


Abstract
Background Telephone triage is used to assess acute illness or injury. Clinical decision making is often assisted by triage tools that lack callers’ perspectives. This study analysed callers’ perception of urgency, defined as degree of worry in acute care telephone calls.
Aim To explore the caller’s ability to quantify their degree of worry, the association between degree of worry and variables related to the caller, the effect of degree of worry on triage outcome, and the thematic content of the caller’s worry.
Design and setting A mixed-methods study with simultaneous convergent design combining descriptive statistics and thematic analysis of 180 calls to a Danish out-of-hours service.
Method The following quantitative data were measured: age of caller, sex, reason for encounter, symptom duration, triage outcome, and degree of worry (rated from 1 = minimally worried to 5 = extremely worried). Qualitative data consisted of audio-recorded telephone calls.
Results Most callers (170 out of 180) were able to scale their worry when contacting the out-of-hours service (median = 3, interquartile range = 2–4, mean = 2.76). Degree of worry was associated with female sex (odds ratio [OR] 1.98, 95% CI = 1.13 to 3.45) and symptom duration (>24 hours: OR 2.01, 95% CI = 1.13 to 3.45) (reference <5 hours), but not with age or reason for encounter. A high degree of worry significantly increased the chance of being triaged to a face-to-face consultation. The thematic content of worry varied from emotions of feeling bothered to feeling distressed. Callers provided more contextual information when asked about their degree of worry.
Conclusion Callers were able to rate their degree of worry. The degree of worry scale is feasible for larger-scale studies if incorporating a patient-centred approach in out-of-hours telephone triage.
- after-hours care
- computer-assisted decision making
- mixed methods
- patient participation
- self-rated worry
- telephone helpline
- triage
INTRODUCTION
Most people are good at predicting their own morbidity and mortality by self-rating their health,1 but it is unclear whether they are equally good at predicting their own need for help in situations when they have acute illness or injury. Triage tools are recommended in acute care to provide safe and efficient assessment of urgency and appropriate type of care,2 but generally fail to incorporate the caller’s perspective.3 It is possible that patients are capable of providing unspoken information on symptom severity and that their perception could prove valuable in telephone triage.
A normal reaction to illness or injury is problem-solving behaviour, in which worry has been described as the emotion that leads to problem-solving behaviour.2 It might be useful for the caller’s self-evaluation of urgency (defined as degree of worry) to be systematically incorporated into triage tools.
This study aimed to explore the ability of callers to telephone triage to quantify their degree of worry, the association between their degree of worry and variables related to the caller, the effect of the degree of worry on triage outcome, and the thematic content of the caller’s worry.
METHOD
Design
A mixed-methods study with simultaneous convergent design was conducted.4 Quantitative data (descriptive statistics, associations of variables, and effect of degree of worry on triage response) and qualitative data (thematic analysis of telephone dialogues) were collected simultaneously. The qualitative and quantitative strands contributed equally to the results.
Setting
The out-of-hours and emergency services in Denmark’s capital, Copenhagen, are combined in one organisation, and are accessible via two telephone numbers: 112 for emergency calls and 1813 for less urgent calls.5 The helpline for less urgent calls is available from 4pm to 8am on weekdays and around the clock on weekends and holidays. Telephone triage is used to preassess the need for the caller to access acute medical help.
Annually, the out-of-hours service handles about 1 million calls. Call handlers are nurses or physicians (in either primary or secondary care), who triage the caller to self-care, to their own GP on the next working day, to hospital consultation, to a home visit, or to direct hospitalisation. The call handler’s clinical decision making is guided by a locally developed, criterion-based decision tool (visitor guide, Denmark, Copenhagen, 2011).
How this fits in
Triage tools for non-urgent conditions often do not include the patient’s perspective. Callers to emergency care are able to rate their degree of worry. Degree of worry can be scaled on a continuum from problem focused to emotional coping. Asking callers about self-rated worry seems feasible in order to incorporate patient involvement in urgent-care telephone triage.
Data collection
Study population
Calls concerning somatic illness in adults (aged ≥15 years) were included. Calls made on behalf of another person, or concerning life-threatening problems or logistical problems (such as transportation) were excluded. Participating call handlers collected data on 3 consecutive days: Wednesday 30 March and Thursday 31 March 2016 (4pm to 10pm), and Friday 1 April 2016 (8am to 4pm), which was a bank holiday. A convenience sample of calls to the out-of-hours service in Copenhagen was included.
Data sources
Two data sources were used: internal patient registration (data on age, sex, and triage outcome such as face-to-face consultation at an emergency department or advice on how to self-care) and recorded voice logs of the calls (to describe the emotional manifestations of degree of worry, reason for encounter, symptom duration, and degree of worry).
Call handlers were instructed to assess the callers’ degree of worry. All call handlers were invited (by e-mail and at a staff meeting) to collect data and they received instruction about the data collection, criteria for inclusion, focus of the study, and voluntary caller participation. Question sequence and phrasing were tested in calls 2 weeks before data collection by two experienced call handlers, and revised according to their recommendation. The call handler’s greeting to out-of-hours calls was, for example: ‘This is the medical helpline, how can I help you?’ At the call handler’s discretion, the caller was invited to participate in the study, giving their verbal informed consent. Subsequently, data collection was carried out by the call handler posing the following question: ‘How worried would you say you are on a scale from 1 to 10 for the condition you are calling about today?’
Degree of worry was registered on a scale (1–10) similar to the Numeric Rating Scale, which is regarded as equally good for rating pain as the Visual Analogue Scale in clinical settings.6 In calls where the callers failed to provide a numeric response reflecting their degree of worry, an intensity descriptor/converter was used to convert the spoken word to a numeric value6 by two researchers carrying out an independent assessment. The differences were solved through discussion, resulting in a final degree of worry score.
Quantitative data collection
Variables for the quantitative strand were: age group (15–30, 31–45, 46–60, ≥61 years), sex, duration of symptoms (<5 hours, 5–24 hours, >24 hours), reason for encounter (injury, acute illness, exacerbation of chronic disease), triage outcome (self-care advice, referral to GP, call transferred to physician, consultation at hospital, direct hospital admission, or other), and degree of worry. Triage outcome was divided into face-to-face consultation (hospital consultation, hospital admission, or other) and telephone consultation (self-care advice or contact with a GP during office hours.
Quantitative data analysis
Descriptive analysis was performed using frequency distributions (number, percentage), median value, mean, and interquartile range (Q1–Q3). Degree of worry was aggregated into a five-point ordinal scale ranging from 1 = minimally worried to 5 = extremely worried. The associations between quantified degree of worry and age, sex, reason for encounter, and symptom duration as explanatory variables were analysed using ordinal regression. The association between triage outcome and degree of worry was analysed using logistic regression. Backward elimination was used to obtain a model including only significant variables. Results were reported as odds ratios (ORs) with 95% confidence intervals (95% CIs), and P-values when appropriate.
Finally, a non-response analysis on sex and age was carried out, comparing the non-responders with responders in the study period using Wilcoxon’s rank sum test (age) and Fisher’s exact-test (sex). A P-value <0.05 was considered significant for all analyses. Data were analysed using Excel (version 7.9) and SAS Enterprise Guide (version 7.12). The quantitative part of the study is reported in accordance with the STROBE statement.7
Qualitative data analysis
The qualitative strand was created by transcribing the recorded voice logs,8,9 focusing on emotional factors leading to the out-of-hours contact. Thematic analysis was carried out by two of the authors, as described by Braun and Clarke.10 Transcribed voice logs were coded inductively and sample size was determined by the number of included calls over the 3-day period; however, informational saturation was obtained.11 In the transcription process every voice log was categorised according to the final degree of worry; the initial coding was carried out while blinded to the degree of worry category to internally validate the findings. The initial codes were clustered into themes, and data were systematically reviewed to ensure that name, definition, and exhaustive set of data supported the theme.
Mixed-method analysis
The data strands were merged to provide one interpretation of the interface between data sources. This was carried out by horizontal analysis of the unblinded (to degree of worry) dataset and construction of matrices and themes. The thematic-and-mixed analysis was supported by investigator triangulation and differences were resolved by consensus. NVivo (version 10) was used for coding and analysis, and the results are reported according to the COREQ criteria.12
RESULTS
Study population
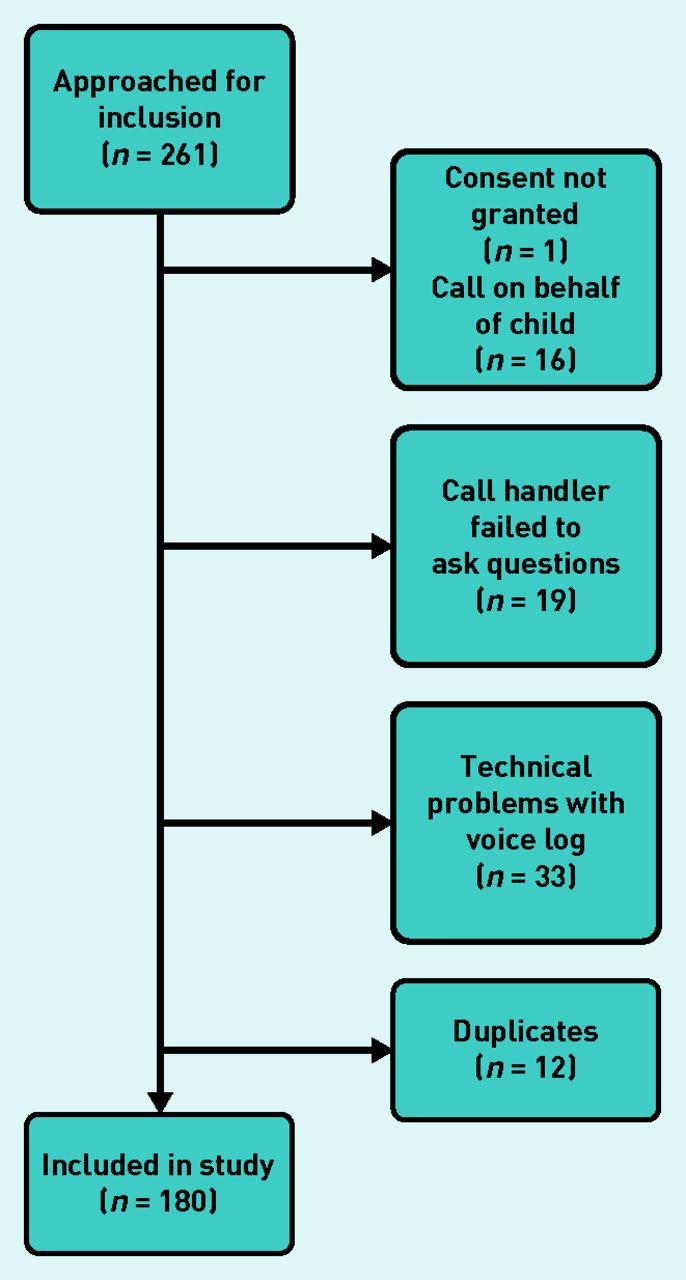
A total of 261 eligible callers were invited to participate in the study and, after exclusion, there were 180 consenting participants remaining (Figure 1). Most participants (n = 170; 94.4%) were able to numerically rate their degree of worry (Table 1). The median degree of worry was 3, interquartile range (IQR) = 2–4 (mean = 2.76) with a right skewed distribution. Telephone consultations lasted 3–12 minutes. The median age of included callers was 33 years (IQR = 25–49) and 63% (n = 113) were female. Reasons for encounter were injury (n = 37), acute illness (n = 120), exacerbation of chronic disease (n = 15), other (n = 7), and undetermined (n = 1).
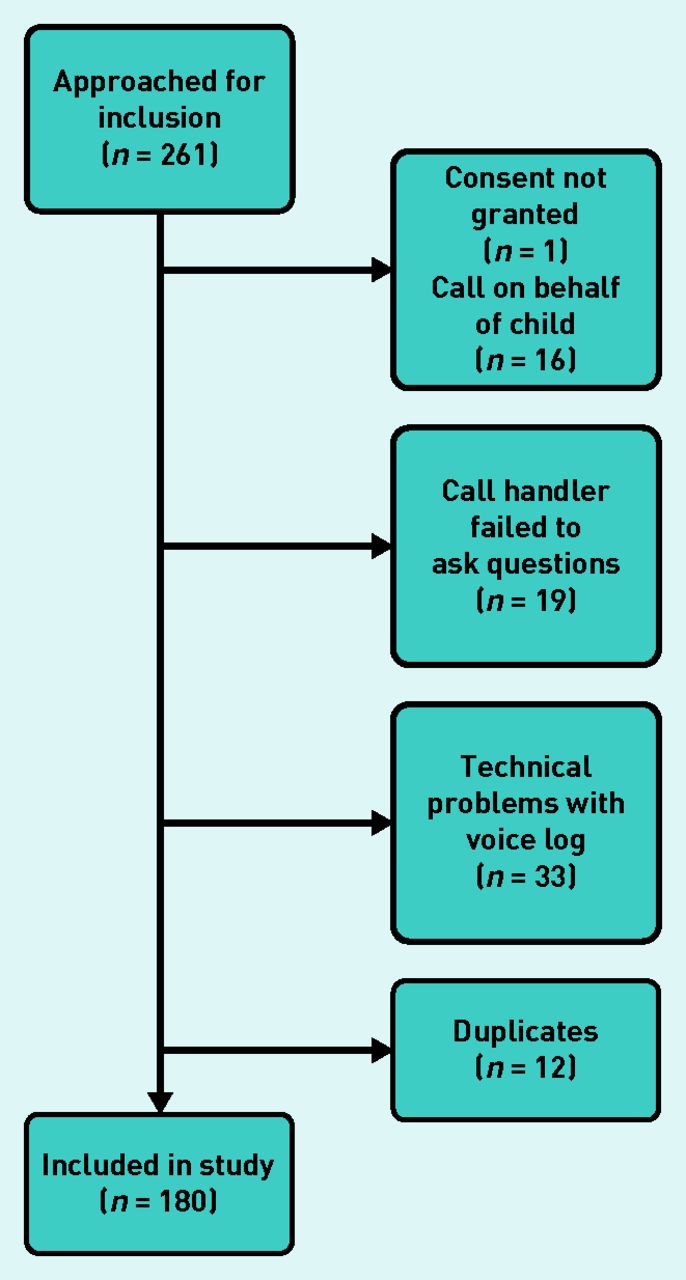
Flowchart showing number of calls included.
Data on degree of worry, sex, age, symptom duration, reason for encounter, and triage outcome of callers to telephone triage
Quantitative results
Association with degree of worry
The median degree of worry was 3 (IQR = 2–4) for females (mean = 2.90), which was significantly higher than for males, whose median degree of worry was 3 (IQR = 1–3) (mean = 2.52) (OR 1.98, 95% CI = 1.13 to 3.45). The association between symptom duration (<5 hours, 5–24 hours, and >24 hours) and degree of worry was significant (P = 0.028). Callers with symptom duration >24 hours had a significantly higher degree of worry than callers with symptom duration <5 hours (OR 2.01, 95% CI = 1.13 to 3.45). Age and reason for encounter were not significantly associated with degree of worry.
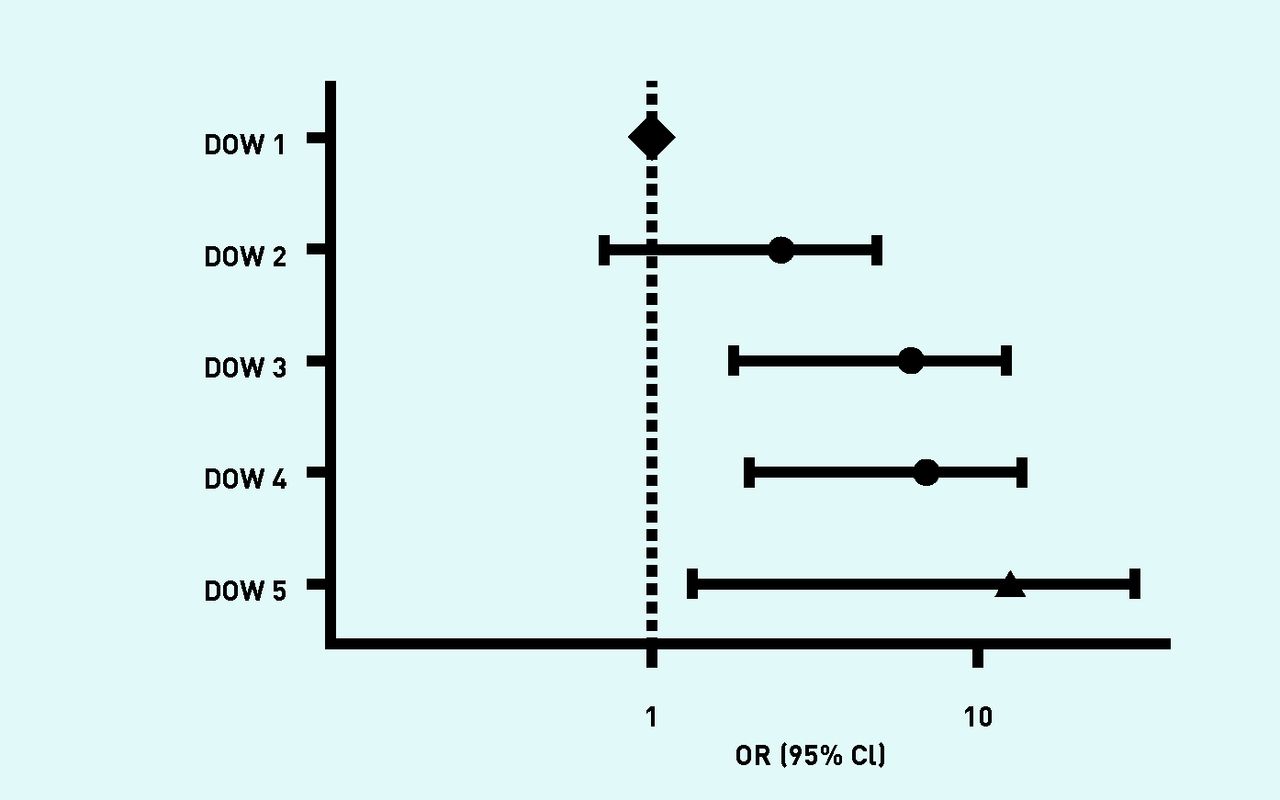
A degree of worry >2 resulted in more face-to-face consultations (degree of worry = 5 versus 1: OR 6.1, 95% CI = 1.3 to 29.5) (Figure 2). Age and reason for encounter were not associated with dichotomised triage outcome (face-to-face consultation or telephone consultation), and the elimination of these variables had little effect on the estimates.
{kind=link}
{kind=link}
Odds ratio for being triaged to face-to-face consultation versus telephone consultation only.a
a Degree of worry (DOW) 1 is used as reference. Model adjusted for sex and age
Non-response analysis
The study group was significantly younger than all callers in the study period, but there was no difference in sex distribution (P<0.001).
Qualitative results
Types of worry
Thematic analysis of emotional response to worry resulted in nine sub-themes (Table 2), which were reduced to five sub-themes that were expressed as scaled emotion (degree of worry). The emotional responses described a continuum of emotions ranging from ‘bothered’ to ‘distressed’ (Tables 2 and 3). These states translated to the categories of scaled degree of worry: ‘minimally worried’, ‘slightly worried’, ‘worried’, ‘very worried’, and ‘extremely worried’ (Table 3).
Emotional reasons for telephone contact and the result of the mixed horizontal analysis
Scaled emotion and mixed analysis of narratives as presented by callersa
Analysis of the voice logs showed that the questions ‘How worried are you?’ and ‘Can you tell me why you are worried?’ prompted new information such as additional information on chronic disease, a more extensive medical history, or a detailed family history.
DISCUSSION
Summary
This study found that it was possible for callers to score their degree of worry when calling a medical helpline. Sex and symptom duration could explain some variation in caller’s degree of worry. Moreover, a high degree of worry was associated with higher odds for being seen in a face-to-face consultation. The scaled degree of worry ranged in a continuum from minimally worried (degree of worry = 1) to extremely worried (degree of worry = 5) with the connecting themes: bothered, concerned, insecurity, sense of urgency, and distressed.
Strengths and limitations
The advantage of this study was the mixed-methods study design and minimal risk of recall bias. Incorporating the patient perspective into acute health care by using degree of worry was found to be feasible.
The study had some limitations. The question of worry and worry intensity was not uniformly articulated at the beginning of the telephone consultation, which could influence the stated worry intensity — especially if the telephone consultation itself had a worry-relieving effect. The convenience sample implies a risk of selection bias. Call handlers found it difficult to ask very distressed callers about their degree of worry. Thus, the study population was most likely not representative of the total population of callers because it mainly included patients with a lower degree of worry, which would skew the result in the direction of less degree of worry. A trend towards an effect of increasing degree of worry on odds for face-to-face consultation was observed. Furthermore, caller personality characteristics, such as trait, were not included, which might confound the results.
Comparison with existing literature
Degree of worry has been explored in three small-scale studies in the same study population (n = 62) in Finland, which aimed to explore the precursors for excessive health anxiety in young adults consulting their GP.13–15 The participants were asked to rate their worry on a Visual Analogue Scale (0–100), with a score above 50 defining the person as worried.14–15 Perception of the duration and course of the complaint together with psychological characteristics were associated with the degree of worry expressed by primary care patients.13 The studies also found that uncertainty, being left without an explanation, and the seriousness of an illness defined as the impaired ability to function characterised the worry voiced before a doctor’s consultation.15 These findings13–15 are in line with the present study and could be seen in the context of the self-regulatory model by Leventhal.16 Leventhal et al’s theory on help-seeking behaviour proposes that a situational stimulus (symptom) is followed by a cognitive and emotional response, a behavioural reaction (coping), and appraisal of the efficacy of these behaviours. Representation of illness consists of five cognitive representations: identity — the label that the person assigns the symptoms; consequences — the expected outcome of the symptoms; cause — idea of what caused the illness; timeline — expected duration of the illness; and perceived cure or control over the disease.16 In the current study, worry leading to help seeking could be scaled from the problem oriented to the very emotional.17
The lack of association between age and degree of worry corresponds with the findings of Kolk et al,18 who described that the effect of age was mediated by the number of chronic diseases (older people experience more chronic disease). The Finnish studies did not find a sex difference in degree of worry,14,15 whereas the current study found that females reported a slightly higher degree of worry. Two Danish studies found that females report their self-rated-health as being worse than males.19 A sex variation in self-reported health is a generally known phenomenon,18 which might be comparable to self-rated degree of worry.
The finding of the current study that degree of worry is associated with duration of symptoms and perceived medical urgency has not been seen in other studies. The Finnish studies were carried out in daytime primary care and used a symptom duration of more or less than 2 weeks.13 The current study used a shorter time frame corresponding to the general aims of the out-of-hours care services in regard to time perspective. It did not find an association between degree of worry and reason for encounter, but quite general categories were used for reason for encounter. The authors conclude that degree of worry is not entirely free of context but this should not matter in regard to telephone consultation, when the complaints of the caller should be evaluated regardless of their age, sex, reason for encounter, and other characteristics.
This study showed an association between degree of worry and triage outcome, with callers having a degree of worry score >2 receiving more face-to-face consultations. The association between degree of worry and triage outcome could be mediated by a low feeling of control,20 or the fact that low-urgency problems to a large degree can be dealt with by performing self-care.21 A third explanation might be that the expectation of treatment is anticipated in the problem-solving sub-group of those whose degree of worry is 1–2 (such as obtaining a prescription), whereas a degree of worry of 4–5 might reflect a fear of having a more serious illness.
Implications for research and practice
The patient-centred approach of scoring degree of worry in telephone triage might be a beneficial addition to existing triage tools. The authors acknowledge that worry intensity might not be assessed easily by a single-item worry question, however, because of the complexity of coping when faced with illness or injury.
The authors hypothesise that the caller’s perception of urgency of the problem has the potential to improve decision making in telephone triage. Questioning the caller’s perspective invites the caller to take part in decision making and facilitates information sharing. Attempts should be made to explore the systematic incorporation of degree of worry and its effect on the caller, call handler, patient outcome, and healthcare use in calls to acute medical care services.
Further research would be beneficial to investigate the correlation of this patient-centred approach with healthcare use and whether more contacts can be dealt with by telephone consultation; its effect on the healthcare professionals providing telephone consultations and whether their clinical decision making is affected by the awareness of degree of worry; and its worry-relieving effect. This study may represent a paradigm shift in acute care by introducing patient participation and empowerment.22,23 Moreover, there is a possibility that the cognitive task of rating a degree of worry could provide an opportunity to empower callers24 by teaching patients health behaviour25 such as providing advice on self-care.
Notes
Funding
The Emergency Medical Services Copenhagen receives an unrestricted research grant from the Laerdal Foundation and the corresponding author is supported by the Danish Tryg Foundation (ID: 119443). None of these organisations had an impact on the results of this study.
Ethical approval
The study was approved by the Data Protection Agency (PVH-2015-004, I-Suite nr: 04330). All participants gave informed consent. The Ethical Committee was consulted but no permission was needed (H-15016323).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received August 7, 2017.
- Revision requested September 21, 2017.
- Accepted October 2, 2017.
- © British Journal of General Practice 2018
This article is Open Access: CC BY-NC 4.0 licence (http://creativecommons.org/licences/by-nc/4.0/).
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

