


INTRODUCTION
Hiccups is a reflex consisting of a sudden spasmodic contraction of the diaphragm causing shaking of the inspiratory muscles of the chest and abdomen, followed by the sudden closure of the glottis, which generates a characteristic noise of air being violently expelled from the lungs. The hiccup reflex consists of the afferent limb (phrenic nerve, vagus nerve, or thoracic sympathetic fibres), the central connection (not involving a specific centre), and the efferent limb (primarily the phrenic nerve).
Depending on their duration, hiccups are classified as transient hiccups (episodes lasting seconds or minutes), persistent hiccups (longer than 48 hours), and recurrent hiccups (episodes of hiccups more lasting than transient and often with frequent repetition). In most bouts of transient hiccups the aetiology is unknown. In the case of persistent hiccups the most frequent causes are gastro-oesophageal diseases (Table 1).1
Causes of persistent hiccups
This article describes an unusual cause of persistent hiccups and considers some of the remedies that can be used for the condition.
CASE REPORT
A 68-year-old man with a history of smoking (20 pack–years) and a left upper lobe lobectomy for tuberculosis 50 years ago, came to his primary care doctor following about 10 days of persistent hiccups, malaise, and costal and lumbar pain of mild intensity. A blood test was requested and omeprazole 20 mg daily was prescribed.
The patient came back 6 days later to collect the blood test results, with symptoms persisting. The tests revealed slight leucocytosis, C-reactive protein elevation (14.29 mg/dL), erythrocyte sedimentation rate (84 mm/hr), total bilirubin (2.6 mg/dL), direct (0.7 mg/dL), indirect (1.9 mg/dL), and rheumatoid factor (63 UI/ml). He was referred to the emergency department for evaluation.
On admission his general condition was reasonable: lung auscultation revealed decreased breath sounds with scattered crackles. His abdomen was normal, and there was no temporal artery tenderness.
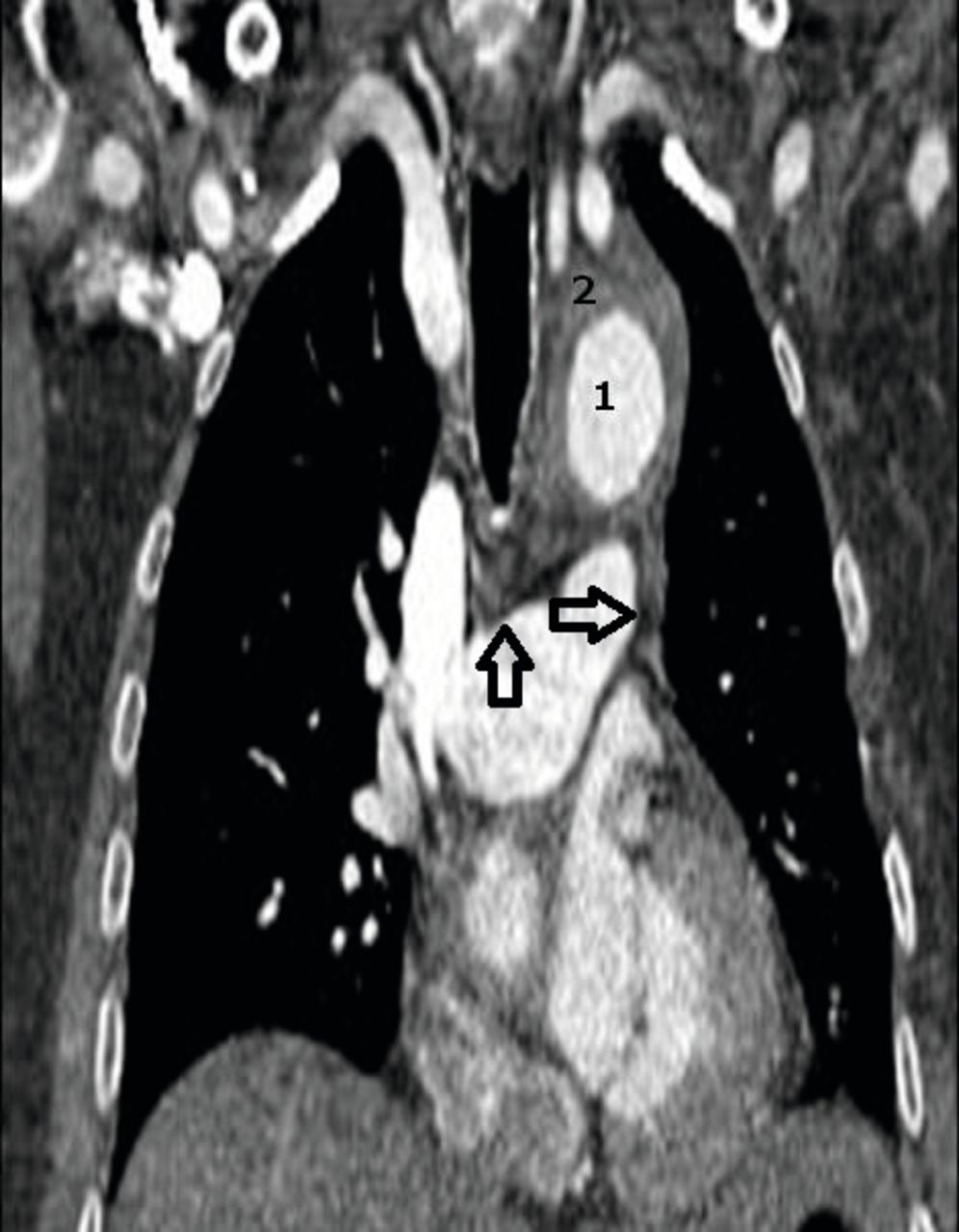
A chest X-ray (CXR) showed mediastinal widening. Thoracic computed tomography angiography was requested, and showed tissue surrounding the aortic wall, with diffuse circumferential swelling caused by an acute thoracic aorta intramural haematoma extending from the left subclavian as far as the renal arteries, with a maximum transverse diameter of 4.7 cm (Figure 1). The aortopulmonary window was occupied by the aortic haematoma (Figure 2), and there were two ulcers in the descending thoracic aorta (Figure 2). No signs of rupture or dissection were seen. A 6.7 cm infra-renal abdominal aortic aneurysm with large intramural thrombus associated with no signs of rupture was also discovered (Figure 3).

CTA sagittal image of thoracic aorta intramural haematoma (arrows). CTA = computed tomography angiography.
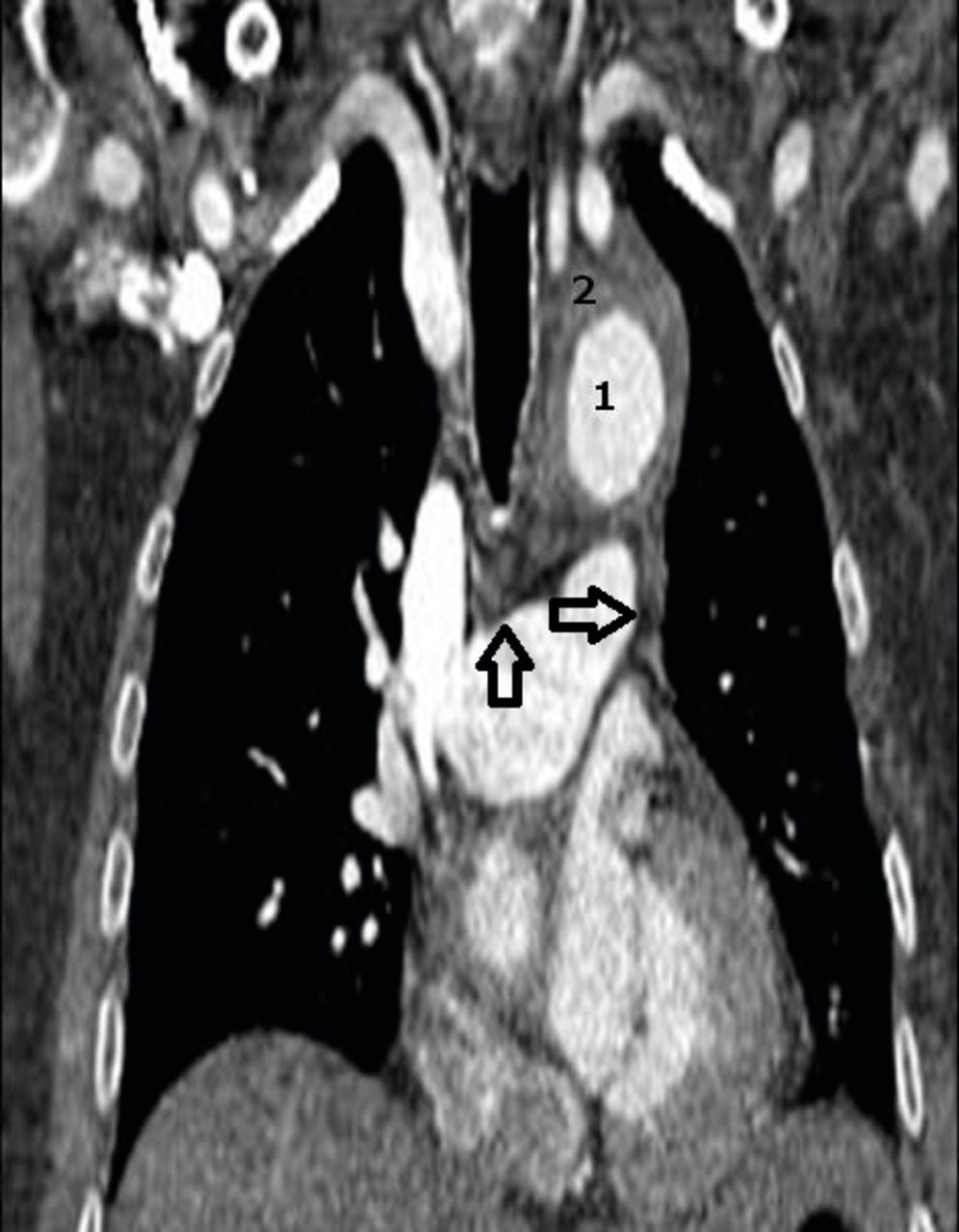
MPR coronal image: tissue surrounding aortic wall and diffusely circumferential swell that corresponds to the arterial wall haematoma aortic. (2) Aortic lumen. (1) This haematoma extends, partially occupying the aortopulmonary window (arrows). MPR = multiplanar reconstruction.

CTA axial image of thoracic aorta with parietal haematoma. (1) Aortic lumen. (2) Image of penetrating aortic ulcer (arrow). CTA = computed tomography angiography.
In order to seal the aortic ulcers and prevent haematoma progression, hybrid surgery (combining open and endovascular approaches) was performed several days after admittance. During surgery a haematoma in the ascending aorta was observed, with a bleeding point at the proximal graft anastomosis, and the defect repaired. However, at 72 hours after surgery, the patient became neurologically unreactive, despite having sedation suspended 36 hours before. A brain CT was reported as showing diffuse brain oedema with signs of tonsillar and bilateral uncal herniation, and intraventricular bleeding. Electroencephalogram (EEG) was reported as characteristic of brain electrical silence.
DISCUSSION
Most hiccup episodes are self-limiting and disappear after a few minutes. Despite being very frequent, they do not have any clinical repercussions, and medical care is not usually requested.
DIAGNOSIS
To target the cause of hiccups, it is very important to take a thorough clinical history, asking about smoking and drug misuse, and drugs, gastrointestinal symptoms (heartburn, dysphagia, regurgitation, or abdominal pain), cardiorespiratory symptoms (chest pain, cough, or dyspnoea), and neurological symptoms (headache, diplopia, dizziness, or abnormal sensitivity). An appropriate physical examination (vital signs, otoscopic, pulmonary and cardiac auscultation, and abdominal and neurological examination) must be conducted. When indicated, additional tests should be requested that are aimed at diagnosis (blood tests, chest X-ray, ECG, gastroscopy, abdominal CT, and cranial MRI) (Figure 4).1

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Evaluation of persistent hiccups. CT = computed tomography. CXR = chest X-ray. ENT = ear, nose, and throat. LFTs = liver function tests. LP = lumbar puncture. MRI = magnetic resonance imaging. Sx = symptoms.
In the present case, the CXR guided us to the diagnosis and CT was needed to confirm the cause of persistent hiccups: an acute aortic syndrome that caused thoracic aortic enlargement due to an intramural aortic haematoma. This haematoma extended to partially occupy the aortopulmonary window and presumably caused compression of the phrenic nerve that stimulates the diaphragm, which was an initial symptom of the patient with hiccups.
In the differential diagnosis of persistent hiccups, the following questions can help us: does it only happen when awake? Or does it occur day and night? In the first case the hiccups are probably functional and the causes are gastric dilatation, aerophagia, and gastro-oesophageal reflux disease. In the second case it is more likely to be due to toxic–metabolic causes, chronic alcoholism, oesophageal and gastric tumours, pleural involvement, mediastinal or diaphragmatic, or intracranial lesions.2 In children, or in an adult in whom all these causes have been excluded, the existence of a foreign body in the ear should be expected.2,3
COMPLICATIONS
Complications from hiccups are rare but they can occur and include discomfort, difficulty in feeding, gastro-oesophageal reflux, respiratory alkalosis (in tracheostomised patients), wound dehiscence, sleep deprivation, and psychiatric disorders.4
MANAGEMENT
The recommendations for treatment of transient hiccups are nasopharyngeal stimulation (drinking a glass of water, or inserting a tube through the nose as far as the back wall of the pharynx for 20 seconds), vagal stimulation (carotid sinus massage, cold compress to face, or induced vomiting), and respiratory manoeuvres (holding the breath, cough, Valsalva manoeuvre, or breathing into a paper bag). These manoeuvres are, in general, effective only in shortening an attack of acute hiccups and not in the treatment of persistent or recurrent hiccups.
The purpose of these manoeuvres is the attempt to interrupt the reflex arc thought to maintain repetitive diaphragmatic contractions.5 This is most often attempted by breath holding, the Valsalva manoeuvre, or breathing into a paper bag. Physiological studies have demonstrated a mechanism by which these manoeuvres improve hiccups, with the frequency of hiccups decreasing as arterial PCO2 rises.6
In the case of persistent hiccups, the following drugs are used: haloperidol 2–5 mg/24 hr, metoclopramide 10 mg, baclofen7 5 mg/8 hr, phenytoin, valproic acid, carbamazepine, gabapentin, amitriptyline, and amantadine.8 Chlorpromazine 25–50 mg intramuscularly or intravenously is effective in up to 80% of cases.
When hiccups fail to respond to the above therapies, other treatment options can be tried, including surgery, hypnosis,9 acupuncture,10 rectal massage,11 sexual stimulation,12 ejaculation13 (possibly as a result of the sympathetic stimulus stemming from ejaculation, which may terminate the reflex arc causing the hiccups), and even smoking marijuana.14
CONCLUSION
Most hiccup episodes are self-limiting and disappear after a few minutes. Despite being very frequent, they do not have any clinical repercussions, and medical care is not usually requested. But sometimes hiccups are a manifestation of a major disease, as in the case described in this article. Here, the origin of the hiccups was a thoracic aortic enlargement due to an intramural aortic haematoma likely to encourage direct contact with the phrenic nerve, which stimulated the diaphragm. To target the cause of hiccups, it is extremely important to obtain a thorough clinical history.
Acknowledgments
The authors would like to thank the patient’s family.
Notes
Patient consent
The patient’s family consented to the publication of this article and the images.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received March 16, 2016.
- Revision requested March 24, 2016.
- Accepted May 4, 2016.
- © British Journal of General Practice 2016
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

