


INTRODUCTION
Sore throat is a common presentation to general practice and national guidelines are available to aid in the management of acute cases.1 Chronic cases of sore throats, however, can pose diagnostic and management dilemmas for many GPs because clinical guidelines are lacking and routine investigations may be normal. Here we describe a previously unreported presentation of eosinophilic oesophagitis (EO) as a cause of chronic sore throat and demonstrate the importance of serial oesophageal biopsies and food allergy testing in patients with chronic symptoms. EO does not affect mortality but untreated disease can cause oesophageal stricturing.
CASE REPORT
A 46-year-old male with no significant past medical history presents to his GP with a sore throat, made worse on swallowing, for a month. Physical examination was normal, and the patient was reassured that it was a viral infection and his symptoms should resolve with lozenges. A month later, he re-presents with ongoing symptoms. The GP, suspecting gastro-oesophageal reflux disease, prescribes a 2-month course of proton-pump inhibitor (PPI) but it made no difference to his symptoms. A referral was made to the ear, nose, and throat clinic where transnasal oesophagoscopy and routine blood tests were completely normal. A diagnosis of globus pharyngeus was made and the patient was reassured then discharged back to the care of his GP.
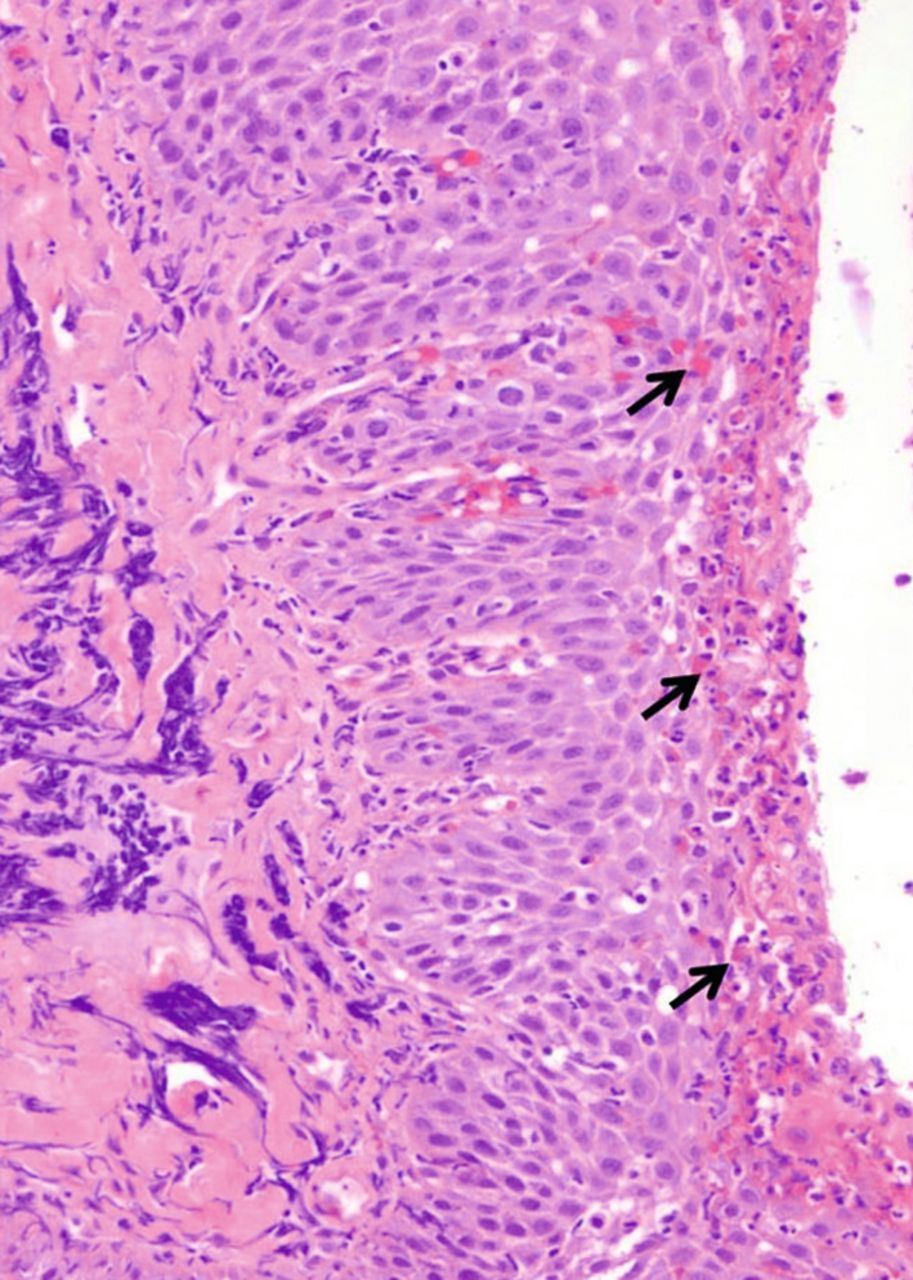
Symptoms persisted for several months and the patient was referred to a gastroenterology clinic but later discharged due to the lack of gastrointestinal symptoms. Seven months after initial presentation, he developed pooling of saliva due to severe odynophagia. The GP refers the patient for an urgent oesophago-gastro-duodenoscopy (OGD), which was reported as macroscopically normal. Random biopsies were taken of the proximal, mid, and distal oesophagus. Histology reports were returned 2 weeks later demonstrating significant eosinophilic infiltration (Figure 1) in all oesophageal biopsies consistent with EO.
{kind=link}
Cross-sectional histology of the oesophagus. The black arrows indicate infiltration of eosinophils within the squamous cell layer of the luminal surface (H&E staining, original magnification ×200).
Subsequently, the patient underwent serological food allergy testing, which revealed he had developed multiple food allergies including milk, wheat, soya bean, fish, shrimp, and hazelnut. He was seen by a dietician and an allergy specialist but showed little response to ingested budesonide aerosols. The patient was referred back to the gastroenterology clinic and, after commencement of oral budesonide, montelukast, and a strict exclusion diet, is now symptom free.
DISCUSSION
EO affects people of all age groups and ethnicities, with prevalence most common among males and Caucasians.2,3 Its exact aetiology is unknown, although it is associated with an immune-mediated reaction and the majority of sufferers have either personal or family history of other allergic conditions.4 The presentation of EO is often vague and nonspecific resulting in misdiagnosis. In adults, the most common presenting symptoms are intermittent dysphagia and dyspepsia.4,5 In children, the presentation is more variable with symptoms such as regurgitation, abdominal pain, vomiting, and failure to thrive.4,6 EO does not affect mortality but untreated can cause oesophageal stricturing.
UK guidelines on the diagnosis and management of EO are lacking though guidelines are available from the American College of Gastroenterology3 and parallels usual practices in gastroenterology within the UK. A diagnosis of EO is made on the basis of the clinical, endoscopic, and histological findings. Unfortunately both clinical and endoscopic findings can be hugely variable with no specific features pathognomic of the disease.2,3 Endoscopic appearances in EO can range from apparently normal mucosa to non-specific inflammatory features such as proximal strictures, pinpoint exudates, multiple concentric oesophageal rings (also known as trachealisation of the oesophagus or ‘feline oesophagus’), vertical furrowing (‘tram tracks’ sign), white plaques, and absent vascular markings.2,3 In severe cases of EO, the oesophageal mucosa becomes friable and tearing of the mucosa following passage of the endoscope may occur — the so-called ‘crepe paper’ sign.2 It is noteworthy that these endoscopic findings alone are not specific to EO, for example, oesophageal dysmotility or spasms may also give appearances of oesophageal trachealisation. This lack of specificity highlights the importance of serial mucosal biopsy in aiding diagnosis.
Oesophageal biopsies should be taken both proximally and distally, with additional targeted biopsies from macroscopically abnormal areas. Histologically, eosinophilic infiltration is seen in the squamous layer of the oesophagus (>15 eosinophils per high-power field), which is usually devoid of eosinophils.2 Importantly, all changes are limited to the oesophagus with gastric and duodenal mucosa remaining normal, thus differentiating EO from other secondary disease processes where eosinophilic infiltration is also seen, as in gastro-oesophageal reflux disease (GORD), connective tissue diseases, and parasitic infections.2
Once eosinophilic infiltration has been demonstrated, it is recommended that patients should be given a trial of high-dose PPI for 4–8 weeks followed by a repeat endoscopy.2,7 In patients with persistent symptoms and eosinophilic infiltration despite PPI therapy, EO can be formally diagnosed.3 This step is important in distinguishing EO from GORD where eosinophilic infiltration is caused by reflux, and Proton Pump Inhibitor-Responsive Oesophageal Eosinophilia (PPI-REE), a primary autoimmune disorder that causes eosinophilic infiltration in the absence of reflux3 but resolves with PPIs.
EO, PPI-REE, and lymphocytic oesophagitis (LO) make up a group of disorders termed ‘infiltrative oesophagitis’, which is characterised by the infiltration of atypical cells within the oesophagus. Like EO, LO often presents with dysphagia, though incidences of food impaction and stricturing are less frequent.8 LO is characterised by lymphocytic infiltration of the oesophagus, although it is not yet clear if LO is a distinct clinical condition or a consequence of other forms of chronic oesophageal inflammation such as GORD.8 LO has been associated with inflammatory bowel disease in children,9 although not in adult studies. Endoscopy tends to be normal macroscopically though oesophageal rings are not uncommon.8 Histologically, increased lymphocytic infiltration is characteristically seen in the middle and distal third of the oesophagus. Unlike EO, PPI administration tends to improve symptoms in LO though it does not provide a cure. Whether this effect is due to the direct treatment of LO or the treatment of concomitant GORD is as yet unclear. Efficacy studies of alternative therapies (for example, steroids) in the treatment of LO are still required.8
The treatment of EO is avoidance of allergens and corticosteroid administration. Food allergy testing should be conducted in all patients with suspected or confirmed EO, with large numbers demonstrating positive testing.2 If an allergy is identified, dietary elimination with support from a dietician should be implemented. In incidences where this fails to control symptoms, corticosteroids can be administered, though a combined approach is often adopted in the UK. A topical corticosteroid (for example, using swallowed fluticasone or budesonide aerosols) is the first line of steroid treatment. If this fails, oral steroid therapy is used.2,3 Endoscopic treatment may be indicated in order to treat food impaction and oesophageal stricturing, but due to the associated risk of perforation this is generally reserved for occasions where medical therapy has failed.2,3 Another potential therapy is the leukotriene inhibitor montelukast, though evidence for its use remains limited at present.10
CONCLUSION
Patients with chronic sore throat, where blood tests and transnasal oesophagoscopy or laryngoscopy are normal, are commonly diagnosed as globus pharyngeus or ‘functional sore throat’. Patients with atypical presentations of EO may also be misdiagnosed by gastroenterologists as in this case. This paper highlights the importance of performing food allergy testing, OGD, and oesophageal biopsies in cases of chronic sore throat in order to exclude EO and other less common causes of infiltrative oesophagitis such as LO. It is also noteworthy for GPs that, since May 2016, changes have been made to the diagnostic guidelines of globus pharyngeus, which now recommends EO as an exclusion criterion before the diagnosis can be made.11
Notes
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received July 1, 2016.
- Revision requested July 11, 2016.
- Accepted July 19, 2016.
- © British Journal of General Practice 2017
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

