


Abstract
Background Early diagnosis of HIV infection is a major public health issue worldwide. In 2009, the French National Authority for Health (Haute Autorité de Santé) developed specific guidelines and recommended mass screening of 15–70-year-olds across the general population. The guidelines were supported by communication directed at healthcare professionals, especially GPs.
Aim To assess the impact of the national mass screening policy on HIV testing.
Design and setting The study used data from the French National Health Insurance Fund database, from January 2006 to December 2013. Males and females aged 15–70 years, excluding HIV-positive individuals and pregnant females, were followed up throughout the 2006–2013 period. During the study period, 2 176 657 person-years and a total of 329 748 different individuals were followed up.
Method Standardised and non-standardised rates of HIV screening were calculated for each year; the impact of the policy was assessed using adjusted segmented regression analyses.
Results Overall, annual HIV screening rates increased over the study period, from 4.2% (95% confidence interval [CI] = 4.2 to 4.3) in 2006 to 5.8% (95% CI = 5.7 to 5.9) in 2013 with a more pronounced trend after 2010 (P<0.0001). This increase was more significant for those who regularly consulted a GP. For these individuals, the policy led to a 20.4% increase (95% CI = 17.0 to 23.8) in HIV screening in 2013 compared with only a 4.5% increase (95% CI = 4.4 to 4.5) for those who did not consult a GP regularly in 2013.
Conclusion The results show that the mass screening policy coordinated by GPs had a significant impact on HIV testing in France, which could result in positive impacts on public and individual health outcomes.
- HIV testing
- longitudinal studies
- mass screening
- policy evaluation
- primary care
- segmented regression analysis
INTRODUCTION
About 33 million people worldwide are infected with the human immunodeficiency virus (HIV).1 HIV is a major contributor to the global burden of disease.2 In 2010, HIV was the leading cause of disability-adjusted life years worldwide for people aged 30–44 years and the fifth leading cause for all ages.3 Globally, acquired immune deficiency syndrome (AIDS)-related deaths peaked at 2.3 million in 2005, and then decreased to 1.6 million by 2012.1 However, HIV incidence has remained static in Western Europe, despite the widespread use of antiretroviral therapy.4 In France, approximately 140 000 people are HIV-positive; among them, about 30 000 are unaware of the infection.5 Between 6000 and 8000 new HIV-positive diagnoses are made each year, with one-third of these at an AIDS stage. According to the French Institute for Public Health Surveillance (Institut de Veille Sanitaire, InVS), 47% of adults were not aware of being HIV-positive at the time AIDS was diagnosed, and 46% were heterosexuals who had been born in France.6
Arguing that early diagnosis of HIV infection could have an individual and collective positive impact,7–9 the French Health Authority (Haute Autorité de Santé) developed specific guidelines in 2009,10 followed by the French government, which established a national plan against HIV/AIDS and sexually transmitted infections.11 Both bodies recommended mass screening of 15–70-year-olds across the general population. The plan was supported by communication directed at healthcare professionals, especially GPs.12
Several studies have investigated the effect of screening programmes in middle- and low-income countries, for instance, by studying provider-initiated counselling and testing (PICT).13 In developed countries, some studies have investigated the effect of screening specific populations, such as those with a disease indicative of HIV infection;14 however, to the authors’ knowledge, none has investigated the effect of a national programme on HIV mass screening over time.
This study aimed to assess the impact of this national policy on HIV screening, launched in 2009, on a representative sample of the French general population aged 15–70 years, and evaluate the independent effect of the frequency of visits to GPs.
METHOD
Data
Data from the French National Information System of Public Health Insurance (Système National d’Informations Inter Régimes de l’Assurance Maladie) was used. This is a large health administrative database that provides exhaustive and detailed information on all reimbursed ambulatory care of people affiliated with any of the main French health insurance funds (that is, 98% of the population). Researchers worked on the basis of the Generalist Sample of Beneficiaries (EGB) based on a survey at the 97th percentile on the national health insurance number of French health insurance beneficiaries. This constituted a representative sample of the French general population in terms of age, sex, and geographical location, and included >700 000 individuals.15 The time span between January 2006 and December 2013 was assessed to include sufficient lengths of time both before and after the policy intervention (introduced in 2009).
How this fits in
Most of the research to date agrees on the positive effects, in terms of morbidity reduction, of early diagnosis of HIV infection. To the authors’ knowledge, this is the first study to demonstrate, in a developed country, the positive and significant impact of a national mass screening policy, coordinated by GPs, on HIV screening rates. The results suggest that broadening the target of HIV screening, by increasing HIV screening rates, could have a positive impact on public and individual health. The cost-effectiveness of such a policy remains to be demonstrated.
Intervention
The National Plan against HIV/AIDS advised GPs to be aware of opportunities for broad screening in people not recently tested. The programme consisted in leaflets sent to GPs, recommending that they pay attention to carrying out HIV screening among their patients in a more systematic way, independently from their level of risk for HIV infection. Thus, GPs were at the forefront of the screening programme.
Inclusion and exclusion criteria
The inclusion criteria for the study were being male or female, aged 15–70 years, affiliated to the general social security scheme (régime général de la sécurité sociale), and alive during the 2006–2013 period. Individuals with a history of HIV infection and pregnant females, where HIV testing is systematically prescribed, were excluded.
Primary outcome: screening test for HIV
Using the codification for a serodiagnosis of HIV infection from the EGB database, a binary outcome variable was adopted, where ‘1’ was used for an individual who had undergone a screening test for HIV prescribed by any specialist in ambulatory care within that current year; otherwise, a ‘0’ was recorded.
Independent variables
The main independent variable was the frequency of GP visits because they were the main target of the intervention. This was scored as ‘1’ if the individual had seen a GP at least once during the year, and scored as ‘0’ otherwise. The control variables were sex, age, and geographical location. Geographical location was divided into four subgroups: Île de France (except Paris); Paris; ‘Overseas’ including the five French departments of Guadeloupe, Réunion, Mayotte, Guiana, and Martinique; and the rest of France (labelled ‘Other’). Overseas departments were considered a specific subgroup because HIV prevalence is higher than in other French departments. According to the InVS, the HIV incidence rate was 44 new contaminations per 100 000 person-years in overseas regions in 2009, compared with 18 new contaminations per 100 000 person-years overall in France.5
Statistical analyses
Unadjusted rates for the numbers of patients having undergone a screening test for HIV were computed for each individual year between 2006 and 2013. Data were plotted to assess any changes in HIV screening overall and for any changes after the policy intervention. The crude rates were then computed for different subpopulations stratified by sex, age, geographical location, and frequency of GP visits.
A segmented regression model for the outcome variable was used to assess the trend of HIV screening each year both before and after the policy intervention.16,17 The segmented regression was implemented using the generalised estimating equation technique by specifying a logit link function and autoregressive correlation structure. The estimated model is shown below:
 where pit denotes the probability that an individual i was screened in year t; timet is a continuous variable indicating time in years at time t from the start of the observation period (timet = 0 in 2006 and timet = 7 in 2013); interventiont is an indicator of time t occurring before 2009 (included) (interventiont = 0) or after 2009 (interventiontt = 1); and time after interventiontt is a continuous variable that includes the number of years after the intervention at time t, coded 0 before 2009 (included) and timet, coded −3 after 2009. Thus, β1 was interpreted as the trend in HIV screening before the policy intervention; β2 was the level after the intervention; and β3 was the slope’s trend after the intervention. The model was adjusted according to sex, age group, geographical location, and frequency of GP visits.
where pit denotes the probability that an individual i was screened in year t; timet is a continuous variable indicating time in years at time t from the start of the observation period (timet = 0 in 2006 and timet = 7 in 2013); interventiont is an indicator of time t occurring before 2009 (included) (interventiont = 0) or after 2009 (interventiontt = 1); and time after interventiontt is a continuous variable that includes the number of years after the intervention at time t, coded 0 before 2009 (included) and timet, coded −3 after 2009. Thus, β1 was interpreted as the trend in HIV screening before the policy intervention; β2 was the level after the intervention; and β3 was the slope’s trend after the intervention. The model was adjusted according to sex, age group, geographical location, and frequency of GP visits.
As the policy intervention was expected to have different effects according to the frequency of GP visits, the model was also estimated separately for individuals who did not visit a GP within the year (GP = 0), and for individuals who visited a GP at least once within the year (GP≥1).
To quantify the impact of the intervention on HIV screening (overall and according to the frequency of GP visits), the probabilities for performing a screening test for HIV annually were simulated, both with and without the policy intervention (that is, the counterfactual scenario). For each year after 2010, the absolute policy effect was estimated using the formula:

The policy impact was then expressed as a percentage with a 95% confidence interval (CI).18
RESULTS
Descriptive statistics
During the period 2006–2013, 2 176 657 person-years and a total of 329 748 different individuals were followed. The descriptive statistics are presented in Table 1.
Descriptive statisticsa
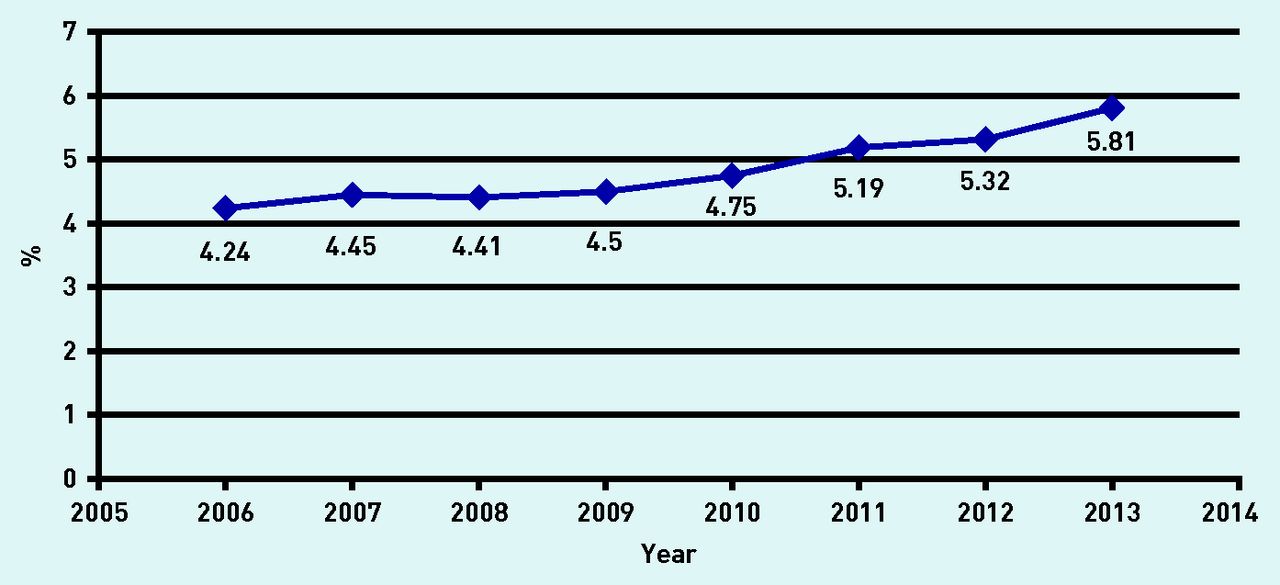
The unadjusted rates of patients who had undergone a screening test for HIV are presented in Figure 1, and Appendix 1 provides the exact numbers/rates of screening tests together with the 95% CIs. There was a significant increase in HIV screening across time, from 4.2% (95% CI = 4.2 to 4.3) in 2006 to 5.8% (95% CI = 5.7 to 5.9) in 2013, and the trend is more pronounced after 2010.

Patients aged 15–70 years who underwent a screening test for HIV between 2006 and 2013: unadjusted HIV screening rates.
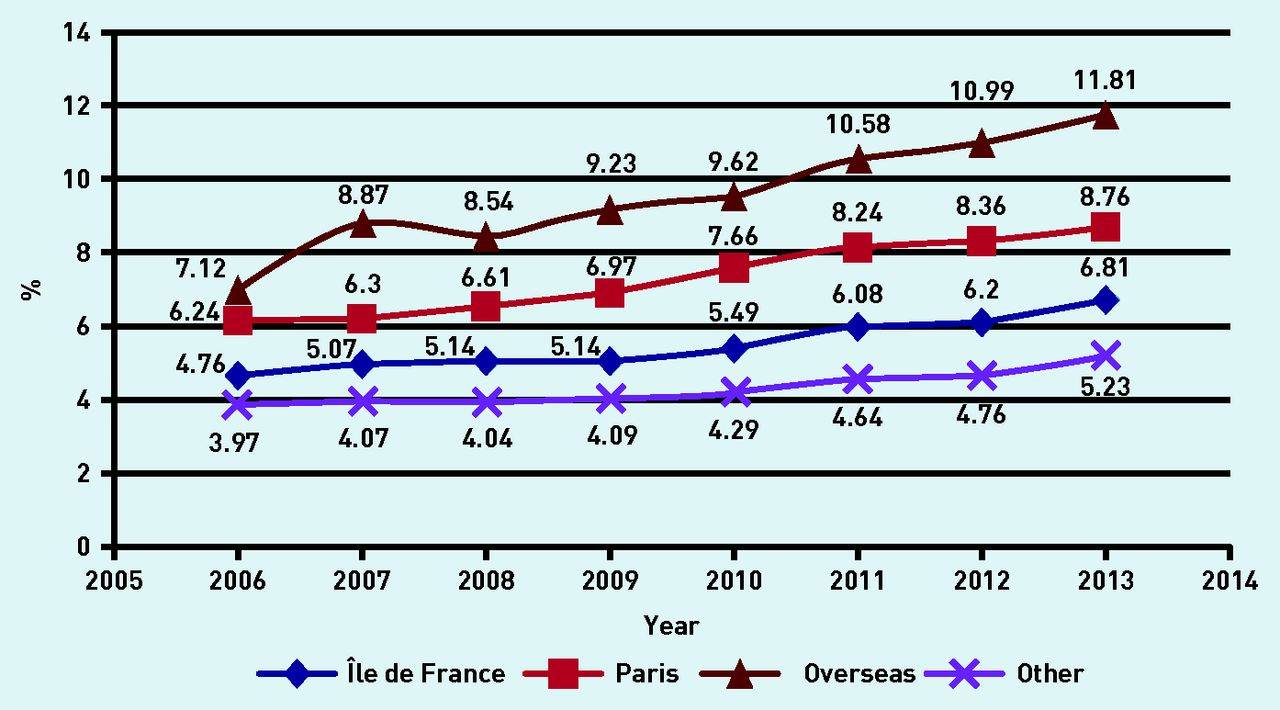
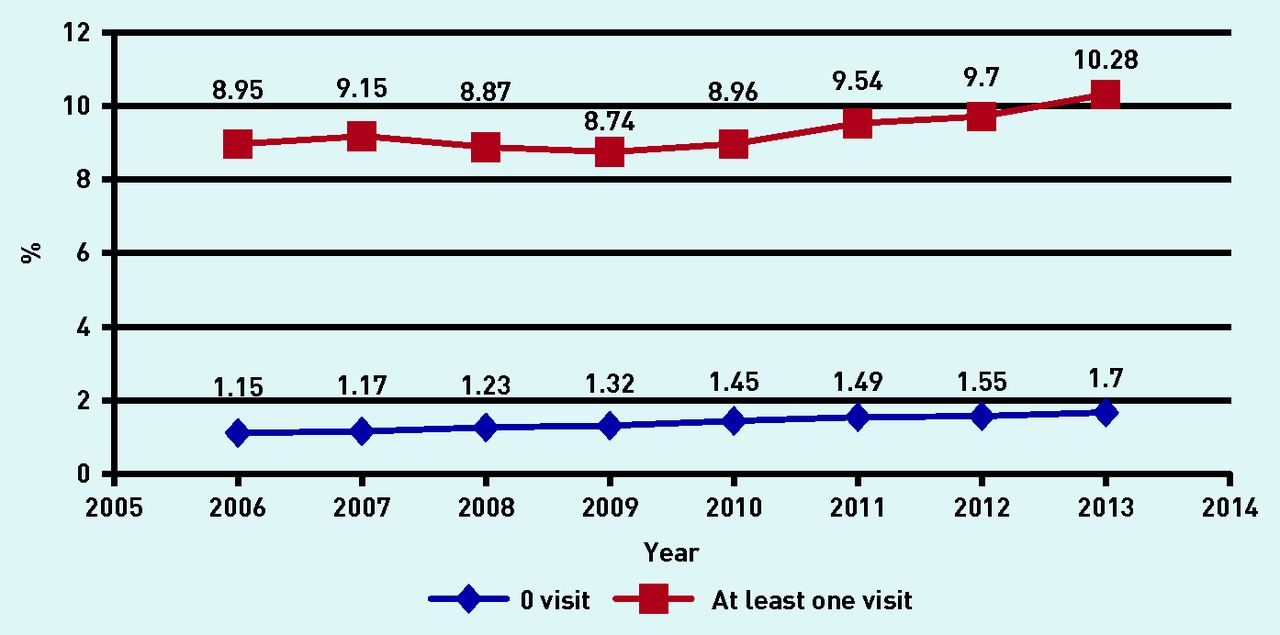
The rates of patients who underwent a screening test for HIV (hereafter referred to as ‘the screening rates’), stratified by sex, age, geographical location, and frequency of GP visits, are shown in Figures 2⇓⇓–5. The screening rates were significantly higher for females compared with males (P<0.001), and for both of these subgroups there was a significant increase in HIV screening rates over time (P<0.0001). The highest screening rates were recorded for the 15–29-year age subgroup with a statistically significant increase over time (from 5.9% in 2006 to 9.5% in 2013, P<0.0001), and were lowest for those aged 45–70 years. There were strong disparities in HIV screening according to geographical location: the screening rates were highest in patients living overseas; the second highest rate was in Paris; and the lowest rates were recorded in the other metropolitan regions. Overall, the screening rates were about seven times higher for individuals who visited a GP at least once a year compared with individuals who did not visit a GP. For this subgroup, there was a significant increase in HIV screening over time, from 9.0% in 2006 to 10.3% in 2013.

Trends for HIV screening between 2006 and 2013. HIV screening rates stratified by sex.
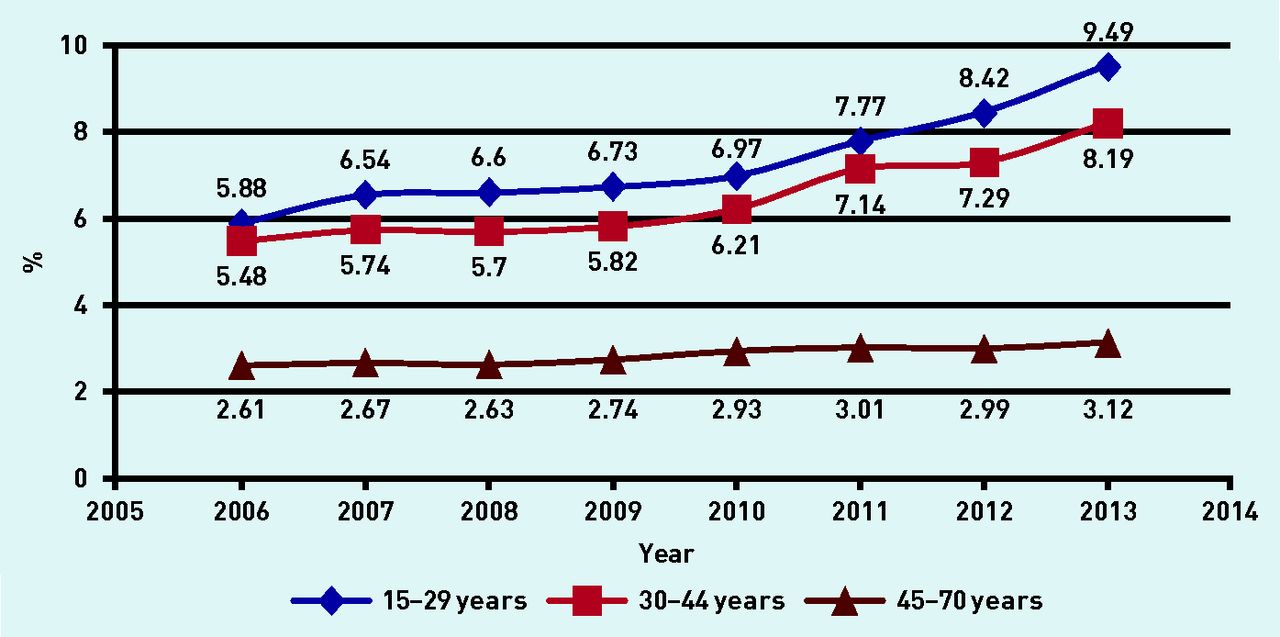
Trends for HIV screening between 2006 and 2013. HIV screening rates stratified by age.

Trends for HIV screening between 2006 and 2013. HIV screening rates stratified by region.

Trends for HIV screening between 2006 and 2013. HIV screening rates stratified by number of GP visits.
Segmented regression model results
The results from the segmented regression model, both with and without stratification for the frequency of GP visits, are presented in Table 2. Overall, that is, in the ‘pooled model’, and in the subgroup who visited a GP at least once a year, there was no significant trend in HIV screening before the policy intervention (P = 0.42). Overall and in the two subgroups stratified by GP visits, there was no significant change in the level of HIV screening immediately after the policy intervention (P = 0.29, P = 0.22 and P = 0.15, respectively). Overall and in the subgroup that made at least one visit annually to a GP, there was a positive and significant trend after the policy intervention (P<0.0001); the effect was not significant for the subgroup that did not visit a GP (P = 0.93).
Results from the segmented regression models
Simulations and impact of the policy
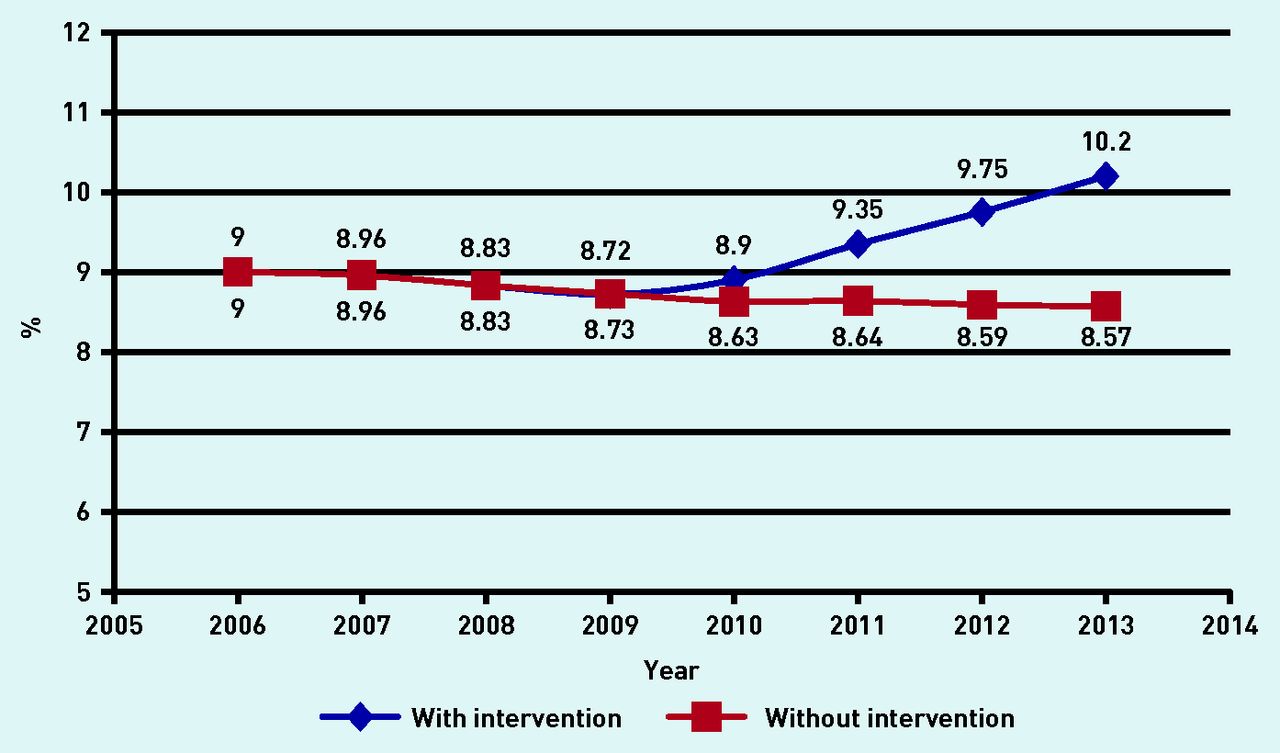
The stratified and non-stratified simulated probabilities of HIV screening are presented in Figures 6⇓–8 and the impacts of the policy intervention are presented in Table 3. As expected, the intervention had the largest impact on the subgroup that regularly visited a GP. For this group, the intervention led to a 3.3% increase (95% CI = 2.8 to 3.8) in HIV screening in 2010, an 8.7% increase (95% CI = 7.4 to 10.1) in HIV screening in 2011, and a 20.4% increase (95% CI = 17.0 to 23.8) in HIV screening in 2013. The intervention led to a 19.2% increase (95% CI = 16.5 to 22.0) in HIV screening in 2013 for the entire population, but only a 4.5% increase (95% CI = 4.4 to 4.5) for the subgroup that did not visit a GP regularly.
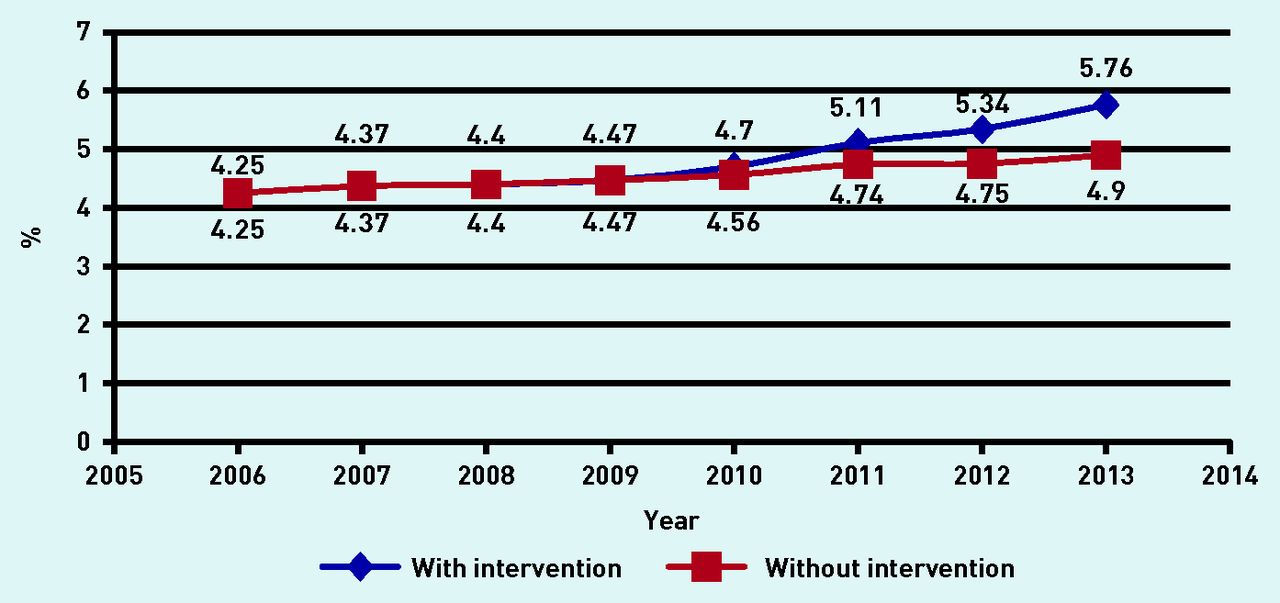
Simulated probabilities of HIV screening between 2006 and 2013, with and without policy intervention. Simulated probabilities of HIV screening overall.
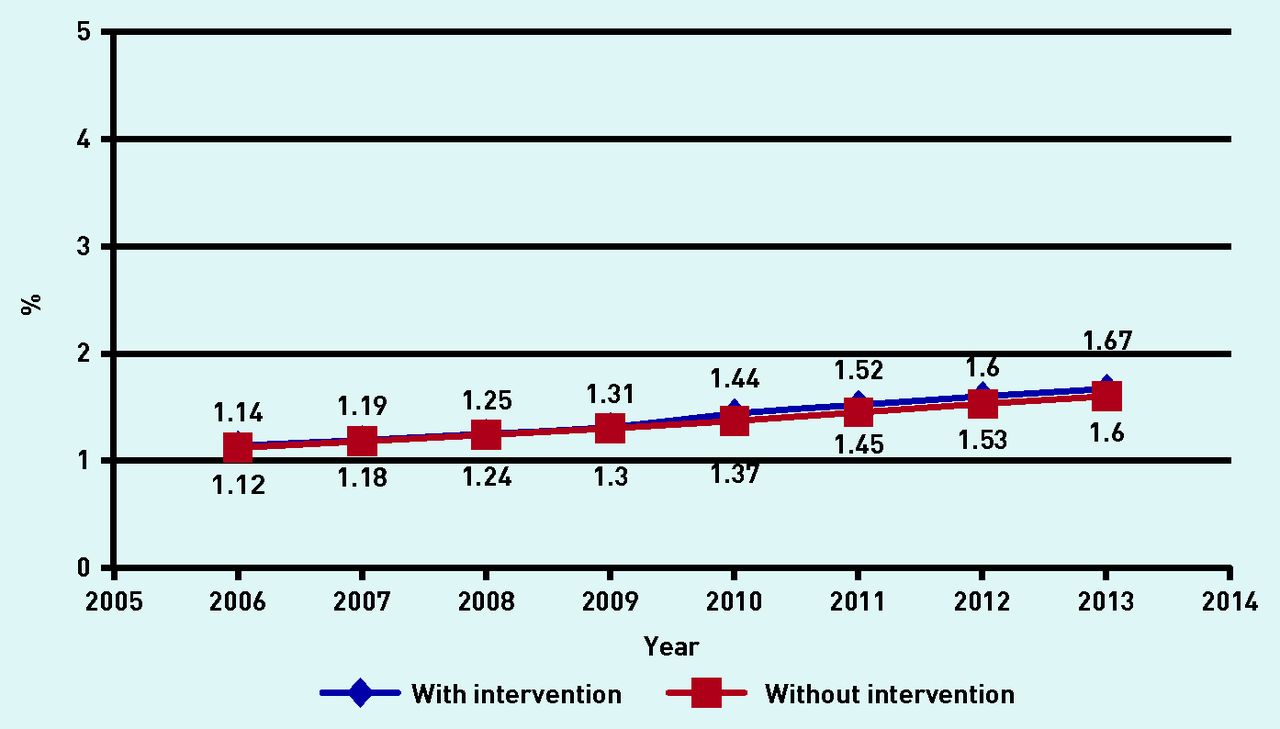
Simulated probabilities of HIV screening between 2006 and 2013, with and without policy intervention. Simulated probabilities of HIV screening when GP visits = 0.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Simulated probabilities of HIV screening between 2006 and 2013, with and without policy intervention. Simulated probabilities of HIV screening when GP visits ≥1.
Simulated percentage increases in HIV screening due to the policy intervention
DISCUSSION
Summary
The results show that, overall, the rates of HIV screening increased during the study period, especially after the launch of the national policy in 2009. Simulations on the impact of the policy showed that the intervention led to a large increase in HIV screening for individuals who regularly saw a GP compared with a much lesser increase for those who did not see a GP regularly.
Strengths and limitations
The large sample size and its representativeness of the French general population are the two main strengths of this study. In addition, on the basis of the administrative records, an objective measure of HIV screening was constructed and the long-term changes were followed up.
However, the study has some limitations. First, the screening rates did not take into account the fast diagnosis tests (tests rapides d’orientation diagnostique), which were infrequently conducted during the study period. There were 32 000 tests in 2012, that is, less than 0.002% of HIV screening tests performed in 2012.19 A second limitation, inherent to any non-randomised analysis, was that it was not possible to state with confidence that the estimated increase in HIV screening rates after 2010 was only caused by the policy intervention. However, to the best of the authors’ knowledge, no other policy that targeted the French general population was implemented simultaneously. Because it was possible to show that the policy intervention had no impact on those individuals who did not regularly visit a GP, and because the policy especially targeted GPs, this subgroup could be considered as the ‘control’ group.
Comparison with existing literature
To the authors’ knowledge, this is the first study in a developed country to assess the impact of a national mass screening policy on HIV testing. In the UK, national guidelines on HIV testing were published in October 2008 by the British HIV Association.20 These guidelines were intended to promote an increase in HIV testing, but did not recommend HIV mass screening. They targeted specific populations, such as those with a disease indicative of HIV infection or new registrants in primary care who lived in regions where there was a diagnosed adult HIV prevalence >2 per 1000 population. A meta-analysis published in 2014 found that the estimated percentage of patients eligible for HIV testing and who received a test was 27.2% (95% CI = 22.4 to 32.0).14 This low level of testing suggests that adherence to the 2008 UK guidelines for HIV testing was poor in recommended populations. The authors of the report believe that the low overall level of testing was because HIV screening was not promoted enough rather than the patients’ willingness to be tested. In 2003, the UK implemented a similar policy initiative to the French one discussed here. A screening programme against Chlamydia infection was proposed in primary care for males and females aged <25 years. The policy seems to have had positive outcomes: in 2009, 16% of individuals aged 15–24 years were screened and 7.6% of the tests were positive.21
In the USA, in 2006, the Centers for Disease Control and Prevention recommended HIV screening in all healthcare settings for all individuals aged 13–64 years, regardless of risk, who were seen at facilities, with a prevalence of undiagnosed HIV infection ≥0.1%. They also recommended annual screening for patients who were known to be at risk for HIV infection.22 In areas of ≥0.1% prevalence, only 25 healthcare settings (6.6%) reported screening all patients for HIV, whereas 131 (34.8%) reported screening only some patients.23
In 2007, the World Health Organization recommended PICT for HIV counselling and testing in health facilities as a standard element of medical care during HIV epidemics in low- and middle-income countries. This was proposed to expand on the current practices of client-initiated voluntary counselling and testing.24 PICT capitalises on contacting all patients within the medical system, and this can be used as an opportunity to carry out HIV testing and diagnosis, and to provide links to care.25 PICT seems to be an effective public health intervention that increases access to HIV counselling and testing, and reduces the number of missed opportunities for testing.26
Implications for research and practice
The results of this study suggest that the national plan increased HIV screening, and that GPs played an important role in its implementation. This could have a positive impact on public and individual health for the following reasons:
60% of people unaware of their HIV status have a CD4 count ≤500 cells/mm3 and are thus eligible to receive antiretroviral treatment; males have a lower CD4 count than females;27
the death rate in France at 4 years for patients with advanced-stage AIDS or a CD4 count <200 cells/mm3 is estimated at 6.7%, whereas it is estimated at only 1.4% for patients who are treated earlier;28 and
moreover, the probability of changing sexual conduct by adopting preventive behaviour is 2–3 times greater when the HIV-positive status is known than when it is ignored or feared.29
A strategy of mass screening faces several difficulties because HIV transmission is mostly associated with sexual intercourse; consequently, screening is related to sexuality, which is often seen as questioning the faithfulness of one’s partner or spouse.30 Moreover, some GPs may be reluctant to systematically address the possibility of HIV and to offer a test.31 This is why the Morlat report32 invited GPs to initiate a proposal for HIV testing that focuses on the simple message of paying attention to the classic clinical situations and monitor the opportunities for broad screening in people not recently tested as and when the opportunity arises. Routine testing could dispense with the ineffective results from referral-based risk testing33 and would reduce stigma and discrimination.34
The question of cost-effectiveness of HIV mass screening is still highly debated. In France, screening in emergency departments showed a modest impact of non-targeted HIV screening.35 However, an early model based on cost-effectiveness36 showed that mass screening could have favourable cost-effectiveness ratios. Similar results have been found in Portugal.36 Expanding HIV testing in healthcare and community services is also encouraged in England, where the 2011 Health Protection Agency guidelines suggested that HIV testing should be widely promoted by GPs, especially in areas of high prevalence.20
This study showed the positive impact of a national mass screening policy on HIV testing, especially for individuals who regularly visited a GP. However, it was not designed to evaluate newly-detected HIV cases or to appraise the cost-effectiveness of such a policy. Further studies are needed to investigate these issues.
Acknowledgments
The authors thank the Caisse Nationale d’Assurance Maladie des Travaileurs Salariés (CNAMTS) for providing access to the data.
Appendix 1. Unadjusted numbers and rates of patients who underwent a screening test for HIV between 2006 and 2013
Notes
Funding
None.
Ethical approval
This study was planned as a research project. All precautions were taken to ensure anonymity of the data, in agreement with the CNIL (Commission Nationale de l’Informatique et des Libertés, French law no. 78–17). According to the French law, written informed consent was not required for this type of study.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received January 27, 2016.
- Revision requested April 15, 2016.
- Accepted May 9, 2016.
- © British Journal of General Practice 2016
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

