the patient at baseline, and tailored the self-management support. Participants completed a 13-item Patient Activation Measure (PAM-13) and validated lifestyle questionnaires at baseline and after 6 months. Data, including individual care plans, referrals to self-management interventions, self-monitoring, and healthcare use, were extracted from patients’ medical records. Multilevel multiple regression was used to assess the effect on outcomes.
Results The PAM-13 score did not differ significantly between the control (n = 348) and intervention (n = 296) arms at 6 months. In the intervention arm, 29.4% of the patients performed self-monitoring, versus 15.2% in the control arm (effect size r = 0.9, P = 0.01). In the per protocol analysis (control n = 348; intervention n = 136), the effect of the intervention was significant on the number of individual care plans (effect size r = 1.3, P = 0.04) and on self-monitoring (effect size r = 1.0, P = 0.01).
Conclusion This study showed that discussing SeMaS and offering tailored support did not affect patient activation or lifestyle, but did stimulate patients to self-monitor and use individual care plans.
INTRODUCTION
Enhancing self-management of health and disease is widely seen as a way to improve health outcomes, increase self-control, and decrease healthcare costs. It involves patients being encouraged to take responsibility for their health and play an active role in managing the disease.1 The UK’s Department of Health defined self-management as:
‘… the care taken by individuals towards their own health and wellbeing: it comprises the actions they take to lead a healthy lifestyle; to meet their social, emotional and psychological needs; to care for their long-term condition; and to prevent further illness or accidents.’2
Implementing effective self-management support in routine health care has proven to be a challenge.3 Research shows that the effectiveness of self-management interventions depends on individual characteristics, such as self-efficacy and social support.4–8 However, rigorously evaluated interventions to personalise self-management support to these characteristics appear to be lacking.
The Self-Management Screening questionnaire (SeMaS) assesses individual capabilities or barriers for self-management; it has been validated for patients with chronic diseases, such as diabetes mellitus, (risk of) cardiovascular diseases, asthma, or chronic obstructive pulmonary disease (COPD).9 SeMaS assesses:
perceived burden of disease
self-efficacy;
locus of control;
social support;
coping;
anxiety; and
depression.
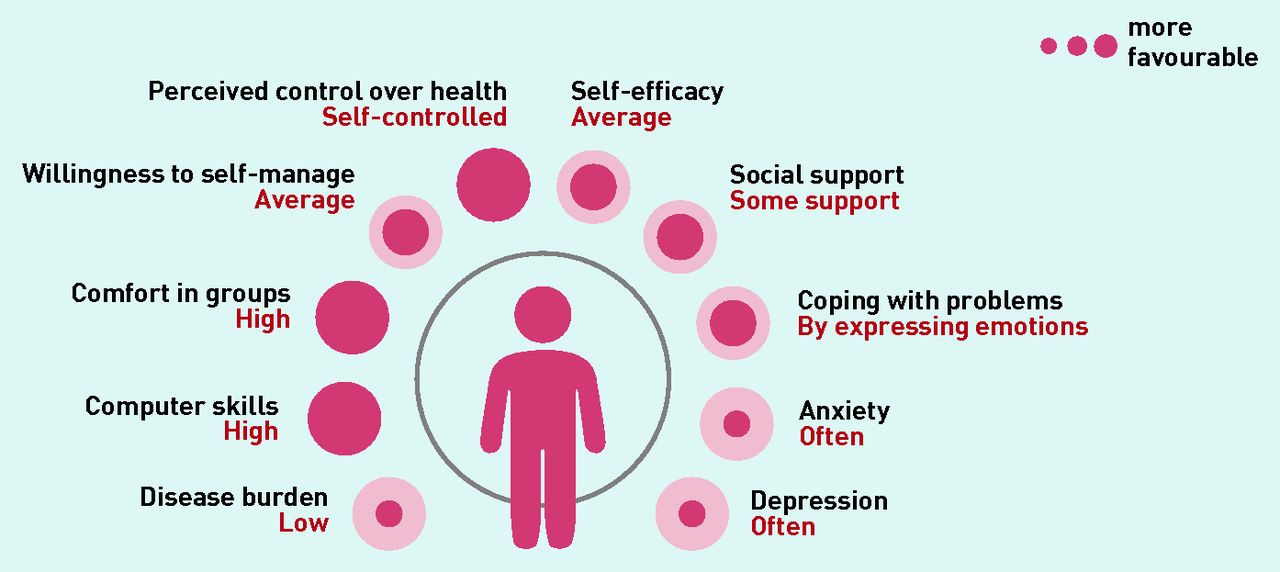
To guide the type of support, it also contains items about computer skills, functioning in groups, and willingness to perform self-care. A 1-page graphic profile of the results is provided to support the patient and health professional in counselling on self-management and to make the results of SeMaS easy to use in daily practice (Figure 1).9

Example of a SeMaS profile.
Increasing patient activation (comprising knowledge about the chronic condition, the skills to cope with the condition, and the self-efficacy of the patient) is considered a positive outcome of self-management interventions.10 Both individual care plans and self-monitoring have shown to positively affect self-management and other (clinical) outcomes, such as medication adherence, for various conditions.11–13 A recent Cochrane Review showed that personalised care planning improves several indicators for people with long-term conditions, such as glycated haemoglobin, systolic blood pressure, self-efficacy, and the ability to carry out self-care activities.14 Furthermore, in many cases, stimulating self-management aims to change the patient’s lifestyle for the better.
How this fits in
The effect of self-management support depends on individual characteristics but many self-management interventions follow a ‘one-size-fits-all’ principle. By discussing results of the validated Self-Management Screening questionnaire (SeMaS) with the patient, healthcare providers can provide personalised support. This study showed that, although applying SeMaS did not have a positive effect on patient activation or patients’ lifestyle, it did result in more patients self-monitoring and using their individual care plans. This is the first study applying a barrier analysis in order to provide personalised self-management support with promising results.
In the study presented here, the effect of providing personalised self-management support using SeMaS was assessed with regard to patient activation, health-related behaviours, and individual care plans in primary care patients with a chronic disease.
METHOD
A two-arm cluster randomised controlled trial (RCT) was conducted, as described in the study protocol and registered in the Netherlands National Trial Register (reference number: NTR3960).15 More details on the method are available from the authors. Parallel to the RCT a process evaluation was performed including interviews with practices nurses, which are reported on separately.
Setting
The study was performed in 15 group practices of the primary care cooperative De Ondernemende Huisarts (DOH) in the south of the Netherlands. DOH provides programmatic multidisciplinary care to 110 000 patients with chronic diseases. One author randomised the practices as clusters to the control (n = 8) or intervention (n = 7) arm using a two-block randomisation list.15
Patients
Adults with at least one chronic condition (diabetes mellitus, [risk of] cardiovascular diseases, asthma, or COPD) and a planned consultation with the practice nurse in the inclusion period (January 2013 to July 2013) were eligible to participate in the study. Patients were sampled from the practice nurses’ agenda using a systematic method to avoid selection bias. One practice did not plan ahead so patients were systematically sampled from a list of dates when they received the call to visit the laboratory for annual or quarterly blood tests (for example blood glucose); these patients subsequently had to make an appointment with the practice nurse.
Following power calculations, 50 patients per group practice were recruited at baseline.15 Anticipating a 30% response rate and a 33% attrition rate, 150 patients per practice were invited to participate. Based on the number of included patients after 3 months, 100 additional patients were invited from one control (n = 50) and one intervention practice (n = 50).
Intervention
The intervention consisted of the practice nurse acknowledging the patient’s SeMaS results in the planned consultation with the patient, and providing subsequent personalised self-management support based on their SeMaS profile, using the support options of the care group as appropriate (the care group offered several internet-based support programmes, educational group meetings, and physical activity groups). The intervention was hypothesised to affect patient activation and health-related behaviour, as shown in the logic model (available from the authors on request) and the study protocol.15 Two authors together provided one 2-hour group training session to the practice nurses and GPs on:
information about the constructs in SeMaS;
how to interpret and discuss results with the patient; and
role play.
GPs were involved in the training to make sure that they were informed about the project and to ensure their involvement and commitment.
A paper-based manual contained instructions for health professionals on personalised self-management support and how to cope with possible barriers.9,15 Of the two authors who conducted the training, one is a researcher with expertise on SeMaS and the other trainer is a psychologist with expertise on training in behavioural change methods.16 To provide additional support, the author with expertise in SeMaS visited intervention practices shortly after starting the study to ensure that practice nurses understood the information and were able to work with SeMaS in their consultations. This author was available to answer nurses’ questions during the study.
The research team visualised the results from each SeMaS baseline questionnaire as an automatically generated profile (two versions) (Figure 1), and mailed these to the practice nurse. The professional version contained the profile and tailored instructions; the patient version contained a neutral explanation of the profile with tailored instructions how to address barriers found. The practice nurses were instructed to:
discuss the profiles with the patient; and
use the manual where necessary to address the profile in a personalised self-management support dialogue.
In order to check intervention fidelity, 1 week after the planned consultation, patients were asked whether SeMaS was discussed with them during the consultation. The per protocol analysis is based on data from patients reporting that SeMaS was discussed.
Outcomes
Questionnaires
Patients were invited to participate in the study by mail, approximately 4 weeks before their planned consultation; along with the invitation, they were sent an informed consent form and the baseline questionnaire. Participants received the final questionnaire 6 months after the consultation.
The baseline and final questionnaires comprised the following:
SeMaS questionnaire;
13-item Patient Activation Measure (PAM-13);
Short Test of Functional Health Literacy in Adults;
Rapid Assessment of Physical Activity;
Rapid Eating Assessment for Participants — short; and
PAM-13 was the primary outcome measure; it measures patient activation, with subdomains covering knowledge, skills, and self-efficacy.10 SeMaS consists of 27 items and covers the domains outlined in the introduction.9 An overview of the questionnaires is available from the authors on request.
Medical record data
Data were extracted from patients’ electronic medical records by the care group’s data management team, using standard extraction procedures. The coded dataset was provided to the research team. The conditions were assessed according to:
their International Classification of Primary Care codes;
the number of documented individual care plans;
the number of patients performing clinical self-monitoring (weight, blood pressure, and glucose levels);
the number of referrals to self-management interventions (group courses, internet coaches, and informative websites, either registered in the consultation report or as a referral); and
the number of consultations in general practice during the study period.
A keyword search was used to code the consultation notes for referrals to self-management interventions.
Data analysis
Analyses, performed with SPSS software (version 20), are described in detail in the study protocol.15 A multivariate, multilevel linear regression model was used to assess the difference in PAM-13 scores, exercise, nutrition, and the number of consultations and referrals between the intervention and control arms at 6 months, when controlled for baseline scores. The covariates were controlled for:
age;
sex;
chronic condition;
social support;
diagnosis of depression; and
health literacy.
Generalised linear models were used for the dichotomous outcomes of smoking, individual care plans, and self-monitoring.
Per protocol analyses were also performed; the data from all participants in the control group, plus those in the intervention group who reported that SeMaS was discussed during their planned consultation, were used. For the pre-specified subgroup analysis, the score on each SeMaS dimension was divided into three levels:
less favourable for self-management;
moderately favourable for self-management; or
highly favourable for self-management.
A description of the analysis, together with the results of it, are available from the authors.
The multiple imputation procedure was used to check whether missing values influenced the results of the primary analysis.22 Five datasets were generated using predictive mean matching methods under the missing at-random assumptions.
RESULTS
Baseline characteristics
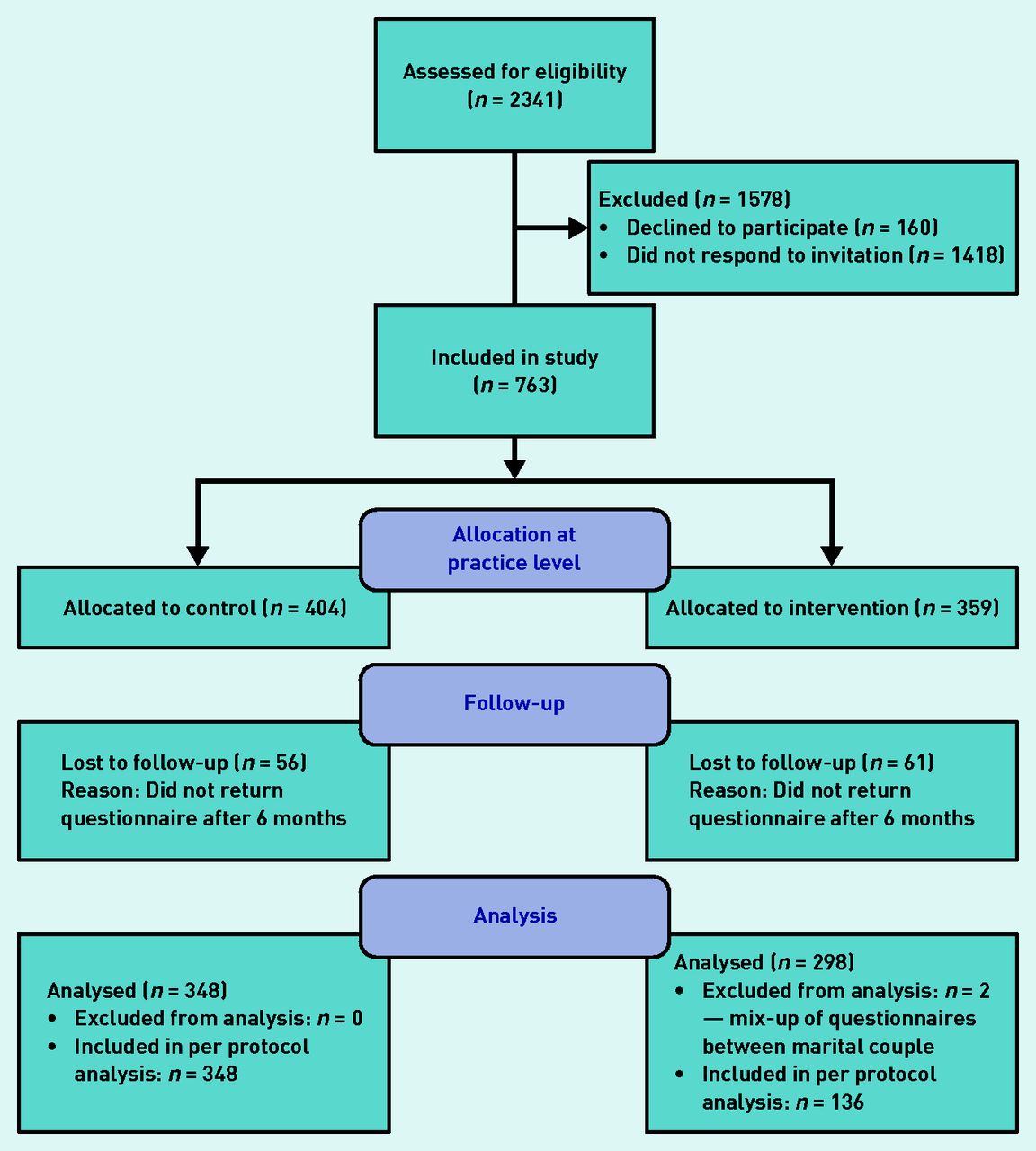
In total, 763 patients were included in the study, of which 117 were lost to followup (Figure 2). Table 1 shows the patients’ characteristics. PAM-13 scores were calculated on a scale of 0–100; the average baseline score for the control group was 59.1 (standard deviation [SD] 14.5) versus 59.5 (SD 16.1) for the intervention arm.
{kind=link}
{kind=link}
Trial flowchart.
Participants’ baseline characteristics
Table 2 shows the characteristics of the total and SeMaS subgroups by primary outcome (PAM-13 score at follow-up: 59.7 [SD 15.4] for the control group and 60.7 [SD 15.5] for the intervention arm) and by secondary outcomes (nutrition, exercise, smoking, individual care plans, clinical self-monitoring, number of consultations, and referrals to interventions).
Total and SeMaS subgroup characteristics, by primary and secondary outcomes
Primary outcomes
The results of the primary analysis are shown in Table 3. The PAM-13 score at follow-up did not differ significantly between the control (n = 348) and intervention (n = 296) arms (effect size r = 0.6, 95% confidence interval = −1.9 to 3.1; P = 0.59). Intra-class correlation was 0.001. The covariates of health literacy (effect size r = −0.9, P<0.001) and education (effect size r = 0.8, P = 0.006) showed a significant association with the PAM-13 score data not shown. Pooled analysis of the multiple imputed dataset showed similar results (data not shown).
Results of the regression models for the primary and secondary outcomes
Secondary outcomes
The intervention was found to have no effect on exercise, nutrition, or smoking (Table 3). Being female (P = 0.001) and having higher education (P = 0.012) were associated with healthier nutrition habits (data on covariates not shown). Other covariates did not show associations with exercise or nutrition.
The percentage of participants performing clinical self-monitoring was significantly higher in the intervention group than in the control group: 29.4% versus 15.2% respectively (effect size r = 0.9, P = 0.011) (Table 2). No effect was found relating to the number of documented individual care plans or self-management interventions offered.
Per protocol analysis
Of the intervention group (n = 296), 136 patients reported that SeMaS was discussed and 96 stated it was not; data were missing for 64 members of this group. The per protocol analysis showed no effect on the PAM-13 score (effect size r = 0.7, P = 0.61), as shown in Table 4, but the effect of the intervention was significant on the number of individual care plans (effect size r = 1.3, P = 0.04) and on clinical self-monitoring (effect size r = 1.0, P = 0.01).
Results of the per protocol analysis, by primary and secondary outcomes
DISCUSSION
Summary
In this cluster RCT, a tool for personalising self-management support in patients with chronic disease was tested. Of the secondary outcomes, the intervention showed a positive effect on the percentage of patients performing self-monitoring (primary analysis and per protocol analysis) and on the number of individual care plans (per protocol analysis). The intervention showed no effect on the primary outcome of patient activation.
Strengths and limitations
A strength of this cluster RCT is its closeness to daily practice, as the intervention was integrated into normal processes as much as possible. This enhances its relevance to decision makers as application in daily practice proved feasible. However, a number of limitations may be noted.
The response rate on the invitation for the study was 30%. It was not possible to perform a non-responder analysis, as no data were available.
In addition, having been discussed with the patients during their consultation, SeMaS was expected to have an effect on the support offered by the practice nurse, who could personalise it according to the patient’s SeMaS results. This support could contain the self-management interventions offered by the care group, as well as the support the practice nurse can offer; that is, education/psychoeducation on how to cope with barriers, providing information about the condition, lifestyle, self-monitoring, and composing an individual care plan. The self-management interventions were expected to contribute to the effect of SeMaS. However, they were only used in a small subset of patients, and some of the support interventions were unavailable. This hindered practice nurses’ support options and may have reduced the positive outcomes.
Finally, approximately one-third of patients in the intervention group reported that SeMaS was not discussed in their consultation. In evaluative interviews practice nurses gave several reasons why SeMaS had not been discussed: they sometimes received the SeMaS profile after the consultation had taken place, forgot to discuss the profile, or used the results implicitly in their consultation (N Eikelenboom et al, unpublished data, 2016). Also, if no barriers were present, the practice nurse may not have spent much time on discussing SeMaS, but used the time to discuss other subjects. Practice nurses experienced time pressure; discussing SeMaS took extra time and they expressed that there was a lot to discuss, including test results. Patients may not have recalled this when filling in this question. In addition, data regarding the discussion on SeMaS in the consultation with the practice nurse were missing on this item for 21.6% of patients in the intervention group.
Comparison with existing literature
The broad definition of self-management implies that such activities and support may vary to a large extent.2 In addition, not all aspects are easily supported by practice nurses; psychological needs, for example, will likely lie outside of their expertise. It is possible that the variety of aspects of self-management and the limited support practice nurses can offer contributed to the results of this study that were not statistically significant. The practice nurses in this study were instructed to help patients overcome barriers, mainly regarding locus of control and coping; these factors are important, but not easily changed in a 6-month period. In addition, the nurses’ training may have been insufficient to address the barriers; this may have hindered positive findings. Training comprised a 2-hour group session and a follow-up visit. More intensive and in-depth training, with for instance coaching on the job or feedback moments after patients’ visits, could strengthen practice nurses’ abilities to overcome barriers effectively.
As described in a recent Cochrane Review, the effects of personalised care planning were positive on several outcomes, although these effects were not large.14 The effects tended to be larger when the programme was more intense, or the patient had more contact with their practice nurse. As SeMaS was used in routine care in the study presented here, but did not form an intensive programme, its intensity may have been too low. On the other hand, however, the per protocol analysis in this study showed a statistically significant difference between the intervention and control arms with regard to the number of individual care plans, despite the fact that individual care plans are still in the implementation phase in this care group.
Self-monitoring is traditionally considered to be an aspect of self-management, whereas patient activation and healthy lifestyles have only been linked to self-management more recently. By self-monitoring, patients can keep check on their chronic condition and experience the effect of their behaviour on clinical outcomes.13,23,24 Self-monitoring can also increase self-efficacy for health-related behaviour.25 This trial, which had a heterogeneous study population, showed a significant effect on self-monitoring. Apparently, this aspect of self-management support is common and easily implemented in daily practice, and there is potential for improvement in primary care. Given the positive findings in this study, the concept and potential of personalised self-management support seems promising.
Implications for research and practice
Based on this study’s positive findings, SeMaS may be a useful tool to progress the personalisation of care and support in daily practice. The following could enhance the positive effects of this intervention:
targeted use of SeMaS for patients whose self-management may be hindered by one or more barriers;
more intensive and more in-depth training for healthcare providers, resulting in improved skills to successfully tackle those barriers and provide personalised support by creating differentiated individual care plans, stimulating self-monitoring, and using available interventions when appropriate.
Further research is recommended before these are implemented in daily practice.
Acknowledgments
The authors thank the DOH care group, the care providers, and all patients for their participation in this study; the trial steering group for its contributions; ROS Robuust and Philips Research for their financial contributions; all colleagues of IQ Healthcare, and in particular Janine Liefers, Juliette Cruijsberg, Jolanda van Haren, and Irah Noy, who provided help and support in organising this trial.
Notes
Funding
This study was funded by ROS Robuust (grant no. E12EL06) and Philips Research (funding no. NLYO-4520132964). ROS Robuust was not involved in the design of the study, nor in the collection, analysis, or interpretation of the data. Philips Research was represented in the trial steering group by authors Joyca Lacroix and Aart van Halteren but not involved in the collection or analysis of the data; results were discussed with the steering group for interpretation.
Ethical approval
Ethical approval was waived by the Medical Research Ethics Committee, the CMO region Arnhem-Nijmegen (registration number: 2012/561).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The Department of IQ Healthcare (DOH) received grants from ROS Robuust and from Philips Research, during the conduct of the study, as well as grants from Philips Research outside of the submitted work (Nathalie Eikelenboom, Jan van Lieshout, Annelies Jacobs, Michel Wensing). The DOH care group received grants from Philips Research while the study was being undertaken, and outside of the submitted work (Nathalie Eikelenboom, Ivo Smeele, Maarten Klomp). Frank Verhulst received personal fees from DOH while the study was being undertaken and outside of the submitted work for his involvement in the training of the health professionals. In addition, Frank Verhulst has registered Doen en blijven doen at the Benelux-bureau for intellectual property (no: 1222793).
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received March 19, 2015.
- Revision requested May 8, 2015.
- Accepted October 25, 2015.
- © British Journal of General Practice 2016
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

