


Abstract
Background In the UK, GPs play a key role in the identification and management of children, young people, and adults on the autism spectrum, but there is a paucity of research on GPs’ perceptions of working with these patients.
Aim To understand GPs’ perceived self-efficacy in identifying and managing their patients on the autism spectrum, and the factors affecting this.
Design and setting An online self-report survey was developed for completion by GPs across the UK.
Method A total of 304 GPs in the UK took part. The survey collected responses on participants’ background, training, and experience, both as a GP and with regard to autism, and included a 22-item knowledge of autism questionnaire, a 14-item self-efficacy scale targeting GPs’ perceived confidence in identifying and managing their autistic patients, and an open question eliciting participants’ experiences of working with autistic people.
Results In total, 39.5% (n = 120) of GP participants reported never having received formal training in autism. Despite demonstrating good knowledge of its key features, participants reported limited confidence in their abilities to identify and manage autistic patients, with many citing a number of barriers that overwhelmingly focused on perceived failings of the current healthcare system (such as a lack of clarity around referral pathways).
Conclusion There is an urgent need for improved local specialist service provision alongside clearer referral pathways for diagnosis to improve both GPs’ confidence in caring for their autistic patients and the healthcare experiences of autistic patients and their families. Local clinical commissioning groups are best served to assist GPs in ensuring that they can reliably detect the condition and make appropriate provisions for support.
INTRODUCTION
In the UK, GPs are often the first professionals consulted by parents or individuals seeking assistance for a suspected diagnosis of autism spectrum disorder (hereafter, referred to as ‘autism’).1 Responding to autism is a potentially challenging task for GPs: changing definitions of autism,2 the substantial heterogeneity both between and within individuals,3 and the prevalence of co-occurring conditions in many children and adults on the autism spectrum4 all present serious difficulties for non-specialist clinicians. The situation is further complicated by the fact that help is not necessarily sought for suspected autism per se: parents often seek help for their child’s behavioural issues1 and many adults’ initial concerns are about their own mental health — for example, anxiety or depression.5 Parents of children on the autism spectrum often report dissatisfaction with their healthcare experiences,1,5,6,7 especially regarding the diagnostic process.
Beyond these autism-specific challenges, GPs are experiencing increased pressure in the wake of recent, radical changes to the primary healthcare system,8 including burgeoning caseloads and an increasingly important role for GPs in the commissioning of services. Particular frustration relates to lengthy delays, which can postpone access to services and limit confidence in their clinicians’ ability to help during, or after, diagnosis.1,9–11 This, in turn, has led to calls for increased training in autism for GPs and other frontline professionals.12 The few existing studies — all conducted outside of the UK — have shown that GPs’ awareness of autism, as well as appropriate referral and care pathways, is variable.13–16
The only study to have investigated the perceived self-competence of primary care physicians in the US found that this linked to the extent of their experience of autism (both in having a greater number of autistic patients and having a friend or relative on the autistic spectrum) and whether they had received previous autism training.17
To understand these issues within a UK context, the authors conducted a survey examining GPs’ perceived self-efficacy in identifying and managing their autistic patients and the factors that affect it.
A note on terminology: identity-first language (that is: autistic person), opposed to person-first language (that is: person with autism), is preferred by many autistic people and their allies. Therefore, in this article, the authors use predominantly identity-first language.18
How this fits in
There is currently significant interest in autism and one central question concerns how, and when, autistic people are diagnosed and access services. GPs are crucial to that process but nothing is known about the perceptions of GPs in the UK of working with this patient group. This study examined GPs’ perceived self-efficacy in identifying and managing their autistic patients and the factors affecting this. GPs reported having limited confidence, which was due, in part, to limited access to autism training and confusion around diagnostic and care pathways.
METHOD
Online survey
GPs were invited to take part in an online survey (powered by SurveyMonkey®) between September and December 2015. Participants were recruited through:
convenience sampling methods;
purposively targeting members of the Royal College of General Practitioners (RCGP) and;
internet snowballing methods through social media, for example, contacting relevant organisations and groups via Twitter.
The survey contained three sections and took approximately 10–15 minutes to complete. Part 1 comprised 19 items on the participants’ background, including basic demographics (age; sex; ethnicity; location of, and years in, current practice; patient hours/week) and information regarding training and experience, both as a GP and in autism specifically.
Part 2 included a knowledge of autism scale, adapted from Stone19 but modified to reflect up-to-date scientific understanding of autism. Twenty-two statements assessed each participant’s knowledge of the early signs of autism, descriptive characteristics, and co-occurring behaviours. Following Campbell et al,20 responders rated these statements as ‘true’ or ‘false’. Scores on each item were summed to yield a total score; the higher the score, the greater the knowledge about autism.
Similar to previous studies on the knowledge of autism,12,20 the scale showed moderate internal consistency (Cronbach’s α = 0.54); this may be due to the diverse nature of the items, which, despite focusing on autism, vary from socioemotional and cognitive characteristics to more descriptive (diagnosis, prognosis, and intervention) features.
Part 3 was a self-efficacy scale. Perceived self-efficacy is a psychological construct concerned with people’s beliefs in their capabilities to achieve a goal, which differs according to context and the behaviour of interest.21,22 The scale used in the present study was based on previous scales, but was adapted to specifically target GPs’ perceived confidence in their decision making regarding working with their patients who were, or who suspected they were, on the autism spectrum. Following Bandura’s procedure,21 a 14-item scale was generated, with scores ranging from 1 (‘not at all confident’) to 10 (‘extremely confident’). Scores from each item were averaged to yield a mean self-efficacy score; higher scores reflected greater self-efficacy. The scale showed excellent internal consistency (Cronbach’s α = 0.95). The survey ended with one final open question to elicit each participant’s views and experiences of working with autistic people and their families. All data were collected anonymously. All participants provided informed consent to participate in this study.
Data analysis
Responses are presented descriptively, alongside:
correlational analyses — to assess the relationships between knowledge of autism, perceived self-efficacy, training, and other key variables; and
regression analyses — to examine potential predictors of GPs’ perceived self-efficacy.
As a result of the relatively large number of comparisons, a P-value of 0.01 was set. Participants’ qualitative responses were analysed using thematic analysis, as detailed by Braun and Clarke.23 An inductive approach was adopted, providing descriptive overviews of the key features of the semantic content of data within an essentialist framework. Two authors independently familiarised themselves with the qualitative survey responses, and met to discuss preliminary themes and make a list of provisional codes. These codes were then independently applied to each qualitative response. The authors reviewed the results on several occasions, resolving any discrepancies that occurred, and agreed on the final themes and subthemes.
RESULTS
In total, 462 people responded to the survey. Responses were not considered for participants who:
did not consent to participate (n = 4);
were not UK residents (n = 31); or
did not progress past Part 1 (n = 123) of the survey.
Table 1 shows background information on the final 304 participants. Most responders were female (72.4%, n = 220), of white ethnicity (79.6%, n = 242), and had obtained their primary qualification in the UK (91.1%, n = 277). The majority of GPs’ current practices were distributed across England, in which participants had spent, on average, 11 years practising as a GP.
Participant characteristics, n = 304
Quantitative analysis
Current practice, training, and personal experience
Of the 304 GP responders, 91.4% (n = 278) reported having at least one autistic patient currently in their care. Of these responders, 48.2% (n = 134) had <10 autistic patients, 41.7% (n = 116) had 11–30, and 10.1% (n = 28) had >30. In the previous year, 91.1% (n = 277) had been approached by at least one patient about suspected autism, with the majority (78.0%, n = 237) being approached by up to five people. Most responders felt that this number had increased since they began their professional career (65.8%, n = 200).
Few responders (28.0%, n = 85) reported referring to the diagnostic criteria for autism1,24 and even fewer (19.1%, n = 58) reported using any screening instruments, such as M-CHAT,25 the Social Communication Questionnaire,26 or the Autism Spectrum Quotient.27 GPs reported referring their patients with suspected autism to child and adolescent mental health services (CAMHS, 61.5%, n = 187), community paediatricians (59.2%, n = 180), community learning disability teams (22.0%, n = 67), and/or adult autism services (42.8%, n = 130).
Almost two-thirds (63.5%, n = 193) of responders reported not having received any training on autism during their primary medical degree or specialist GP training. Furthermore, a similar number (65.8%, n = 200) reported not having received specific training (for example, via continuing professional development) on autism since obtaining their qualifications. All in all, 39.5% (n = 120) of participants reported never having received any training about autism — an additional 2.0%, (n = 6) could not remember.
Of those who had received training (58.6%, n = 178), 42.7% (n = 76) reported having received it during their primary medical degree or specialist GP qualification, 41.0% (n = 73) received specific training in the time since obtaining their primary qualification, and 16.2% (n = 29) received training during both. Encouragingly, those who completed their qualifications more recently were more likely to have received training on autism during their degree (r [297] = −0.31, P<0.001). In total, 62.6% (n = 99) felt that this training was ‘somewhat’ or ‘very’ useful while the remainder (37.3%, n = 79) felt that it was not very, or not at all, useful. Almost half of responders (47.7%, n = 145) reported having some personal experience of autism, either through being autistic themselves (n = 3), or having a child (n = 52), other relative (n = 44), or colleague/friend (n = 37) on the autism spectrum.
Knowledge of autism scale
Table 2 outlines the items on the knowledge of autism scale and the number (and percentage) of GPs that correctly answered each one. Responders generally scored highly on the knowledge of autism scale (M [mean] = 88.1%, correct standard deviation [SD] = 9.2, range = 36.4–100%). A knowledge score was calculated, adjusting for chance responding using the following equation, in which R is the number of right responses, W is the number of wrong responses, and n is the number of items:28

GPs’ correct responses to items on the knowledge of autism scale, n = 304
Responders’ scaled knowledge scores were expressed as a percentage of the total number of questions asked (M = 89.4%, SD = 15.6, range = 0–100%). Although GP responders’ scores approached ceiling (when there is a preponderance of scores at the top end of a scale), it is noteworthy that the scale was sufficiently sensitive to detect differences between this sample of GPs and a sample of trainee primary and secondary school teachers (n = 243), who scored significantly lower (M = 79.2%, SD = 20.0) than the GP responders in this study, t (545) = 6.69, P<0.001, d = 0.57 (Pellicano, Crane, Kenny, and Remington, unpublished).
GPs’ scaled knowledge scores were not significantly associated with:
their age (r [303] = 0.09, P = 0.14);
their time in practice as a GP (r [303] = 0.11, P = 0.06);
the number of autistic patients currently under their care (r [303] = 0.09, P = 0.11); or
their training on autism, (r [303] = −0.01, P = 0.88).
Higher knowledge scores, however, were significantly correlated with a greater personal connection to autism (r [303] = 0.19, P = 0.001).
Self-efficacy scale
Despite their impressive knowledge, overall, participants were only somewhat confident about their ability to make correct or appropriate clinical decisions about the identification and management of their autistic patients (M = 4.8, SD = 1.5, range = 1.50–9.07). The statements were given mode scores of 2–5, suggesting low-to-moderate perceived self-efficacy (Table 3). GPs were least confident in deciding which medications to prescribe for their autistic patients (arguably because there are few tried-and-tested pharmacological ‘treatments’) and most confident about identifying stress in the parents/carers of their autistic patients (Table 3). Higher self-efficacy scores were significantly related to more training on autism (r [297] = 0.18, P = 0.002) and greater personal experience of autism (r [303] = 0.31, P<0.001). Years spent practising as a GP (r [303] = 0.12, P = 0.04), number of autistic individuals under their care (r [303] = 0.13, P = 0.03), and knowledge of autism (r [303] = 0.13, P = 0.02) were also correlated with GPs’ self-efficacy scores, although these correlations did not reach significance at the P = 0.01 level.
Mean and mode scores for each item on the self-efficacy scale
Predicting GPs’ self-efficacy
A multiple regression analysis was undertaken on GPs’ perceived self-efficacy with the following variables entered stepwise into the model, together with knowledge scores:
years spent practising as a GP;
the number of patients on the autism spectrum currently under their care;
their training on autism; and
their personal experience of autism.
Responders’ personal connections to autism made a significant contribution (F [1, 296] = 31.76, P<0.001, R2 = 0.10). Autism training also explained unique variance (F [1, 295] = 11.46, P<0.001, R2 change = 0.03) (Table 4). There were no other significant predictors (all P-values >0.09), final model: F (2, 295) = 22.17, P<0.001, R2 = 0.13.
Summary of hierarchical regression analysis predicting GPs’ self-efficacy scores (final model)
Qualitative analysis
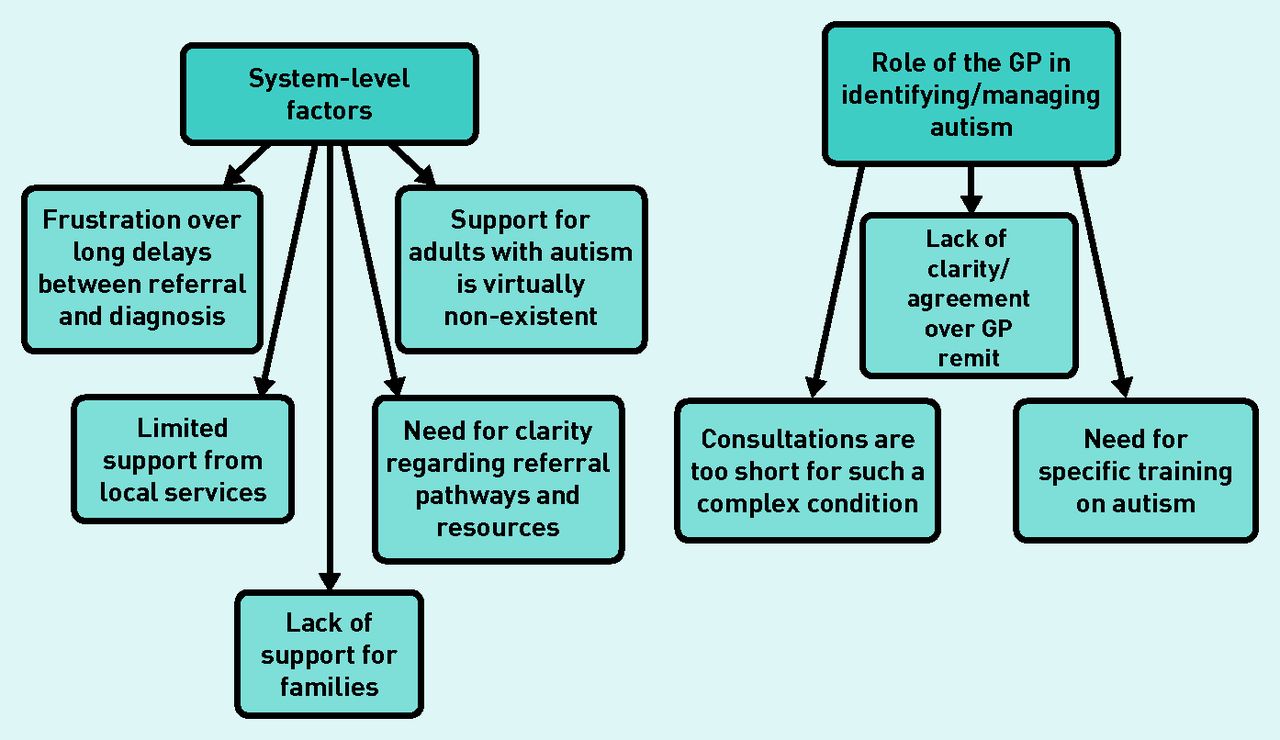
In total, 186 GPs (61.2%) responded to the open question (to elicit each participant’s views and experiences of working with autistic people and their families). The quotes included in the following section represent those from a range of participants. Two main themes were identified:
system-level factors; and
role of the GP in identifying/managing autism (Figure 1).
{kind=link}
GPs’ views and experiences on working with their autistic patients: themes and subthemes.
System-level factors
Participants reported frustration over long delays between referral and diagnosis, largely attributed to a lack of clear referral pathways, long waiting lists, and limited resources. For one responder these delays were ‘completely unacceptable, particularly for adults’.
Others noted the lack of joined-up services, leading to ‘a lot of passing from pillar to post of patients and their families’, with many left unsupported, ‘adding significantly to their distress’.
Responders also reported limited support from local services post-diagnosis. Once diagnosed, one GP commented on having a ‘sense of hopelessness about lack of appropriate help’, with ‘no offer of support, therapy, or follow-up’.
Several commented on the pervasiveness of autism, calling it ‘a lifelong problem that requires lifelong support, which is rarely available’.
Responders stressed that support for autistic adults was virtually non-existent. They highlighted several challenges, including the complexity of diagnosing adults, as opposed to children (particularly in light of co-occurring mental health conditions), and difficulties ‘finding a place for them to be diagnosed’; some reported ‘no specific local service for diagnosis and management for adults with suspected autism’ who are ‘often left to fend for themselves’.
They also underscored problems with patients transitioning from child to adult support services. GPs also highlighted the lack of support for families. They recognised the often profound impact on families, including parents and siblings, emphasising that the strains ‘can be much greater than anticipated or readily recognised’.
Many responders felt the need for clarity regarding referral pathways and resources as these were ‘confusing’ and ‘not at all clear’, leading to a lack of confidence ‘as to what is out there and who/where to refer’. Overall, responders felt that ‘resources for supporting GPs are poor’. One GP remarked on how ‘the relatively few services for children and adults [on the autism spectrum] are in a constant state of flux and impossible to keep up with’.
Organisations working in silos was cited as a key problem. One responder summed up the situation: ‘Diagnostic pathways for children are complex locally, with the hospital paediatricians now rejecting referrals completely. The community paediatricians will not see someone for assessment if they are under CAMHS and vice versa; the community paediatricians will also reject referrals that are not sent with a multidisciplinary referral form, which requests information we do not have access to (for example, school, nursery information). Support for families going through this process is lacking, with delays, buck passing, and frustration all round.’
Role of the GP in identifying and managing autism
Responders described how consultations are too short for such a complex condition. Assessing and managing autism ‘takes more than a 10-minute consultation’ and ‘even with appropriate training, GPs do not have the resources properly to diagnose or look after patients/carers with autism’.
Responders were divided about the remit of the GP. Some felt that undertaking assessments and managing care is ‘well beyond the scope of what a GP can provide in the face of the deepening workload crisis and falling number of GPs’ and that they should not ‘be taking the role of the specialist’. Others, however, felt ‘that our role as GPs is to be aware of local services so that parents/carers/those with autism know where to turn for support’.
However, many also noted that ‘it is very difficult to access resources’ for their autistic patients especially for ‘signposting to community resources’ and that it would be ‘helpful to have more information to assist patients and their families’.
Regardless of these disagreements, responders identified the need for specific training on autism including that ‘in child development and communicating with patients’ because GPs are often ‘the first port of call for these patients’.
Some responders were aware of the special considerations required when engaging with autistic patients concerning sensory sensitivity and co-existing anxiety.
DISCUSSION
Summary
Despite demonstrating robust knowledge about autism, GPs reported modest confidence in identifying and managing individuals with a diagnosis or suspected diagnosis of autism. This confidence was related to greater experience with autism, including personal connections and, to a lesser extent, prior training in autism. Qualitative analysis identified additional factors at the systemic level, which may have affected GPs’ confidence in working with these patients, including lack of services, lengthy delays between referral and diagnosis, and, especially, a lack of clarity surrounding referral and care pathways. These largely negative views are in spite of the Autism Act 2009, recent public policy,29 and service development initiatives30–32 designed to improve service provision for autistic people and their families.
Given that the Department of Health’s autism strategy has not been consistently implemented across regions and services29,32–33 the results presented here suggest there is an urgent need for improved local specialist service provision alongside clearer referral pathways for diagnosis.
Strengths and limitations
This is the first study, to the authors’ knowledge, to use a reasonably large sample to examine UK GPs’ perspectives on working with their patients on the autism spectrum. Although the sample size exceeded that of other, similar studies from outside the UK,13–16 the total sample of 304 GPs was relatively low. Survey responses from general physicians are typically low;34 this could be enhanced in future with surveys mailed to postal and e-mail addresses, with monetary incentives included.
Almost half of responders reported having some personal connection with autism. This number is not surprising given current prevalence estimates (1% of the population),35,36 but may reflect a response bias, with those with a keen interest in autism more likely to respond. If this is the case, GPs’ knowledge and awareness of autism may well be underestimated: in this sample, personal connection to autism was significantly related to participants’ knowledge of autism. It is, therefore, possible that non-responding GPs, who may have more limited personal connections to autism, also have lesser understanding of the condition, including how to identify and manage it.
Comparison with existing literature
In contrast with previous studies conducted outside of the UK,13–16,20 GPs’ basic knowledge of the key autism characteristics was high in this sample.1,5,6 Continual autism training is needed, however, especially given the heterogeneity of presentation and the high rates of co-occurring conditions. Strikingly, more than a third (39.5%) of GPs reported never having received professional training on autism — either during their degree or after qualifying. Given the significant challenges these responders reported, it is unsurprising that they expressed a desire for more autism training.
Currently, GPs appear to rely on their personal connections with autism (through family members, friends, colleagues) as a source of tacit knowledge, which may provide a more visceral and more nuanced appreciation of the realities of autism.13,17 An overreliance on subjective, personal knowledge could, however, afford a narrow, idiosyncratic view of what autism is, potentially causing clinicians to miss the signs in some individuals and potentially lead to disparities in healthcare provision.37 Improvements in disseminating objective knowledge through increased training opportunities — especially focused on underserved populations (for example, autistic girls or women) — should help to mitigate these concerns.
Implications for research and practice
GPs’ confidence in their knowledge of autism may well play a role in their decisions to refer — or to not refer — children or adults for further diagnostic assessment for the condition;38 so efforts to enhance perceived self-efficacy are much needed. The findings presented here suggest that initiatives targeted towards training in autism and greater clarity around referral pathways should go some way to improving GPs’ confidence in working with their autistic patients.
Encouragingly, better understanding of autism among healthcare professionals has been highlighted as a key priority in the UK.12,28 As such, the RCGP has produced educational resources on autism spectrum disorder designed to improve awareness of autism among GPs.30
The authors recommend that local clinical commissioning groups (CCGs) also play a role in enabling GPs effectively to both share best practice and establish robust pathways to care. CCGs and GPs must work together with autistic people and their families to ensure that the care that is commissioned is respectful, accessible, and, as put forth by Nicolaidis et al, person centred.6
Acknowledgments
The authors would like to thank Lauren Harding and Verity Sharp from the RCGP for promoting the survey among its members, Katy Warren and Hannah White for help with recruitment, and Mel Bovis and Marc Stears for helpful discussion. They are also extremely grateful to all those who took part in the questionnaire.
Notes
Funding
No specific funding was provided for this study, although research at the Centre for Research in Autism and Education is supported by the Clothworkers’ Foundation and Pears Foundation. The conclusions and views expressed in this article are those of the authors and not necessarily those of the funders.
Ethical approval
Ethical approval was granted by the Research Ethics Committee at University College London Institute of Education, UCL (REC 708).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received August 8, 2016.
- Revision requested September 9, 2016.
- Accepted October 10, 2016.
- © British Journal of General Practice 2017
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

