


INTRODUCTION
Although essential hypertension (HTN) is the most common type of HTN, nearly 10% of patients have a secondary cause. Primary hyperaldosteronism (PHA) accounts for up to 23% of secondary HTN depending on criteria, screening methods, and the population studied.1 Aldosterone-producing adenomas, known as Conn’s syndrome, represent nearly 30% of PHA cases.
Symptoms of PHA are nonspecific and may be easily missed, leading instead to the diagnosis of essential HTN. Two patients with a long history of HTN, hypokalaemia, and vague symptoms were followed by multiple specialties (internal medicine, cardiology, and endocrinology), but had not been diagnosed with Conn’s syndrome. Two cases are presented here as a means to raise awareness of this condition (Conn’s syndrome) among primary care practitioners (PCPs), because it is a potentially curable cause of HTN.
CASE REPORT 1
A 46-year-old white female with a 6-year history of presumed essential HTN presented to her PCP with fatigue, myalgias, migraines, generalised anxiety, decreased libido, paresthesias, polydipsia, polyuria, trace peripheral oedema, heart palpitations, and shortness of breath over the previous 2 years, as well as a 1-month unexplained weight gain (3 kg). Fluctuating serum potassium levels (with the lowest of 2.1 mEq/L) were reported. Antihypertensive medications (nifedipine and hydrochlorothiazide) were deemed the cause of hypokalaemia. Oral potassium supplements and spironolactone were prescribed.
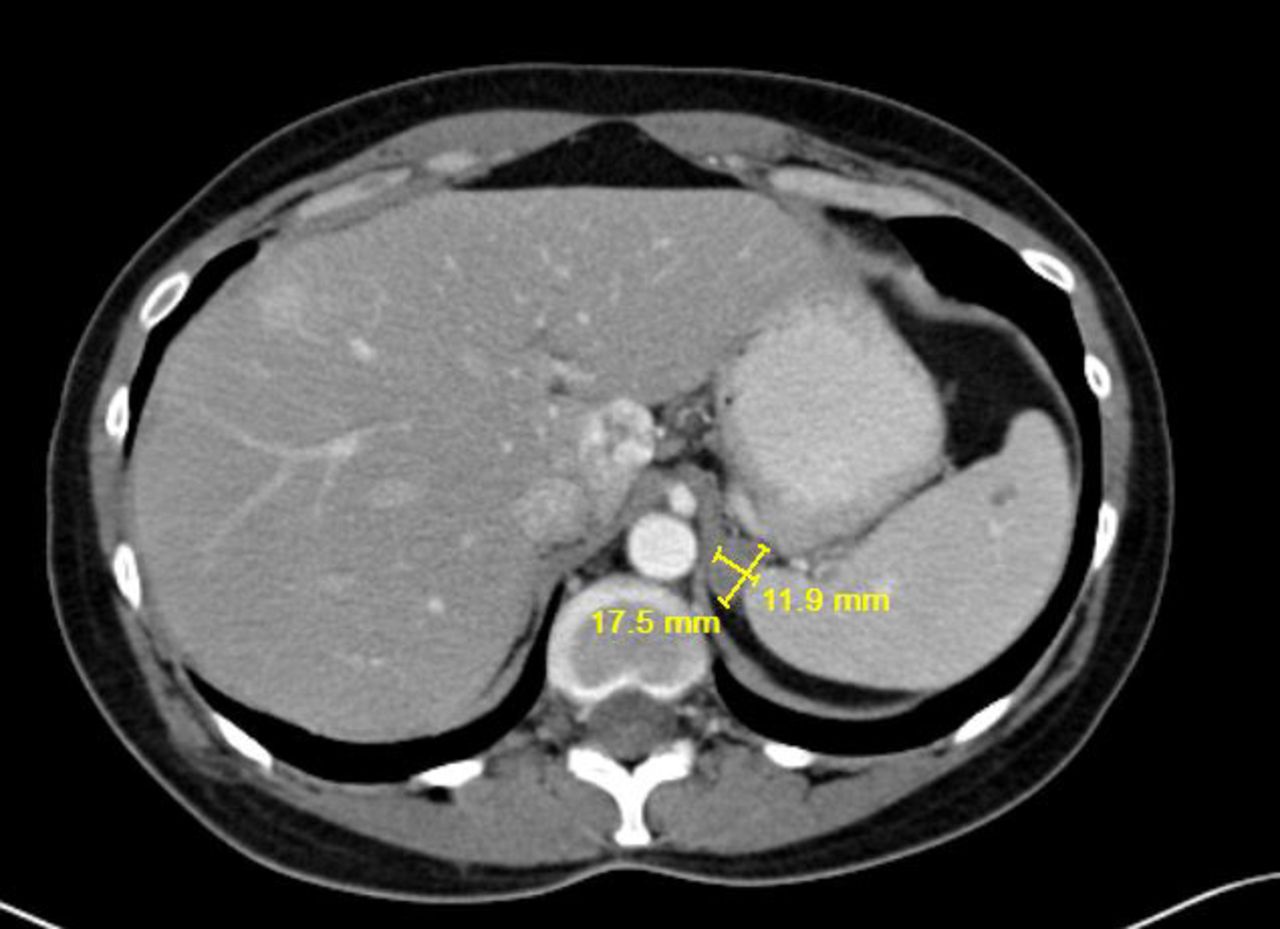
A chest CT scan was unremarkable, but, incidentally, a 1.8 × 1.2 cm mass on the left adrenal gland was found (Figure 1). Endocrinology initially considered PHA. However, due to normal serum aldosterone levels (12 ng/dL) and normal aldosterone-to-renin ratio (after withholding spironolactone for 3 weeks), this diagnosis was dismissed. Thyroid hormones, metanephrines, and cortisol levels were within normal limits, which ruled out the diagnoses of thyroid disease, phaeochromocytoma, and Cushing’s syndrome.

CT of the upper abdomen shows 1.8 × 1.2 cm left adrenal adenoma.
Surgical oncology was consulted for evaluation of the adrenal mass. Physical exam was normal with the exception of blood pressure (BP) of 149/94 mmHg. Serum potassium was 2.6 mEq/L despite oral supplementation. Adrenal venous sampling showed markedly increased aldosterone levels on the left, confirming the diagnosis of aldosterone-producing adenoma.
Laparoscopic resection of the left adrenal gland was performed. HTN resolved immediately after surgery, allowing discontinuation of antihypertensive medications. The patient reported improvement of her symptoms. Adrenal adenoma with hyperplasia of the zona glomerulosa was pathologically confirmed.
The patient was asymptomatic at follow-up and potassium supplementation was discontinued. The patient remains normotensive and asymptomatic 7 years after surgery.
CASE REPORT 2
A 40-year-old black female with a history of presumed essential HTN (diagnosed at age 19) and hypokalaemia presented for surgical evaluation of a multinodular goitre. She reported a 3-month unintentional 12 kg weight gain, along with constant fatigue, headaches, labile affect, anxiety, episodes of unexplained crying, and palpitations. She had been monitored by a PCP and cardiologist for several years and had multiple episodes of hypertensive crisis. Prescribed medications included amlodipine, hydroclorothiazide, irbesartan, spironolactone, potassium chloride, phentermine, alprazolam, and zolpidem.
On examination, the patient was anxious and BP was 144/82 mmHg. Serum potassium was 2.8 mEq/L, despite supplementation. Serum aldosterone was 79 ng/dL, more than twice the normal level. An abdominal MRI showed a 2.2 × 2.1 cm right adrenal adenoma (Figure 2). Thyroid function, metanephrines, and cortisol levels were normal and cytological studies revealed benign thyroid disease.

{kind=link}
{kind=link}
MRI of the abdomen shows 2.2 × 2.1 cm right adrenal adenoma.
Laparoscopic right adrenalectomy was performed and BP returned to normal range shortly after surgery, without the need for antihypertensive medications. The patient was discharged on oral potassium supplementation, which was ultimately discontinued 1 month later. On follow-up, potassium levels were within normal limits and she reported resolution of all her original symptoms.
DISCUSSION
PHA is one of the leading causes of secondary HTN and should be considered when evaluating the hypertensive patient, especially if young. PHA represents a significant cause of HTN in the general population. Studies evaluating pre-hypertensive patients in the primary care setting have reported a PHA prevalence of 5–7%.2,3 Among the population with resistant hypertension, however, the PHA prevalence can be up to 23%.1 The importance of diagnosing and treating PHA is highlighted by the fact that patients with PHA have a higher risk for cardiovascular disease than patients with essential HTN.4 These worse cardiovascular outcomes are caused by aldosterone excess, which produces direct myocardial injury, endothelial dysfunction, and vascular remodelling.
Diagnosis of PHA may be challenging due to nonspecific symptoms, such as muscle weakness, palpitations, and emotional changes. It is known that patients with HTN and hypokalaemia are at increased risk of having underlying PHA.However, many patients with PHA present with normal serum potassium and may have normal aldosterone levels, which may be misleading.5 Moreover, patients with behavioural alterations, including generalised anxiety, are often misdiagnosed as having essential HTN with an underlying psychiatric disorder. It is important for PCPs to suspect Conn’s syndrome in these contexts.
International guidelines, as well as the NICE guidance, recommend PHA screening in patients with HTN and hypokalaemia, treatment-resistant HTN, severe HTN, or onset of HTN at a young age.1,6 Diagnosis is established by biochemical tests (that is, aldosterone-to-renin ratio, sodium suppression test, adrenal venous sampling) and imaging tests (abdominal CT scan or MRI). Diuretics (including spironolactone) should be discontinued at least 4 weeks before testing to avoid a false-negative aldosterone-to-renin ratio, which was possibly seen in our first patient.
Other differential diagnoses of secondary HTN include renal artery stenosis, thyroid disease, Cushing’s syndrome, obstructive sleep apnoea, and phaeochromocytoma.1 Associated weight gain should raise the suspicion of PHA, hypothyroidism, Cushing’s syndrome, and obstructive sleep apnoea.1 Both of our patients had significant weight gain, but cortisol and thyroid hormones were within normal limits. Obesity itself has also been linked with hyperaldosteronism and HTN.7
Surgery is the treatment of choice in unilateral adrenal hyperplasia or adrenal adenoma. Laparoscopic adrenalectomy is a safe procedure, producing long-term normotension without antihypertensive medications in most patients,8 while also reducing the risk for cardiovascular disease, depression, and anxiety.9 It is important to acknowledge, however, that some patients with PHA may have underlying essential HTN; consequently, HTN does not resolve after surgery in these cases.1
CONCLUSIONS
The diagnosis of Conn’s syndrome requires a high level of suspicion. Once diagnosed, it has a straightforward treatment, usually with excellent long-term outcomes. Misdiagnosis can have severe consequences, including complications associated with resistant HTN, hypokalaemia, myocardial damage, and vascular dysfunction. Other consequences include stress from labile emotional states, side effects due to polypharmacy, and unnecessary expenses associated with multiple medications, tests, and consultations.
Notes
Patient consent
Patient consent has been obtained for the publication of this article and associated images.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received March 27, 2017.
- Revision requested April 28, 2017.
- Accepted May 29, 2017.
- © British Journal of General Practice 2017
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

