


INTRODUCTION
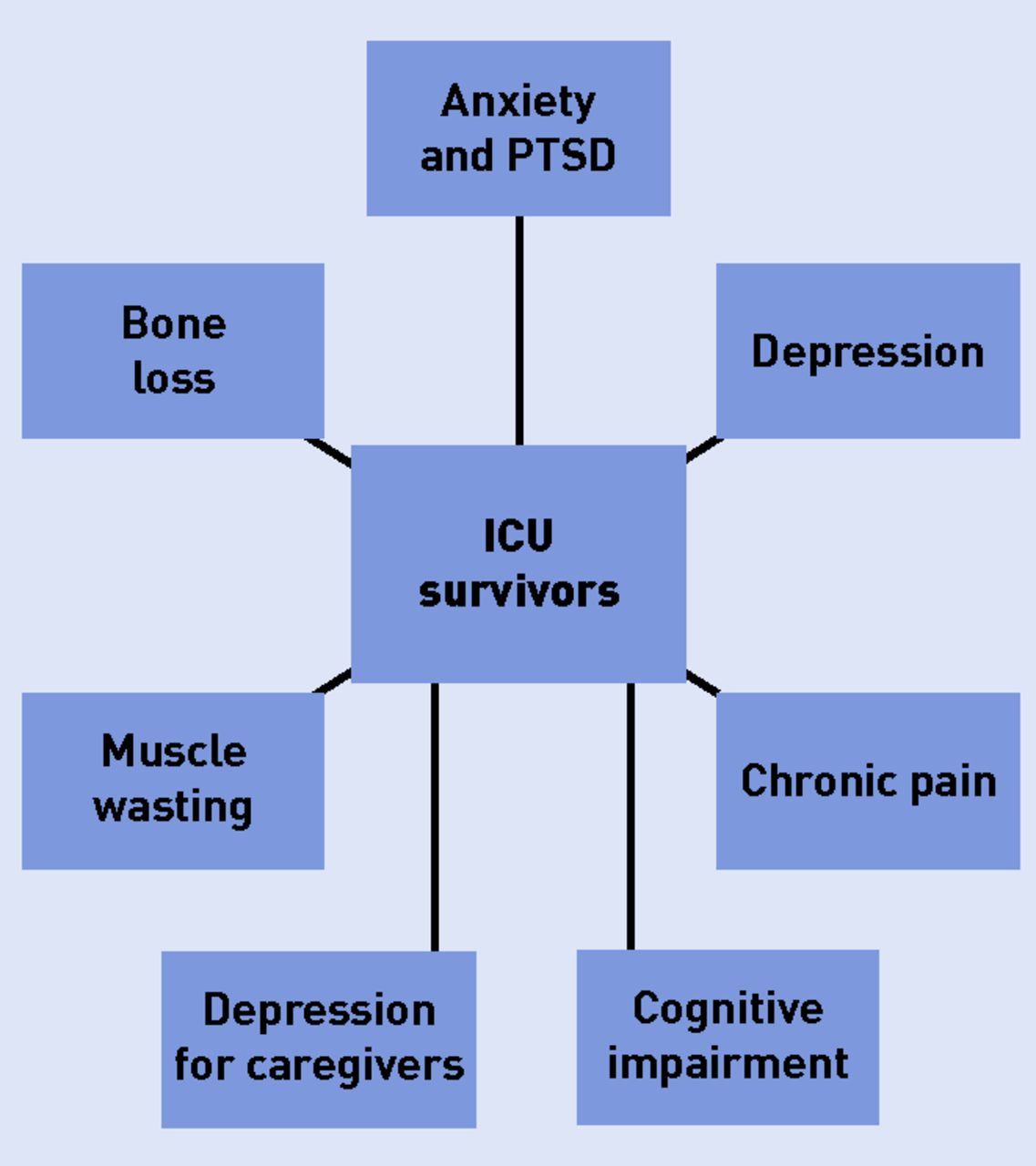
Specialists in intensive care medicine have long focused on the prevention of short-term mortality. As intensive care unit (ICU) mortality continues to improve, interest in outcome measures has expanded to include the morbidity and mortality of survivors. Over the last 10 years it has been increasingly recognised that critical illness is a medical condition itself, irrespective of the underlying cause for ICU admission, and patients experience physical, psychological, and cognitive dysfunction after hospital discharge (Figure 1). However, because relatively few patients ultimately require critical care, many GPs may have little contact with these patients. It may therefore be difficult to provide the additional support required by ICU survivors. This short paper highlights some of the physical and psychological difficulties that patients face after discharge from ICUs, and will hopefully help GPs to plan long-term management of their patients in the community.
{kind=link}
Post-intensive care syndrome signs and symptoms. ICU = intensive care unit. PTSD = post-traumatic stress disorder.
PTSD AND ANXIETY
Twenty-five per cent of patients who survive ICU report symptoms consistent with post-traumatic stress disorder (PTSD), with patients who have a previous history of anxiety or depression being at highest risk of developing PTSD. Critical illness results in PTSD in 22% of cases1 for a variety of reasons — patients suffer life-threatening illness, the treatments provided are often invasive, many medications used have neurological and psychological effects (in particular benzodiazepines, corticosteroids, inotropes, and vasopressors), and almost all patients will experience sleep deprivation, thirst, pain, and delirium with hallucinations and delusions.
Anxiety disorders are present in as many as 25% of patients 2 years after discharge. Both anxiety and PTSD are related due to an inability to recall facts about their ICU stay, and this difficulty with factual recall can last for 18–24 months.
Patients with anxiety and PTSD require referral to psychiatric services. Psychotherapy often focuses on the recall of factual memories, therefore patient diaries are known to be an effective means of decreasing PTSD after discharge. These patient diaries are kept by family members during the ICU stay and should be discussed with a member of the ICU team after the patient’s discharge.
DEPRESSION
The prevalence of depression after ICU is reported to be between 4 and 64%.2 In contrast with studies on PTSD, medication use, length of stay, and severity of illness do not seem to be associated with depression post-discharge. However, patients with a pre-existing history of psychological morbidity are at a higher risk. ICU diaries have less of an effect on depression than on PTSD; however, outpatient physical rehabilitation is suggested as a method of treating and preventing depressive symptoms.
CHRONIC PAIN
Exposure to pain and stress may persist after ICU discharge, leaving patients in chronic pain. Whether or not the incidence and degree of chronic pain in ICU survivors differs from the rest of the population remains unclear. Different rates of pain are reported among sepsis survivors, depending on the country studied.3 However, those who survive acute respiratory distress syndrome (ARDS) are known to have higher rates of chronic pain than the general population. In addition, the high-dose opioids used while patients are intubated and ventilated may result in tolerance and addiction.
MUSCLE WASTING
Neuromuscular weakness is a major complication of intensive care treatment, which affects around 46% of patients with sepsis in multi-organ failure who require mechanical ventilation.4 Weakness may be due to either critical illness polyneuropathy or myopathy, and may be due to microcirculatory damage causing impaired peripheral nerve and muscle perfusion, or commonly used medications including high-dose corticosteroids and neuromuscular blockers.5 In addition, diaphragmatic inactivity during mechanical ventilation can occur 18 hours after mechanical ventilation is started, from atrophy of diaphragmatic muscle fibres. This muscle weakness lasts long after discharge from hospital, and is dependent on ICU length of stay. Each day spent on bed rest in the ICU results in a decrease in muscle strength, which may last for years. Survivors of ARDS are particularly at risk, and may experience functional impairment at 5 years after discharge. Community-based graded exercise programmes can be beneficial in returning patients to their pre-critical care abilities.
BONE DISEASE
Bone hyperresorption and vitamin D deficiency is a common problem in intensive care, with multiple causes including prolonged immobilisation, hormonal changes, the side effects of steroids, a lack of daylight, and circulating inflammatory cytokines. Although this resorption appears to normalise after discharge from the ICU, many patients are left with osteoporosis. The 10-year fracture risk in ICU patients is significantly higher than in the rest of the population.6 Routine use of bisphosphonates is not indicated in the unit because of their cardiac side effects, therefore these high-risk patients should be screened for osteoporosis before hospital discharge, and treated if appropriate.
TRACHEOSTOMY
Around 20–30% of patients in an ICU will require a tracheostomy in order to be weaned off mechanical ventilation. These tracheostomies will usually be removed long before hospital discharge, although patients can continue to experience long-term complications. These include scar formation, discomfort at the site of insertion, and tracheal stenosis. Although percutaneous tracheostomies have a lower incidence of complications than surgical tracheostomies, analysis of patients’ subjective evaluation has found that levels of dissatisfaction remain, particularly in cosmetic terms.7 If there is clinical suspicion of stenosis the patient should be referred to an outpatient ENT clinic, where lung function tests should be performed to diagnose a fixed airway obstruction. If an obstruction is present they will likely require a nasendoscopy, bronchoscopy, CT, and/or MRI.
COGNITIVE IMPAIRMENT
Twenty-five per cent of ICU survivors have a degree of cognitive impairment at 12 months, which is similar to mild Alzheimer’s disease.8 These cognitive deficits are usually new, and related to the critical care admission rather than the patient’s pre-existing medical comorbidities. Both global cognitive impairment and executive function tend to be impaired. An increased duration of delirium during the ICU admission is a major risk factor, as is hypoxia, hypotension, sedation, and hyperglycaemia. Prevention of cognitive dysfunction should therefore begin with treatment delivered in the ICU, but cognitive rehabilitation can improve executive function in ICU survivors.
CAREGIVER STRESS
Although patients who are discharged home with informal caregiving appear to benefit, this has an impact on the quality of life of their caregivers. In general, more depressive symptoms and lower quality of life scores are seen for younger caregivers, those with less personal growth, and less social support, whereas the severity of illness of the patient does not appear to have an effect in the longer term. Furthermore, caregivers of ICU survivors have a poorer quality of life score than caregivers of patients with Alzheimer’s disease.9 These caregivers may benefit from family-based models of care, along with cognitive behavioural therapy and increased social support.
CONCLUSION
Increasing numbers of patients will survive an ICU, and will require the assistance of post-critical care services. However, many of their psychological and physical complaints may arise after discharge and their first point of contact will probably be with their primary care physician. Recognition of the fact that these complaints are related to their period of critical illness should help in ensuring that GPs can access specialist services for their care.
Notes
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The author has declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received November 8, 2016.
- Revision requested November 14, 2016.
- Accepted January 2, 2017.
- © British Journal of General Practice 2017
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

