


Abstract
Background Out-of-hours (OOH) primary care services are integral to the care of patients at end of life. Little is known about the OOH service usage of patients with palliative care needs.
Aim To describe patterns of usage of patients presenting to an OOH service and coded as ‘palliative’.
Design and setting A descriptive study of data from the Oxfordshire OOH service.
Method A database of all patient contacts with the Oxfordshire OOH service from a 4-year period (June 2010–August 2014) was used to extract demographic and service usage data for all contacts to which clinicians had applied a ‘palliative’ code. Observed differences in demographic features between palliative and non-palliative contacts were tested using logistic regression.
Results Out of a total of 496 931 contacts, there were 6045 contacts coded palliative; those ‘palliative’ contacts provided care to 3760 patients. Patients contacting the OOH service with palliative care needs did so predominantly during weekend daytime periods, and over a third had more than one contact. Patients were predictably older than the average population, but contacts coded as ‘palliative’ were relatively less deprived than contacts to the OOH service for all causes, even after adjusting for age and sex.
Conclusion The current ‘one-size-fits-most’ model of OOH primary care may not allow for the specific needs of patients at the end of life. Wider analysis of palliative patient flow through urgent care services is needed to identify whether healthcare access at the end of life is inequitable, as well as the capacity requirements of a community-based service that can provide high-quality end-of-life care.
INTRODUCTION
In recent years, the recognition that good-quality end-of-life care is a fundamental component of a modern health service has led to greater interest in and provision of palliative care services.1 A focus on patient priorities has demonstrated that, although most people with terminal illness want to die at home, only a minority achieve this.2 For patients to die at home, primary care services need to provide or to coordinate the provision of end-of-life care.
In the UK, out-of-hours (OOH) GP services are an integral part of primary care provision (Appendix 1 contains a structure and case study example). In 2013–2014, OOH primary care in England handled around 5.8 million cases, 3.3 million of which were face-to-face consultations, including 800 000 home visits.3 These OOH GP services provide care outside of ‘core’ contracted hours — usually from 18:30 to 08:00, and on weekends and bank holidays. The Oxfordshire OOH service provides care to a population of over 600 000 people, with around 120 000 patient contacts per year.
Although the number of patient contacts with OOH primary care is small in comparison with in-hours primary care (in which an estimated 340 million consultations occur each year),4 OOH services provide clinical cover for over two-thirds of the hours in a calendar year. OOH primary care services are necessarily integral to the care of patients at end of life. This presents a challenge, however, and in January 2015 identifying ‘the best ways of providing palliative care outside of working hours to avoid crises and help patients to stay in their place of choice’ was identified by the Palliative and end of life care Priority Setting Partnership as the number one priority for palliative care research.5
To date, little is known about the OOH service usage of patients with palliative care needs, despite this information being a key first step in designing services better suited to their needs. This descriptive study analyses a large population-based dataset of patient contacts with an OOH service provider to better describe patterns of usage of patients presenting to the OOH service and labelled by the service as ‘palliative’.
METHOD
In a service evaluation agreed with Oxford Health NHS Foundation Trust, a database of all patients presenting to the Oxfordshire OOH service over the 4 years from June 2010 to August 2014 was created from the electronic medical record used by OOH clinicians (SystemOne). This database did not include contacts with district nurses in the OOH period, as these were handled by a separate service. All patient identifiers were removed on entry to the database. Patients without an NHS number were not included, as repeat visits to the service could not be assessed. Demographic data consisted of age, sex, and Index of Multiple Deprivation (IMD) score.6 Service data included call volume and time period.
How this fits in
Identifying the best ways to provide palliative care outside of working hours has been highlighted by patients as a top priority for end-of-life care. Understanding the current service usage of patients at end of life is a key first step in designing services better suited to their needs. This study analyses 4 years of data from a large out-of-hours primary care service to describe service usage and demographics of patients using the service at end of life: who uses the service, when do they use it, and what happens next?
The time interval between assessments in the OOH period was calculated using calendar days that began at midnight, and timings of calls were classified as follows: ‘evening’, 19:00–00:00, ‘overnight’, 00:01– 08:00, ‘day-time weekend’, 08:01–18:59 (Saturday and Sunday).
Validation of clinical coding
At the end of each OOH consultation, clinicians assign at least one clinical code to the case (for example, ‘cardiac’). For this study, patients at end of life were identified by searching the above database with the clinical code ‘palliative’ (the only end-of-life code available on ‘System One’). As more than one clinical code could be assigned to each case, where ‘palliative’ was assigned as a secondary or tertiary code, the primary clinical code was also noted.
To validate the clinical codes applied by the OOH clinicians it was estimated, based on previous coding validity studies7 that analysis of 230 records would be required to establish the coding validity with a confidence level of 90% and 5% margin of error. A random selection of 230 records was obtained using SPSS, and the clinical code was compared by one author to the conclusion drawn by the clinician in the medical notes. The positive predictive value (PPV) of the clinical code for medical diagnosis or conclusion including those cases classed as miscellaneous was 90%. If only those codes that positively described an established clinical presentation were assessed (for example, ‘cardiac’ but not ‘miscellaneous’ or ‘referred to acute trust’), the PPV was 97.5%.
Analysis
Demographic data including age and sex were obtained for patients coded as ‘palliative’, and were compared with all patients presenting to the OOH service. Deciles of IMD scores were generated from all patients contacting the Oxfordshire OOH service over the 4-year period, and the percentage of palliative care patient contacts in each of these deciles was compared. Where a difference in demographic features was noted in the ‘palliative’ group compared with the whole population presenting to OOH, it was tested using logistic regression including the other available demographic features to explore whether variation in other demographic features could explain the observed difference. Analyses were undertaken in SPSS version 22.
RESULTS
Between June 2010 and August 2014, (excluding 14 572 contacts without an NHS number), there were 496 931 contacts with the OOH service. Of these, 6045 contacts were coded as ‘palliative’ (1.2% of all contacts) to provide care for 3760 patients.
Demographics
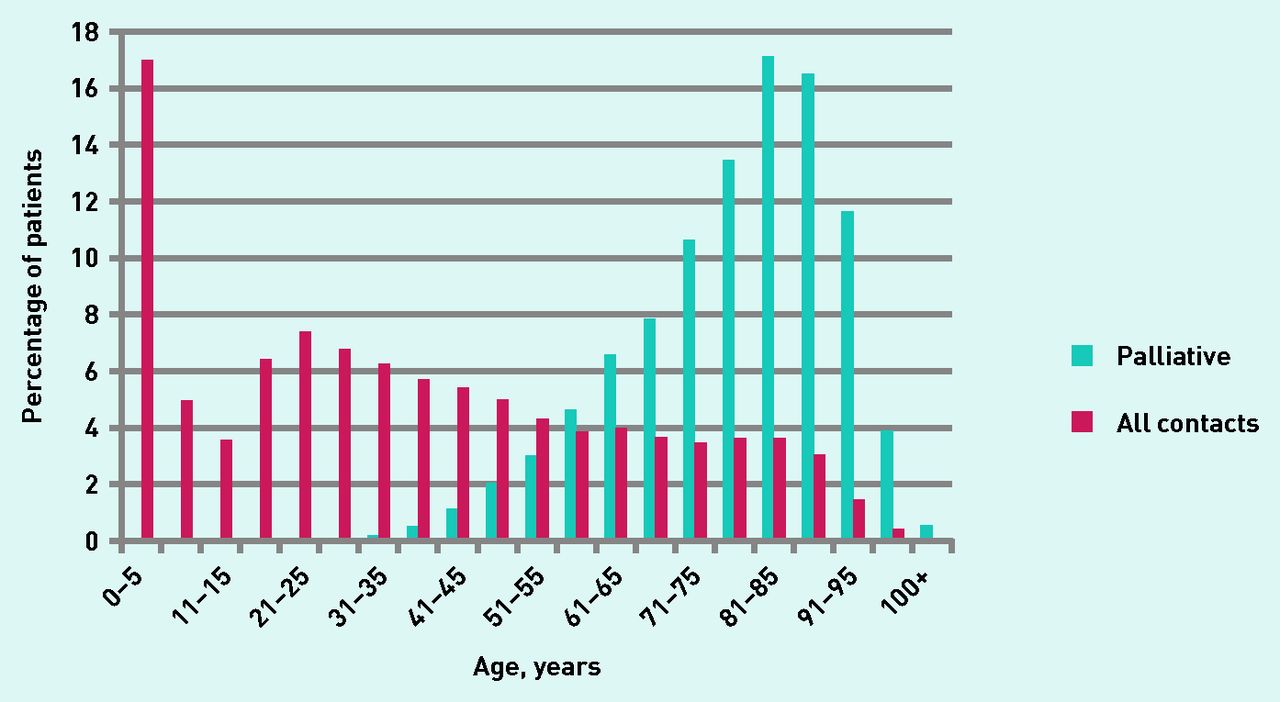
The median age of patients deemed ‘palliative’ presenting to the OOH service was 80 years, with an interquartile range of 70–90 years (Figure 1). The median age of the overall population of patients presenting to the OOH service was 33 years, with an interquartile range of 15–58 years. Of the patients with palliative care needs, 54.2% (2037) were female and 45.8% (1723) male, compared with 56.6% female and 43.4% male in the overall population presenting to OOH.
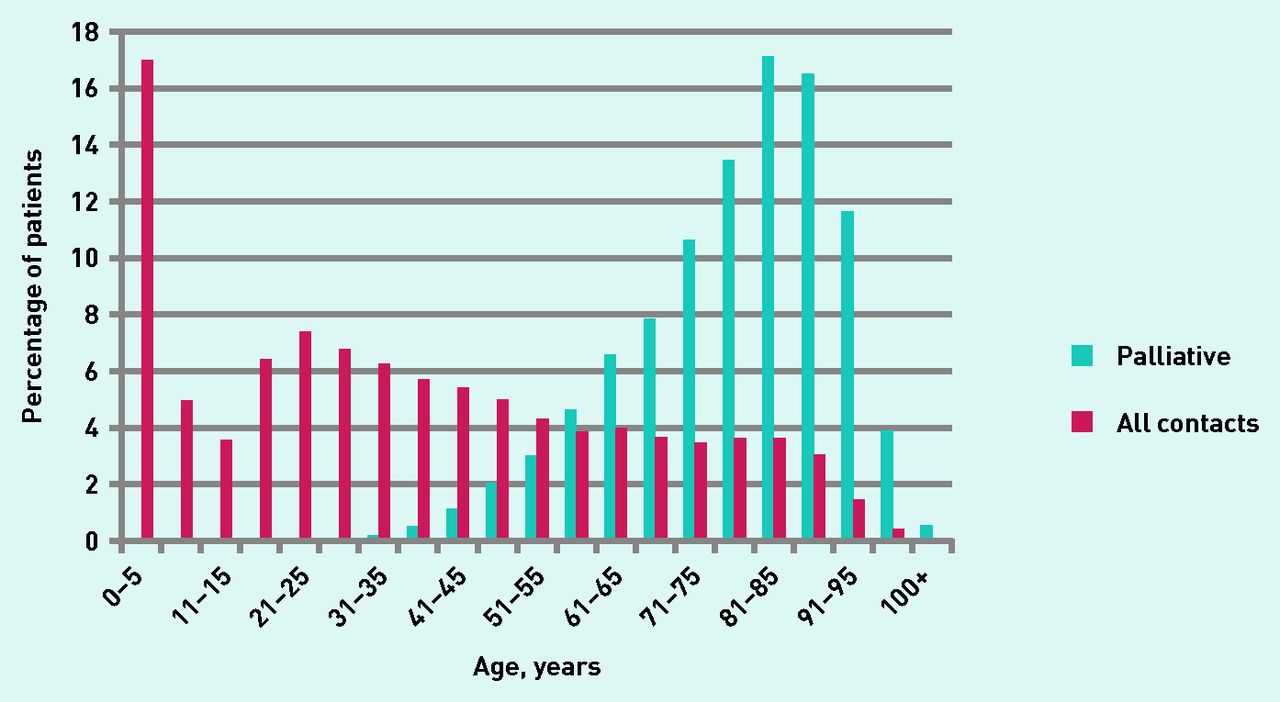
Age of patients presenting to the OOH service with a contact coded ‘palliative’ compared with all contacts to the OOH service.
Of the patients with ‘palliative’ codes, 37.8% were in the five most deprived deciles for Oxfordshire OOH contacts (Figure 2). To explore whether this difference was associated with the older age of patients with palliative care needs, age, sex, and IMD score were included in a multivariable logistic regression, which demonstrated a significant association between lower deprivation levels and contacting the OOH service with a problem coded ‘palliative’, in comparison with all other patient contacts with the service (OR 0.991, 95% CI = 0.988 to 0.994, P<0.001).

{kind=link}
{kind=link}
Number of patients coded as ‘palliative’ by IMD decile (local). Lower deciles are less deprived.
Patterns of service use for contacts coded ‘palliative’
Most palliative contacts (60.9%) were made at weekends (Saturday 30.2%, Sunday 30.7%), with the remaining contacts spread equally from Monday to Friday. Overall, 52.2% of palliative contacts were made during the daytime at weekends and public holidays, 28.5% of contacts were made during the evening, and 19.3% occurred overnight.
Disposition after OOH assessment
Sixteen different outcomes resulted from palliative patient contacts (Table 1). Of the 6045 contacts, 5.1% resulted in an acute admission. Of the remaining 94.9% whose care continued in the community, 41.8% required follow-up contact with their own GP (16.7% of these cases were asked to contact their GP, while in the remainder the GP was directed to contact the patient). In terms of outcomes, 10.4% involved referral to another community-based service, such as the district nurse or hospital at home team. In 34.8% of cases no follow-up was deemed necessary at the close of the consultation. For comparison, across the whole database of OOH contacts (for any reason), fewer (31.4%) contacts required follow-up with their own GP (19.4% were asked to contact their own GP), and more (46.6%) ended with no follow-up.
Disposition at end of consultation
Repeat contacts after initial OOH assessment
Of 3760 patients, 33.6% had at least one further contact with the service for a palliative problem. Over 6% of patients presenting to the OOH service with palliative care needs had four or more palliative contacts (Table 2). Where palliative patients were seen repeatedly with palliative care concerns by the OOH service, 64.4% of these additional contacts were within 3 days of a previous contact with the service.
Repeat presentations coded ‘palliative’
Primary versus secondary coding
Of the 6045 contacts coded by clinicians as ‘palliative’, ‘palliative care’ was the primary code in 5689 cases. Where ‘palliative’ was not the primary code, the most common primary code applied was ‘medication advice’ (n = 261), followed by ‘cardiac’ (n = 25), and ‘repeat prescription’ (n = 24).
DISCUSSION
Summary
At least 1.2% of patient contacts with the OOH service were for palliative problems. Given the 5.8 million contacts with OOH services in England per year, this would equate to around 69 600 patients per year contacting OOH services with palliative problems. Patients contacting the OOH service with palliative care needs do so predominantly during weekend daytime periods, and over a third will have more than one contact with the service. Patients are predictably older than the average population, but palliative contacts were relatively less deprived than contacts to the OOH service for all causes, even after adjusting for age and sex.
Strengths and limitations
To the authors’ knowledge, this is the first quantitative study to look at the usage of OOH primary care services by patients at the end of life. It adds to the qualitative exploration of the use of OOH services by patients at the end of life from Worth and colleagues8 and Leydon and colleagues.9 The use of electronic records by the OOH service has allowed a large dataset to be collected, spanning 4 years. The quality and comprehensiveness of electronic records is, however, variable. Although the clinical coding validation exercise provides some reassurance regarding the reliability of codes assigned by OOH service clinicians, reliance on coding practices of individual clinicians means that the number of patients coded as ‘palliative’ is almost certainly an under-representation of the true number of patients presenting with end-of-life problems (both because a clinician may have chosen another code, for example, ‘heart failure’ to describe a patient at end of life, and also because many people at the end of life have palliative care needs that are not recognised as such).10 In addition, it is recognised that patients with palliative care needs may access services out of hours via a variety of routes (including a small proportion whose own GP will have opted in to provide OOH care),3 and this study describes only the role of the OOH service.
Comparison with existing literature
Although the weekend daytime period represents a fifth of the hours covered by the OOH service, more than half the palliative contacts with the service were made during this period. This may reflect the constant medical need of this population; symptoms such as pain and syringe driver problems being just as likely to occur at weekends. High weekend service usage by patients with end-of-life needs also coincides with overall peak usage of OOH services.3 Although a link between times of peak usage and longer waiting times for home visits has not been documented, this could be of importance in a population in which pain is likely to be a common presenting complaint.11
Patients contacting the OOH service with palliative needs were relatively less deprived than contacts for all other causes. Among other factors, the present results may reflect increased awareness of and access to OOH services by more affluent patients, different service usage among different demographic groups, or simply the known trend for more economically deprived communities to have poorer access to health care.12 Overall, patients in the most deprived quintile are consistently most likely to die in hospital, whereas deaths in hospices are most common in the least deprived quintile.13 Although detailed data on the underlying diagnoses of patients contacting the OOH service for end-of-life care needs were not available for this study, access to such data might facilitate detailed exploration of the relationship between morbidity, deprivation, and service use. As patients at the end of life can access care via multiple different routes during the OOH period (for example, via direct contact with a local hospice or accident and emergency), an assessment of the levels of deprivation of patients accessing services by different routes is also required to fully understand the implications of the present findings for palliative care provision.
When compared with all contacts to the OOH service during this period, palliative contacts were more likely to end with a recommendation for GP follow-up. Moreover, the responsibility for arranging follow-up was more likely to be placed with the GP. The increased tendency of OOH clinicians to hand over these patients to their GP colleagues may reflect an attempt at establishing continuity of care for a patient group likely to have ongoing medical needs, and in whom the importance of such continuity is well recognised.14,15 This would suggest that better platforms for information sharing specifically for patients with palliative needs could improve both quality of care and clinician job satisfaction. The evaluation of electronic tools for information sharing such as the London-based ‘Coordinate my Care’ and the Scottish ‘Key Information Summary’ will provide useful direction on how information is most effectively shared.
A notably small proportion of contacts coded as ‘palliative’ resulted in acute hospital admission (5.1%). Although this may represent a desire on the part of clinicians to manage people at the end of life in their own homes, it is possible that more unwell patients self-triage directly to hospital services, bypassing OOH primary care.
Implications for research and practice
The present findings suggest that the needs of a large proportion of the patients presenting to OOH with palliative problems could be met by a dedicated service in the weekend daytime periods. Although some localities have linked third-sector provision of palliative care services with local hospice and hospital facilities to provide dedicated palliative care services out of hours,16 the resource implications of these services mean that for many areas of the UK the OOH primary care service will continue to provide the majority of unplanned end-of-life care. Work is required to explore whether dedicated services could facilitate faster access and be cost-effective. The success of any such service would rely on both accurate identification of patients with palliative care needs in the community, and effective communication and information sharing between service providers.
Patients at the end of life often have different needs and time frames of need from patients without need of palliative care. Many OOH services are accessed in the same way whether you are a teenager with a sore throat or a patient dying in pain. It is possible that the current ‘one-size-fits-most’ model of OOH primary care provision does not allow for the specific needs of patients who are dying in the community. A wider analysis of palliative patient flow through OOH services is now needed to identify if healthcare access at the end of life is inequitable, as well as the capacity requirements of a community-based palliative care service that can provide high-quality 24/7 care for patients at the end of life.
Acknowledgments
The authors acknowledge the contribution of Dr Mary Miller, Consultant in Palliative Medicine, and Ms Helen Hunt, Clinical Lead for Urgent and Ambulatory Care Services, Oxford Health NHS Foundation Trust.
Appendix 1. Structure of out-of-hours primary care in the UK with illustrative case study
Out-of-hours (OOH) primary care provides GP services outside of ‘core contracted hours’: from 18:30 to 08:00 Monday to Friday, and 24/7 at weekends and bank holidays. Since 2004, GPs have been able to opt out of providing 24-hour primary care cover for their practice population, and most have chosen to do so. Just 10% of practices have opted to retain responsibility for providing their own OOH care.10 For the remaining 90% of practices, the NHS commissions OOH services separately from in-hours services. Since April 2013, NHS England has delegated responsibility for this commissioning to 211 clinical commissioning groups. Hence the actual provider of the OOH service, and the exact way in which that service is delivered, will vary geographically within the country.
OOH service in practice: a case study example from the Oxfordshire OOH service
Mrs Smith is 84 years old and has advanced Alzheimer’s dementia. Her daughter Sarah visits after work on a Tuesday evening and is concerned about her mother. Mrs Smith is coughing, feverish, and has not eaten dinner.
Sarah phones ‘111’ on her mother’s behalf. Her call is answered by a trained call handler who works through an algorithm of questions (NHS Pathways) to determine the most appropriate and safe outcome for Sarah and her mother. The handler might call her an ambulance, direct her to the local OOH service, direct her to a clinician in 111, or give her simple self-management advice. In this case the handler directs Sarah to the local OOH GP service. She is told she will be contacted directly by them, and the 111 call ends. Sarah’s case is now transferred to the local OOH provider. It appears on their screen as needing a telephone consultation, with a priority assigned by the 111 call handler. A GP, Dr Jones, working on shift at the OOH centre picks up the call. Dr Jones works only for the OOH service. Some of her colleagues have jobs ‘in-hours’ in local GP practices too and therefore may know the patient; however, most patients will be unknown to the OOH GP.
Dr Jones rings Sarah to discover more about the situation with her mother and perform a telephone clinical assessment. She does not have access to Mrs Smith’s whole medical record, but, because Mrs Smith has been flagged up by her in-hours GP as near the end of life, the in-hours GP has e-mailed the OOH service some ‘special notes’. These tell Dr Jones that Mrs Smith has Alzheimer’s, and that she would like to be cared for at home if possible. Dr Jones listens to the history and, after assessment, decides that Mrs Smith needs to be seen for a further face-to-face assessment. Mrs Smith is unable to travel to the OOH centre, and so Dr Jones allocates a home visit. Once this is completed (by Dr Jones, or another colleague on shift that evening), her notes will be completed and a clinical code applied to the case. This code is at the discretion of the clinician (no formal coding training is given for either in- or out-of-hours GPs). Mrs Smith’s in-hours GP will immediately receive an e-mail notification from the OOH service containing the notes of the case so that they can see what has happened.
Notes
Funding
This study did not receive any external funding. Daniel Lasserson is funded by the NIHR Oxford Biomedical Research Centre and the views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received January 7, 2016.
- Revision requested March 1, 2016.
- Accepted April 22, 2016.
- © British Journal of General Practice 2016
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

