


Abstract
Background Statin prescribing should be based on cardiovascular disease (CVD) risk, but evidence suggests overtreatment of low-risk groups and undertreatment of high-risk groups.
Aim To investigate the relationship between CVD risk scoring in primary care and initiation of statins for the primary prevention of CVD, and the effect of changes to the National Institute for Health and Care Excellence (NICE) guidance in 2014.
Design and setting Historical cohort study using UK electronic primary care records.
Method A cohort was created of statin-naïve patients without CVD between 1 January 2000 and 31 December 2015. CVD risk scores (calculated using QRISK2 available from 2012) and statin initiations were identified. Rates of CVD risk score recording were calculated and relationships between CVD risk category (low-, intermediate-, and high-risk: <10%, 10–19.9%, and ≥20% 10-year CVD risk) and statin initiation were analysed.
Results A total of 1.4 million patients were identified from 248 practices. Of these, 151 788 had a recorded CVD risk score since 2012 (10.67%) and 217 860 were initiated on a statin (15.31%). Among patients initiated on a statin after 2012, 27.1% had a documented QRISK2 score: 2.7% of low-risk, 13.8% of intermediate-risk, and 35.0% of high-risk patients were initiated on statins. Statin initiation rates halved from a peak in 2006. After the 2014 NICE guidelines, statin initiation rates declined in high-risk patients but increased in intermediate-risk patients.
Conclusion Most patients initiated on statins had no QRISK2 score recorded. Most patients at high risk of CVD were not initiated on statins. One in six statin initiations were to low-risk patients indicating significant overtreatment. Initiations of statins in intermediate-risk patients rose after NICE guidelines were updated in 2014.
- clinical guidance
- general practice
- hydroxymethylglutaryl-CoA reductase inhibitors
- primary prevention
- risk assessment
- statins
INTRODUCTION
Statins for primary prevention of cardiovascular disease (CVD) have been shown to be effective in reducing all-cause mortality, coronary heart disease events, and strokes.1 CVD risk (determined from a combination of age, sex, and cardiovascular risk factors) predicts benefit; therefore, estimating CVD risk identifies patients who should be offered statins.2
CVD risk assessment has been a fundamental part of clinical guidance on CVD prevention in the UK and internationally for two decades.3–5 In the UK, an absolute risk of CVD greater than a threshold was, and remains, the main criterion for offering statins.6,7 The National Institute for Health and Care Excellence (NICE)7 recommends that GPs use QRISK2 (introduced in 2012) to estimate 10-year CVD risk.2 Other risk calculators were used before this and were still available after 2012.
Estimated CVD risk is the best predictor of the benefits of statin treatment and is essential for effective shared decision making.8 Evidence suggests that the use of risk scoring improves the accuracy of perceived CVD risk and medical prescribing without causing harms.9,10 The use of CVD risk scoring should result in more targeted prescribing, but there is evidence both of undertreatment of high-risk patients and overtreatment of low-risk patients.11–15 This may be because risk scores are not consistently used by clinicians16 or because clinical information not incorporated into the risk scores is being taken into account.
In 2014, the NICE guidelines for England and Wales on lipid modification reduced the CVD risk threshold for offering statins from 20% to 10% 10-year risk.6,7 The benefit of lowering the threshold has been questioned.17 The medical community and lay media have raised concerns about overprescribing of statins, questioning the clinical benefit and potential for harm.18,19
The aim of this study is to examine how trends in initiating statins for the primary prevention of CVD relate to QRISK2 scoring and how these have changed over recent years, with particular focus on the impact of the 2014 NICE guidance. This will provide new information on the impact of, and adherence to, clinical guidelines in the UK.
METHOD
This was a historical cohort study using data from anonymised primary care records of practices in England and Wales contributing to The Health Improvement Network (THIN) database. The authors had full access to the database. THIN has been used in previous studies to validate QRISK2 and it was shown that the discrimination statistics in THIN are as good as those for the original QRISK2 cohort.20,21 Practices that contribute to THIN use the Vision (In Practice Systems) electronic patient records system.22 Clinical data are coded using Read Code clinical classification version 2,23 and drug codes correspond to the British National Formulary.24 Codes used are available from the authors on request.
How this fits in
This study confirms that there is potential undertreatment of patients at high risk of cardiovascular disease (CVD) and, although only a small proportion of low-risk patients are initiated on statins, low-risk patients represent a significant proportion of all statin initiations. The study has also demonstrated that the reduction in risk threshold for offering statins recommended in the 2014 National Institute for Health and Care Excellence guidelines has not resulted in the massive increase in statin initiations that was anticipated. This study indicates that only one-quarter of patients have evidence of formal CVD risk assessment with QRISK2 before statin initiation despite the fact that this is essential information for shared decision making and to determine treatment eligibility.
To maintain a stable cohort, only practices that contributed data for the whole study period (from the beginning of 2000 to the end of 2015) were included. Patients had to be suitable for CVD risk assessment according to NICE guidance,6 and should not have been prescribed statins (or other lipid-lowering therapy) in the past. Patients with chronic kidney disease stages 3–5, type 1 diabetes mellitus, or familial hypercholesterolaemia were excluded as risk assessment is not required for statin initiation. Patients were eligible for inclusion from the earliest of the following dates: study start date, acceptable mortality reporting date (which ensures that patient deaths and deregistrations are being recorded consistently), Vision installation date plus 1 year, registration date plus 1 year (to ensure time for baseline data to be recorded), and age 40 years; until the earliest of the following dates: age 85 years, study end date, CVD diagnosis, statin initiation, recording of a contraindication for the prescribing of statins, death, and transfer out of the practice.
All QRISK2 scores recorded during the study period were included (individuals may have had several scores recorded). Practice ID, country, ethnicity, Townsend deprivation quintile, sex, and year of birth were identified. Patients with missing sex or year of birth, or a QRISK score greater than 99.99%, were excluded. A ‘missing’ category was used for other missing data.
Primary analysis
Following a descriptive analysis of the cohort, the rates of statin initiations and QRISK2 recording per year were calculated. Sub-analyses were performed to establish these rates by demographic variables (sex, age, and Townsend deprivation quintile). Rates were not adjusted for these variables.
Secondary analysis
Relationship between QRISK2 scoring and statin initiation
QRISK2 scores were categorised into low (<10%), intermediate (10–19.9%) and high (>20%) 10-year CVD risk. In each category, the proportion of patients initiated on statins following QRISK2 scoring was established based on the patient’s latest record.
Coded CVD prevention encounters were categorised into QRISK2 score with subsequent statin initiation, QRISK2 score without statin initiation, and statin initiation without prior QRISK2 score. The proportion of initiations with/without a recorded QRISK2 score were reported by patient demographic characteristics. Statistical significance was assessed using Pearson’s χ2 tests.
Impact of NICE guidance
The mean recorded QRISK2 score for patients initiated on statins was calculated before and after the updated NICE guideline publication (July 2014). The annual proportion of statin initiations in each QRISK2 category (risk scores within 60 days of prescribing) was reported from 2012 to 2015 to reveal any change in the pattern of prescribing.
RESULTS
After excluding three patients who had a QRISK2 score greater than 99.99%, the cohort consisted of 1 422 664 patients from 248 practices, with a total of 9 437 754 patient-years of follow-up between 2000 and 2015. The median observation period was 5.65 years (interquartile range: 2.50 years–10.50 years). A total of 217 860 patients were initiated on a statin (15.31%, 95% confidence intervals (CI) = 15.25% to 15.37%) and 151 788 patients had at least one QRISK2 score recorded (10.67%, 95% CI = 10.62% to 10.72%). Of the patients with a recorded QRISK2 score, 80.2% had just one score, 15.1% had two scores, and 4.6% had more than two scores recorded (range 3–13). The demographic characteristics of the cohort are shown in Table 1.
Demographic characteristics of cohort (n = 1 422 664)
Statin initiation trends
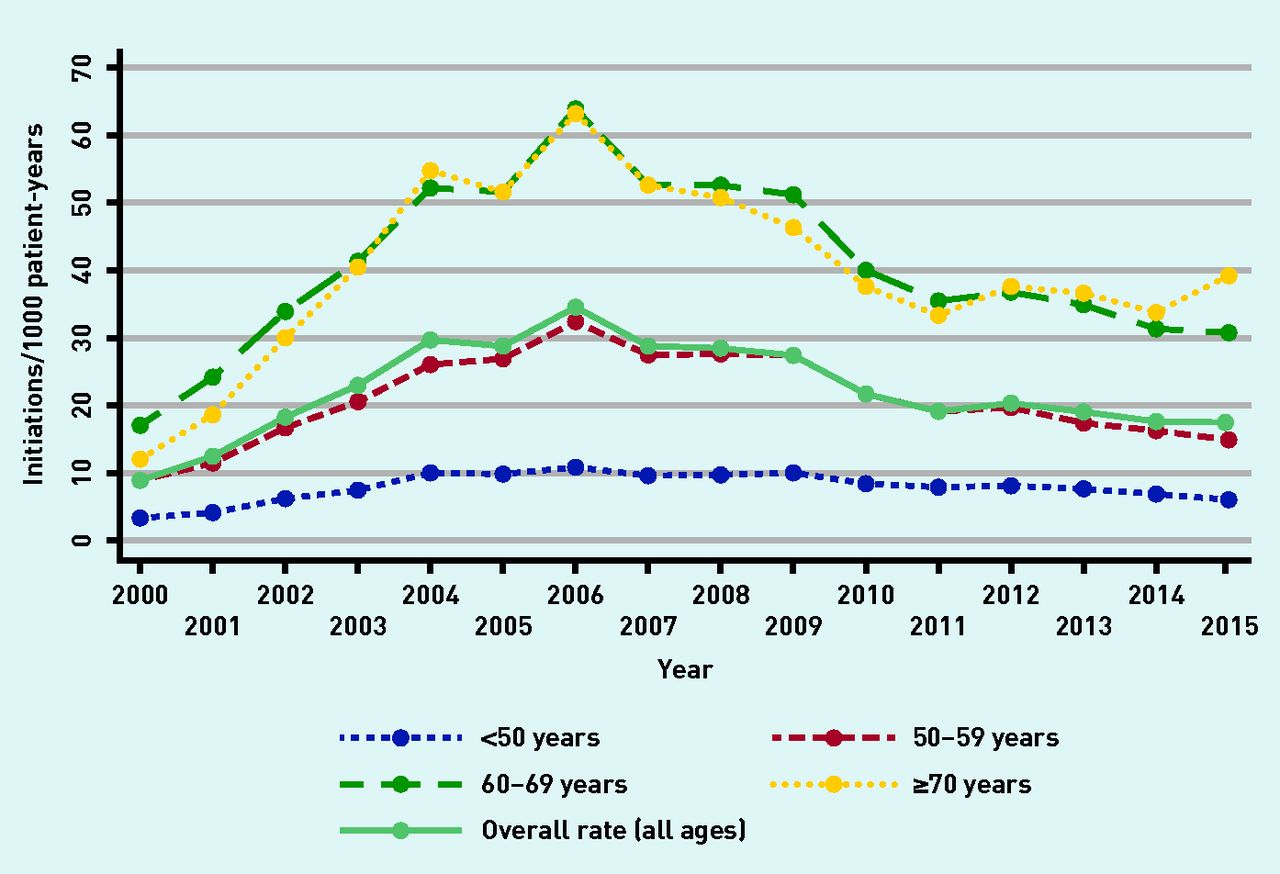
From 2000 to 2006 there was an increase in the rate of statin initiations from 9.05 (95% CI = 8.66 to 9.45) initiations/1000 patient-years to 34.41 (95% CI = 33.95 to 34.87) initiations/1000 patient-years. The rate then declined to 17.26 (95% CI = 16.95 to 17.57) initiations/1000 patient-years in 2015 (Figure 1). Males had a higher overall annual initiation rate than females (25.5 versus 20.9, P<0.001) (not adjusted for other characteristics).
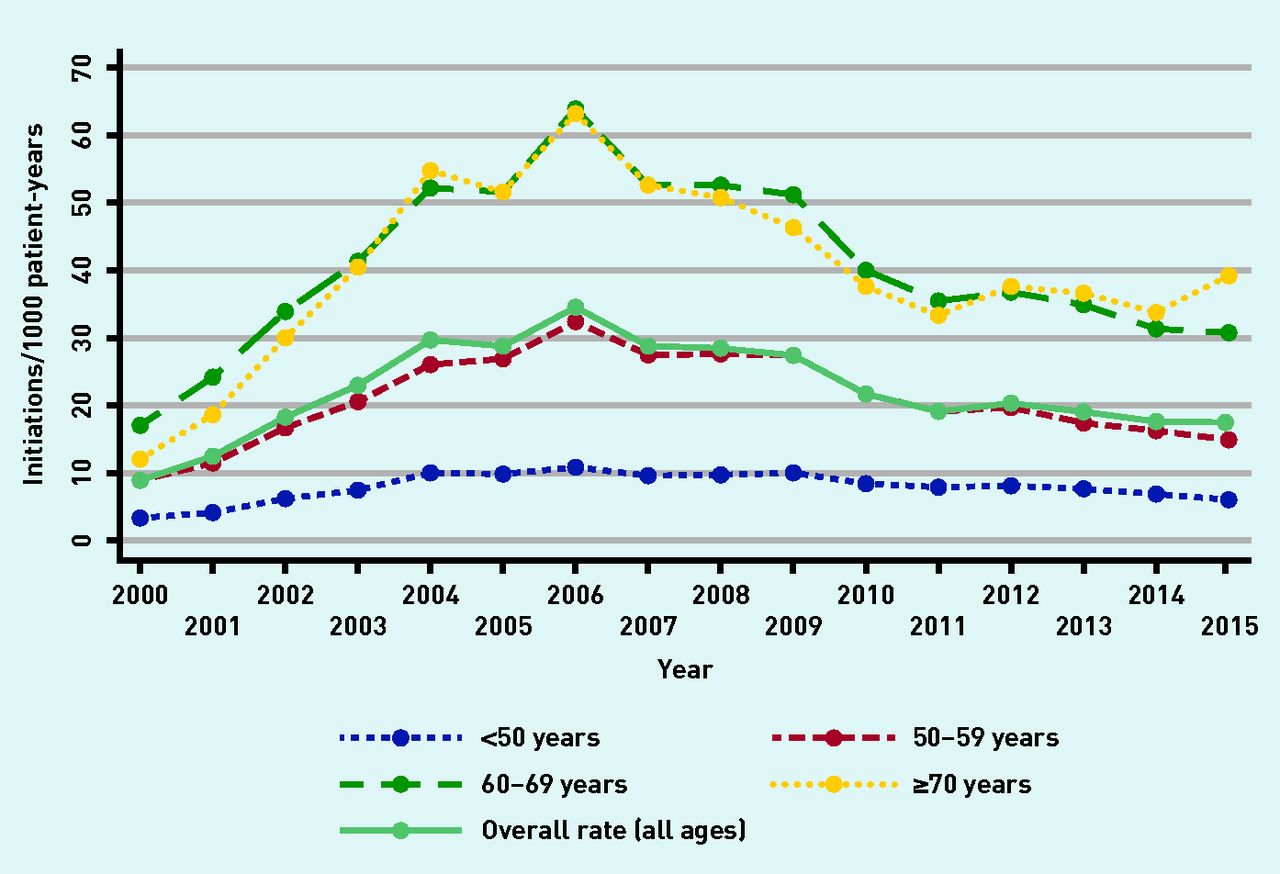
Rate of statin initiation by age group 2000–2015.
Trends in the recording of QRISK scores
From the introduction of the QRISK2 code (2012) until 2015, there was a steady increase in the recording of QRISK2 scores from 31.6 (95% CI = 30.2 to 33.1) to 99.1 (95% CI = 96.6 to 101.7) per 1000 patient-years. Females had an overall unadjusted rate of QRISK2 recording of 61.4 (95% CI = 61.0 to 61.8) scores/1000 patient-years compared with 51.7 (95% CI = 51.3 to 52.1) QRISK2 scores/1000 patient-years for males.
Association between QRISK2 scores and statin initiation
Most patients who had a QRISK2 score documented did not subsequently have a statin prescribed (90.2%, 95% CI = 90.0% to 90.3%). Table 2 shows the number of patients in each QRISK2 category and the proportion initiated on a statin. Low-, intermediate-, and high-risk patients accounted for 16.6%, 37.1%, and 46.3% of all patients prescribed a statin following recorded QRISK2 assessment.
Proportion of patients with previous CVD risk assessment initiated on statins by QRISK2 category and time period
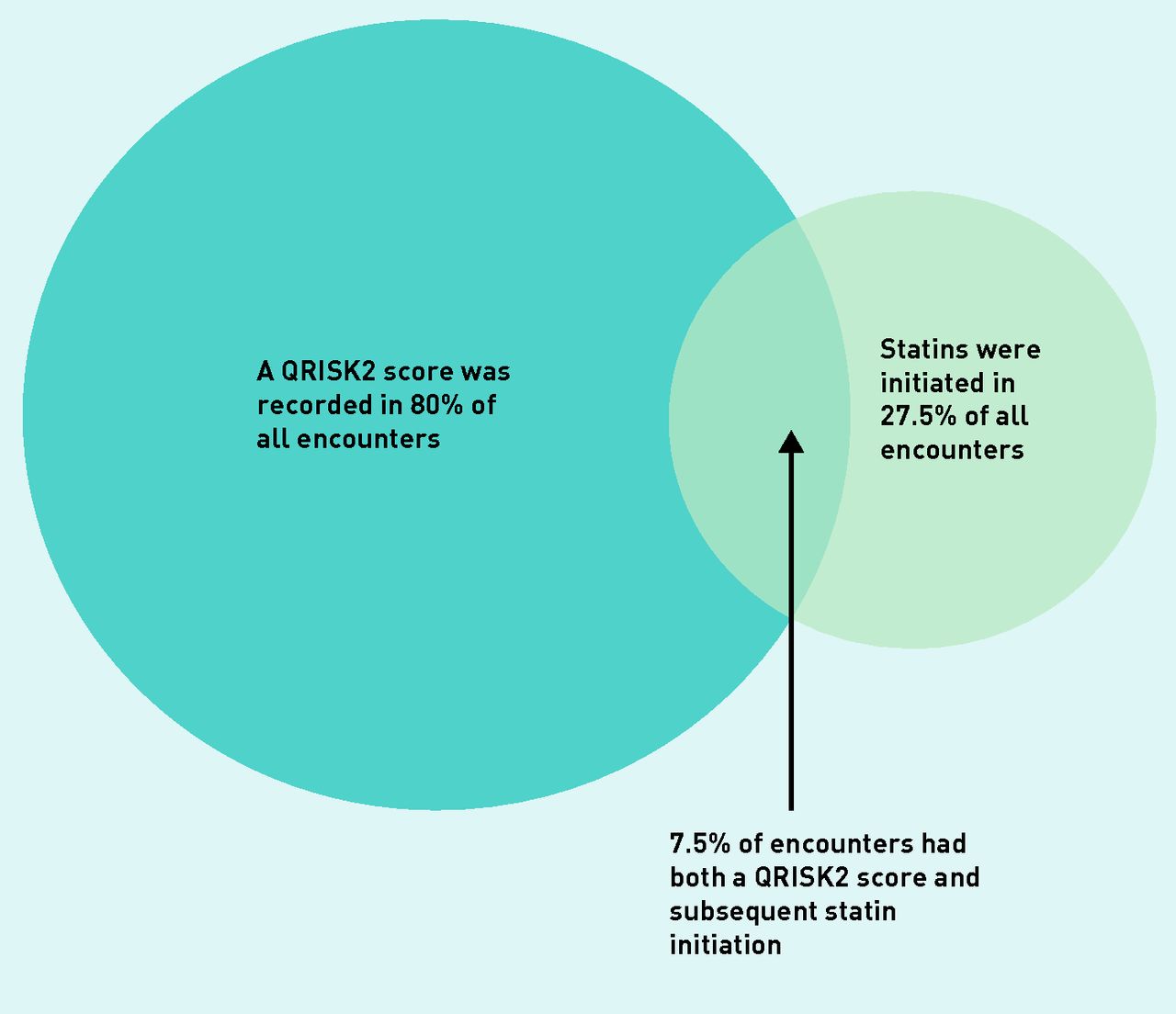
Since 2012, 72.9% (95% CI = 72.5% to 73.3%) of patients initiated on a statin did not have a QRISK score recorded at any time. The outcomes of clinical encounters involving the initiation of statins or recording of QRISK2 score are illustrated in Figure 2. Table 3 demonstrates the variations in these outcomes for different demographic groups. The proportion of statin initiations that occur without a recorded QRISK2 score was relatively consistent, with the notable exception that younger patients seemed to have a higher proportion of initiations without a recorded risk assessment.

Coded outcomes of CVD prevention clinical encounters (an encounter may include more than one consultation).
Variation in QRISK2 score recording and statin prescribing according to demographic group from clinical encounters relating to CVD in 2012–2015
Impact of NICE guidance on QRISK2 scoring and statin prescribing
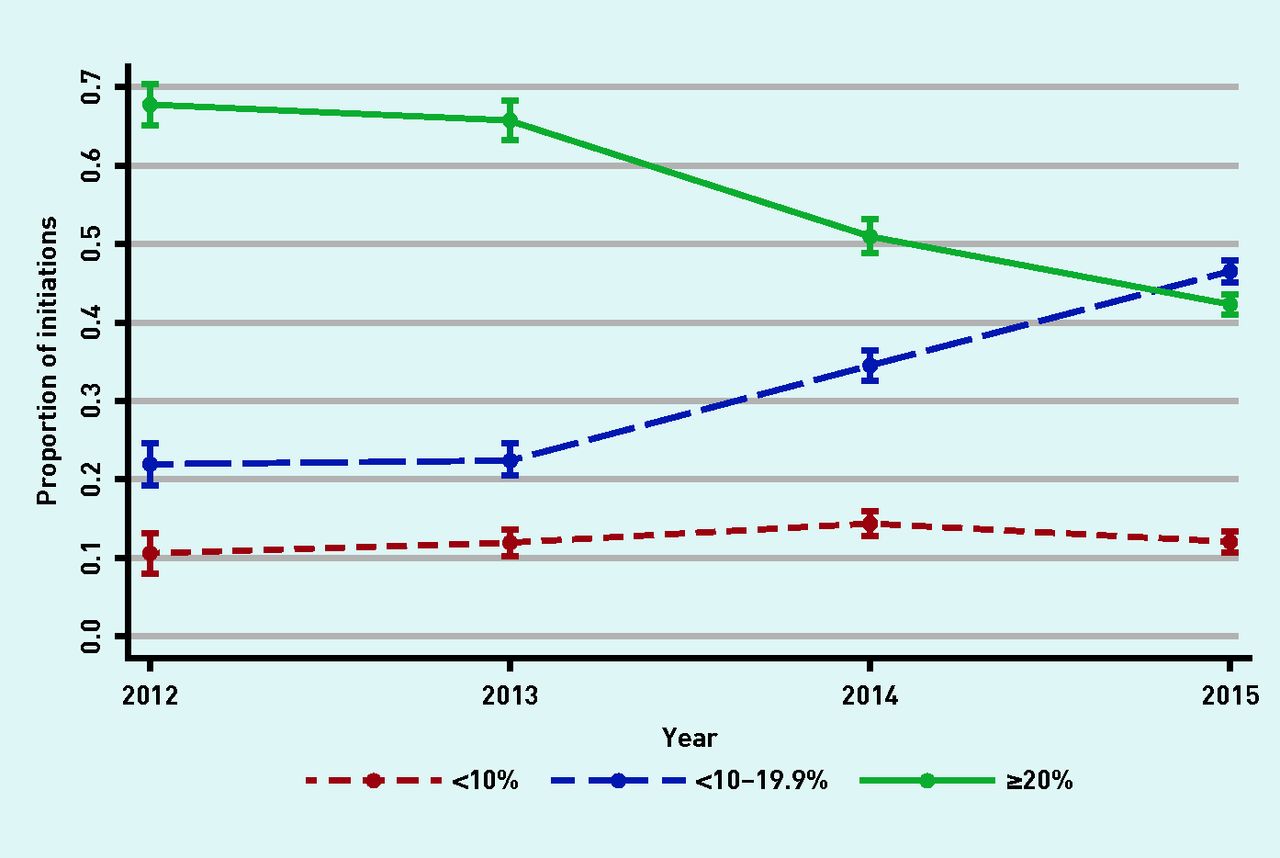
When examining risk scores that were calculated within 60 days of statin initiation, the mean QRISK2 score before the 2014 guidance was 23.06, dropping to 19.28 after July 2014 (P≤0.001). Figure 3 shows that an increasing proportion of statin initiations occur in the 10–19.9% QRISK2 category in 2014/2015 while initiations in the high-risk category (>20%) continue on a declining trajectory.

{kind=link}
{kind=link}
{kind=link}
Statin initiations with QRISK2:a proportion in each QRISK2 category. aQRISK2 score within 60 days prior to statin initiation.
For patients with a recorded QRISK2 score (at any time), the proportion of statin initiations that were consistent with prevailing NICE guidelines increased from 51.9% (2008 guideline) to 85.3% (2014 guideline) (Table 2). This change is mostly accounted for by the patients with a QRISK2 score of 10–19.9%.
DISCUSSION
Summary
The rate of statin initiations has halved since 2006. The initial peak in statin initiations may have been influenced by a dramatic reduction in the cost of prescribing when simvastatin came off patent in 2003. In addition, there were major publications on CVD prevention around this time including the Joint British Societies’ guidelines and a NICE technological appraisal recommending the use of statins.25,26 This may have resulted in saturation of the population of patients who were eligible and willing to take statins over the next few years. This could explain the decline in initiations from 2006 to 2015, as patients who could potentially be prescribed statins would be the newly eligible (lower risk) or those less active in seeking treatment. Additionally, over this period there was increased focus on the adverse effects of statins because data from observational studies differed from trial findings,27 which may have influenced both the clinicians’ decision to prescribe, and the patients’ decision to accept, treatment.
The rate of QRISK2 coding has shown a steady increase since it became available in 2012. Most patients who had a QRISK2 score calculated were not prescribed a statin in the following 60 days, even those found to be in the high-risk category. It is not possible to establish whether those patients who were above the threshold to be prescribed a statin did not receive treatment because they were not offered it or because they declined an offer. Older patients (aged >70 years) were less likely to have a QRISK2 score recorded than patients aged 50–69 years. Younger patients were more likely to be initiated on statins without recorded QRISK2 assessment than older patients.
Most patients initiated on statins since 2012 did not have a prior QRISK2 score recorded. Of those that did, one in six patients were in the low-risk category and should not have been offered a statin according to NICE guidance. These findings indicate that factors other than risk score were being considered when initiating statins. It is possible that clinicians were responding to individual patient preference when prescribing to low-risk patients, but without a discussion about risk (informed by a risk estimate) these preferences cannot be fully informed. It appears that the 2014 NICE guidance changed clinicians’ behaviour as the rate of statin initiation among patients in the intermediate-risk category (10–19%) increased while the high-risk initiation rate continued to decrease.
Strengths and limitations
THIN includes a large number of practices that are generalisable to the UK population.28 This permits identification of prescribing trends across large numbers of patients over a 16-year period. This period included 18 months of data after the publication of the 2014 NICE guidance, which is sufficient time to identify changes in prescribing and coding behaviour. Prescribing data is well recorded because prescriptions are generated and recorded by the clinical system.
Only QRISK2 scores that were entered automatically or manually as coded data in the electronic patient record could be identified. It is possible that clinicians calculated a QRISK2 score but did not enter it as coded data. This would result in an underestimate of the rate of QRISK2 scoring and the proportion of patients being prescribed a statin after QRISK2 score. Additionally, some clinicians may have used alternative risk calculators in their decision making. Risk scores calculated using an alternative calculator were not identified and this may lead to an underestimate of the use of risk estimation in decision making.
The study assumed that a QRISK2 score within 60 days of statin initiation was likely to be taken into consideration when deciding if a statin should be initiated. It is possible the QRISK2 score was not considered, or that scores older than 60 days featured in the decision. The latter would lead to an underestimate of the proportion of patients initiating statins on the basis of QRISK2 score.
Importantly, the decision to prescribe statins is a clinical decision and should not be based on QRISK2 score alone. Patient preferences, comorbidities, and individual patient circumstances will all inform the shared decision to prescribe statins. Some guideline-incongruent decisions will have been clinically justifiable but it is not possible to identify this from the data.
Comparisons with existing literature
The peak in statin initiation in 2006 has previously been reported by O’Keeffe et al29 who used the same database so the initiation patterns are identical. However, their study ended in 2013 so they would not have observed any effects of the 2014 NICE guidance.
Matthews et al 30 observed a steady increase in statin initiations for primary prevention between January 2011 and October 2013 rather than the decline in initiations observed in the current study. This may be explained by the fact that Matthews et al only identified statin initiations for primary prevention in patients with a preceding CVD risk score. The results of the current study would suggest that this definition would exclude up to 75% of initiations.
Other studies considering the relationship between risk score and statin prescribing have used post hoc risk calculations12,14 or risk scores that were collected for the purpose of research,15 so it is difficult to imply that prescribing decisions were based on risk scores. Homer et al13 did use routinely collected risk scores, but their data were limited to a specific geographical area and they found that nearly 60% of patients suitable for risk assessment had a risk score documented. The current study found that only 11% of the population had a coded risk score, suggesting that Homer et al’s results may not be generalisable to the rest of England and Wales.
Balder et al 15 considered whether statin prescriptions were consistent with guidelines in the Netherlands. They classified 66% of prescriptions as guideline-inconsistent. In the UK, previous studies have found that 58.3%12 and 58.1%13 of prescriptions were guideline-inconsistent. This study found lower rates of guideline-inconsistent prescribing (48.1%) under the 2008 guidance. Guideline-inconsistent prescribing decreased to 14.7% from July 2014, but this is as a result of the guidelines changing to be more in keeping with practice rather than the other way around. Guidelines consistently recommend that patients with a CVD risk below 10% should not be prescribed statins. However, the current study found that 2.7% of patients in this category were prescribed a statin (Table 2), which is lower than other studies (2.9%,15 3.7%,13 and 5.0%14), suggesting improved concordance with guidelines.
Implications for research and practice
As CVD risk estimation is instrumental in the decision to initiate statins, all patients should have a documented CVD risk score before statin initiation. It is possible that a higher proportion of statin initiations are based on patients’ individual risk than the data in this study indicate, but the medical record should routinely reflect the incorporation of risk score in this decision.
Further research needs to be carried out to understand why some patients do not undergo risk assessment before statin initiation and on what basis the decision to prescribe is founded if risk assessment is not used. It is also important to identify why low-risk patients are initiated on statins and whether high-risk patients who are not initiated on statins represent missed opportunities to lower CVD risk or an appropriate, informed and shared decision.
Acknowledgments
Samuel Finnikin was supported in this project by National Institute for Health and Care Excellence (NICE) through his role as a NICE scholar 2015–2016.
Notes
Funding
Samuel Finnikin is funded through an In-Practice Fellowship awarded by the National Institute for Health Research (NIHR) (NIHR-IPF-2015-09-04). Tom Marshall was partly funded by the NIHR through the Collaborations for Leadership in Applied Health Research and Care for West Midlands (CLAHRC-WM). This article presents independent research funded by the NIHR. The views expressed in this publication are not necessarily those of the NIHR, the Department of Health, NHS Partner Trusts, the University of Birmingham, or the CLAHRC-WM Management Group.
Ethical approval
The THIN Data Collection Scheme was approved by the South-East Multicentre Research Ethics Committee in 2003. Individual studies using THIN require Scientific Review Committee approval. The original protocol for this study and a subsequent amendment have been approved (16THIN009A2).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received May 10, 2017.
- Revision requested June 19, 2017.
- Accepted July 18, 2017.
- © British Journal of General Practice 2017
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

