


Abstract
Background Patients can play a role in achieving an earlier diagnosis of cancer by monitoring and re-appraising symptoms after initially presenting to primary care. It is not clear what interventions exist, or what the components of an intervention to engage patients at this diagnostic stage are.
Aim The review had two aims: 1) to identify interventions that involve patients, and 2) to establish key components for engaging patients in the diagnosis of cancer in primary care at the post-presentation stage.
Design and setting Empirical studies and non-empirical articles were identified searching Ovid MEDLINE, PsycINFO, and Embase databases, relevant journals, and available key author publication lists.
Method Abstracts and titles were screened against inclusion and exclusion criteria. Qualitative synthesis of empirical research and current opinion from across all articles was used to select, organise, and interpret findings.
Results No interventions were found. Sixteen articles provided suggestions for potential interventions and components important at the post-presentation stage. Factors contributing to patients not always being engaged in assisting with diagnosis, strategies to foster patient involvement, and moderators and benefits to patients and health services (proximal and distal outcomes) were captured in a logic model.
Conclusion There is an absence of interventions involving patients during the post-presentation stage of the diagnostic process. Limited literature was drawn upon to identify potential barriers and facilitators for engaging patients at this diagnostic stage, and to establish possible mechanisms of change and measurable outcomes. Findings can direct future research and the development of interventions.
INTRODUCTION
It is estimated that 46% of all cancers in England are diagnosed at a late stage, resulting in lower survival and additional treatment costs.1 Delays in cancer diagnosis may occur at a number of stages during the diagnostic process.2–4 In a primary care setting, the patient interval (before presentation) rather than the primary care interval (after presentation) has been found to make a larger contribution to delay in 18 out of 28 cancers assessed.5 Work on factors involved in emergency presentations of cancer has also examined patients’ previous use of primary care.6,7 One finding was that some patients diagnosed with cancer during emergency presentations had delayed re-presenting back to primary care after an initial consultation for symptoms that might be related to their cancer symptoms (referred to as post-presentation stage from this point).6 Delayed re-presentation may contribute to a diagnosis at a point where treatment is less effective. Clear communication between the GP and patient about the possible meaning of symptom severity and persistence, and the patient’s role in following up and reviewing symptoms, are critical for early recognition, referral, and treatment for cancer.8,9
Though diagnostic error is little researched in the field of patient safety,10,11 interest in the role that patients may have in reducing delayed diagnosis and misdiagnosis, and improving health professionals’ diagnostic performance, has begun to gather pace. This is reflected in the recent Institute of Medicine12 report on diagnostic error, which proposes that patients are ‘a diagnostic team member’. The importance of patients and healthcare professionals working in partnership to avoid delay in the diagnosis of cancer is also an emerging topic and a key component in the increasing focus on safety netting.8,13 Although there is a growing appreciation that engaging patients in their own health care can achieve better outcomes through involvement in disease management14,15 and improving patient safety,16 little is known about how patients currently assist with cancer diagnosis in primary care.
Here, the authors report a systematic review that addresses this gap in understanding. The aims of the review were to consolidate existing knowledge on interventions that involve patients in the diagnosis of cancer in primary care at the post-presentation stage (Aim 1), and to identify the components necessary to engage patients to be actively involved in achieving an earlier diagnosis of cancer at the post-presentation stage (Aim 2). By developing a logic model of these components, the authors’ ambition was to guide further research and intervention development in this field.
How this fits in
Patients have a role to play in achieving an earlier diagnosis of cancer, but little is known about how patients can be engaged in monitoring and re-appraising symptoms after an initial presentation to primary care, and before a referral or a diagnosis is obtained. This is reflected in the absence of interventions that involve patients at this stage. Drawing upon current thinking and empirical data, this systematic review identifies potential barriers and facilitators to patient involvement at the post-presentation stage, possible mechanisms of change, and measurable outcomes. The findings have implications for research and practice in the area of patient involvement in achieving an earlier cancer diagnosis in primary care.
METHOD
This systematic review was carried out using the preferred reporting items in systematic reviews and meta-analyses (PRISMA) guidelines.17
Search strategy: Aim 1
Databases were selected to cover both medical and psychological literatures. One researcher, with medical librarian assistance, searched three electronic databases: Ovid MEDLINE (1946 to February 2016), PsycINFO (1806 to February 2016), and Embase (1974 to February 2016). Articles were not restricted by publication type or study design but were limited to the English language. Four blocks of search terms (Appendices 1 and 2) to capture diagnosis (using previously used search terms),18–20 patient involvement, primary health care, and cancer, were combined for the database search. The authors did not search using the specific term ‘safety netting’, a relatively new concept in the diagnosis literature. A recent search using this term found no safety-netting interventions.8 The authors used a broader set of terms in the hope of identifying interventions with characteristics of ‘safety netting’ but which did not make reference to this specific form of intervention. In addition, two researchers hand searched relevant journal articles from 2010 to February 2016 in relevant fields (Appendix 3). Two reviewers independently reviewed the titles and abstracts of retrieved citations, screening half of the abstracts each. Two researchers reviewed 10% of the citations. The full paper was obtained if the inclusion criteria were met, or no abstract was available. Articles were retained or excluded using inclusion and exclusion criteria for Aim 1 (Appendix 4). Together, two reviewers screened all full-text articles obtained (n = 76) to identify those that reported the evaluation of an intervention using any method at the post-presentation stage (Aim 1). At all stages, disagreements on whether to include or exclude an article were resolved through discussion and consensus.
Search strategy: Aim 2
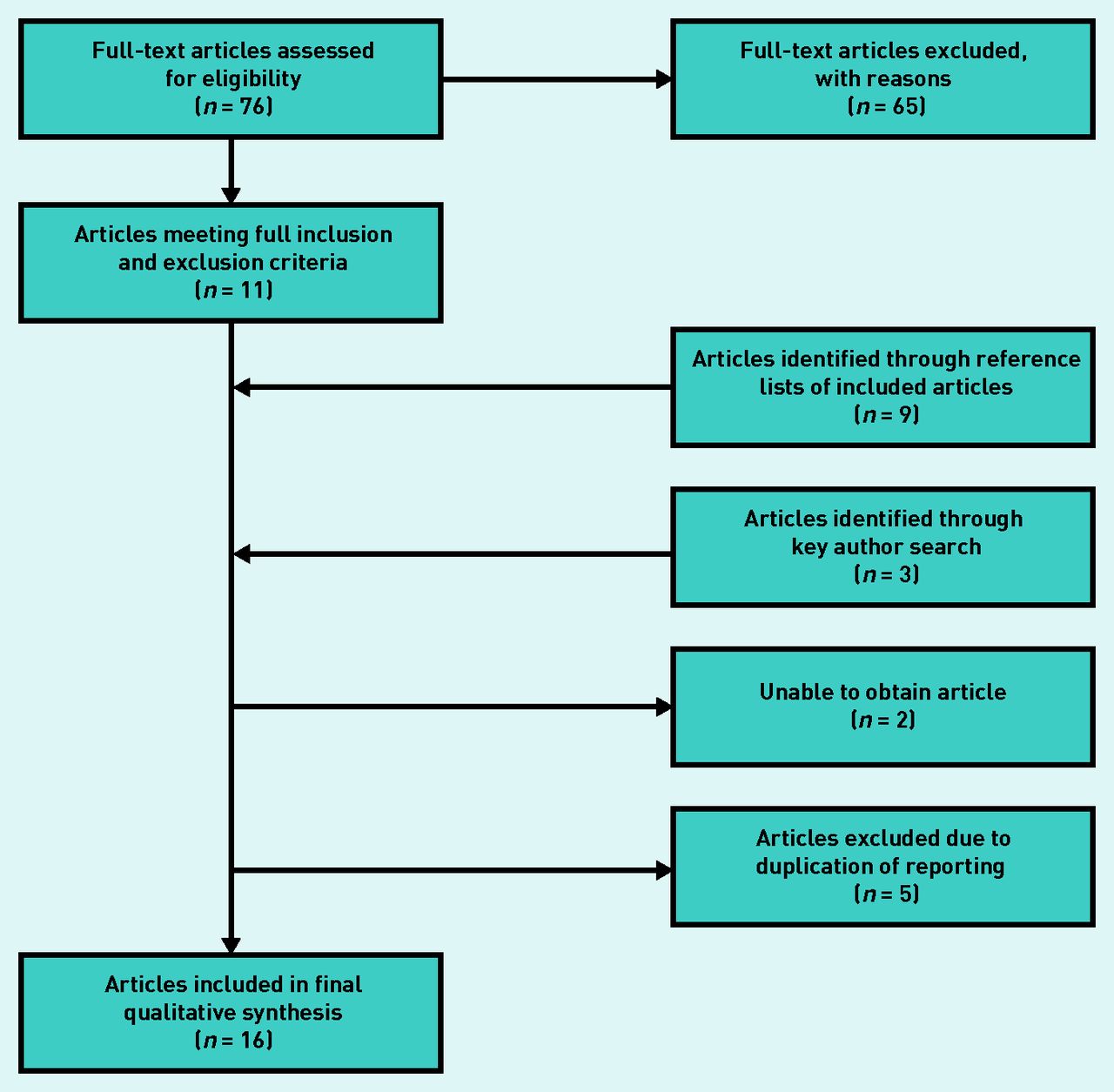
To address Aim 2, two reviewers screened articles that met the original inclusion/exclusion criteria (n = 76). Articles were retained or excluded using inclusion and exclusion criteria for Aim 2 (Appendix 5). An additional secondary strategy involved two researchers manually searching the reference list of all included articles. Publication lists of key researchers in the field were also searched. The decision to include or exclude an article was made through discussion, and a third researcher arbitrated when consensus could not be reached. At this stage, five articles fulfilling the inclusion criteria were removed due to data duplication.21–25 One article6 used some of the data reported in another article.26 However, as the data was analysed to answer different research questions the decision was made to include the article. Two articles could not be retrieved for full article screening.
Data extraction and synthesis: Aim 2
General characteristics data were extracted for each article/study. To identify potential strategies or key components for an intervention at the post-presentation stage, the authors conducted a qualitative synthesis of research findings and current opinion. This facilitated the selection, organisation, and interpretation of nuanced data and thinking from articles with different objectives and which employed a variety of methods. This involved four distinct stages. First, all text relevant to the inclusion criteria in each article was highlighted by one of two researchers and then double-coded by the other researcher. Second, the same two researchers discussed and reviewed the highlighted text and developed a data extraction table (available from the authors upon request) that most meaningfully captured the key categories for all highlighted text and together organised text from each article into each category. Third, the two researchers and one other interrogated the data extraction table and, drawing on a programme theory approach,27,28 began to develop a logic model that illustrated all considerations, possible mechanisms, and outcomes suggested in the articles. Fourth, the logic model was refined to illustrate key considerations, possible mechanisms, and outcomes across the articles.
RESULTS
No published studies met the inclusion criteria for Aim 1 of the review; 16 articles met the inclusion criteria for Aim 2. PRISMA flow charts for Aim 1 and Aim 2 are detailed in Figure 1 and 2.

Flow diagram of search strategy for Aim 1.

Flow diagram of search strategy for Aim 2.
General characteristics of included articles
The general characteristics of the articles included in the systematic review are detailed in Table 1. Four articles were non-empirical,29–32 whereas the majority of articles (n = 12)6,26,33–42 reported empirical findings. Qualitative methods, including interviews (n = 6),34–36,39,41,42 focus groups (n = 2),40,42 and qualitative synthesis of significant event audits (n = 2)6,26 were used in nine studies. Quantitative methods were used in six studies,26,33,37,38,40,42 and included responses to vignettes (n = 1),33 responses to a questionnaire (n = 3),37,38,42 statistical review of incident reports (n = 1),40 and clinical audit (n = 2).26,42 Three articles employed mixed methods using both quantitative and qualitative data.26,40,42 The majority of articles reported studies that were conducted in the UK (n = 9),6,26,33–36,38–40 and one study each was conducted in Denmark,37 the US,41 and New Zealand.42
General characteristics of articles included in systematic review
Though three of the non-empirical articles29–31 and the thematic review40 did not focus on a specific type of cancer, the other articles varied in the type of cancer studied or discussed. Lung cancer was most frequently studied, featuring in eight articles,6,26,33–35,37,39,42 and was the sole focus in two of these articles.34,42 Gastrointestinal (colorectal, colon, rectal, upper GI) was studied in seven articles,6,26,33,35,37,39,41 in one of which it was the sole focus.41 Ovarian cancer was the sole focus of one article,36 and cervical cancer was the sole focus of two articles.32,38 Six articles considered a number of different cancers.6,26,33,35,37,39
The study population in articles varied. Patients only were involved in eight studies,33–36,38,39,41,42 six of which consisted of patients with a diagnosis of cancer35,36,38,39,41,42 and one which involved general patients.33 Two articles included both patients with a diagnosis of cancer and patients suspected of cancer but who had been diagnosed with other conditions.34,42 GPs only were involved in three studies,6,26,37 all of which included patients with a diagnosis of cancer. Both patients, GPs, and/or primary care stakeholders were included in two studies.40,42 And in one article, though patients with cancer and primary care stakeholders were included, it was difficult to establish the exact study population.40
Suggestions for potential interventions/strategies
Though none of the 16 articles directly set out to answer questions about how patients could be involved in the diagnosis of cancer at the post-presentation stage, all articles did consider the patient’s role in diagnostic delay, and identified how they may be involved in the diagnostic process. Articles also considered the contribution of other factors attributable to the healthcare provider (HCP) or system issues. Other than one article that explored referral preferences,33 all articles incorporated findings across a number of diagnostic stages, including pre-initial presentation and/or post-referral factors. As the focus of this review is the post-presentation stage, findings and suggestions that were solely related to other diagnostic stages were disregarded.
Key considerations, possible mechanisms, and outcomes across the articles
The logic model (Figure 3) presents key components and potential mechanisms for involving patients in achieving an earlier diagnosis of cancer and other desirable outcomes.

{kind=link}
{kind=link}
{kind=link}
Logic model — patient involvement in diagnosing cancer in primary care. HCP = healthcare professional.
‘Patients’ and healthcare professionals’ difficulty in identifying potential symptoms’ was identified across most articles, and included distinguishing between symptoms associated with comorbid conditions and new symptoms that may be due to cancer,6,26,29–31,34,36,38–42 and the significance of vague or non-specific symptoms, as well as established ‘red flag’ symptoms.6,26,29–32,34–42 Issues around ‘poor patient–healthcare professional communication during consultation’ were also prominent. These included the healthcare professionals not eliciting a thorough history or asking relevant questions,26,29,36,37,40,41 or the patient’s ability to communicate their health problem.26,29,36,40,41 The emotions of patients were also critical: patients may not re-present due to feeling they were ‘overburdening doctors’ or wasting their time,29,31,38,39,41 or could be influenced by worries and fear concerning tests and potential diagnosis.26,29,31,33,36,38,41,42 The emotional response towards healthcare professionals was also a factor when patients believed that their symptoms and concerns were not being taken seriously or misattributed.31,34–36,39,40
There was a variety of suggestions for strategies to foster patient involvement in the post-presentation stage. Most common was the view that healthcare professionals would benefit from further improvement to their clinical practice. This was primarily around information gathering for diagnosis, such as history taking, physical examination, and record keeping.6,26,29–32,36,37,39 Many articles advocated interventions to involve the patient. The importance of ‘safety netting’ at the end of a consultation was a strong message. It was considered that patients and healthcare professionals agreeing together on a clear symptom follow-up and re-appraisal plan was important.6,26,29–32,34–38,40–42 Some articles discussed having more of an ‘open door’ approach,29,37 and a number also highlighted the importance of setting a timescale for review.6,26,29,30,32,34–36
Many articles also suggested ways for facilitating more open dialogue between the patient and healthcare professional. This included communication about the potential meaning of symptoms and/or the patient’s personal risk31–33,39–41 and healthcare professionals sharing with patients the reasoning behind diagnostic decisions.26,36,37,41 Some articles also stressed the importance of having procedures to ensure continuity of diagnostic information. This involved the patient seeing the same healthcare professional,6,26,30 and improved record keeping to facilitate the linking of previous presentations and/or access to management plans and potential diagnoses, should a patient present to a different healthcare professional.6,26,30,31
Potential moderators of the relationship between suggested strategies and the benefits to patients and health services were identified at three distinct levels. At the patient level, characteristics such as the extent to which patients adhered to the recommendations of the healthcare professional (for example, choosing or not to re-attend to review symptoms)6,26,29,31,37,39,41,42 or patients’ communication skills, such as their ability to express their health problems and concerns,26,29–31,36,41,42 were seen to have an impact on engagement and outcomes. Characteristics of the healthcare professional were also viewed as influencing patient engagement and outcomes, and included the healthcare professional’s experience of cancer to aid recognition.29,31,36,39 There were also a number of moderators at the practice level, which included the impact of consultation length on ability to adequately discuss and address health concerns.29,30,36,42
Both proximal and distal benefits to patients and health services emerged across the articles. Proximal outcomes resulting from proposed strategies include improved monitoring of symptoms6,26,29–32,34–41 and improved quality of the patient–healthcare professional consultation.6,26,29–31,33,35–37,39–41 It is proposed that proximal outcomes such as these may serve as mediators between proposed strategies and distal outcomes, which include reduced diagnostic delay.26,29,32,34–38,40–42
DISCUSSION
Summary
This systematic review did not identify any interventions that involve patients in achieving an earlier diagnosis of cancer at the post-presentation stage and, indeed, none of the articles set out to do this. In general, articles tended to identify and describe barriers and facilitators to achieving an early diagnosis of cancer in primary care, and the role that patients play in diagnostic delay, and provided some general ideas about ways in which patients can assist in this process.
At present, it is unclear whether healthcare professionals and patients sharing responsibility in reviewing symptoms is effective,8 and there is currently no consensus on the practices involved in safety netting,8,13,43 a strategy that is likely to require sustained patient engagement if it is to influence diagnostic outcomes. Based on the authors’ reading of empirical data and current thinking drawn from 16 articles, they identified common components and mechanisms considered to be key to involve patients in diagnosis at the post-presentation stage. This has enabled them to develop and illustrate a first attempt at a logic model for patient involvement in diagnosis in primary care.
Strengths and limitations
There are limitations to this review. Though the authors’ focus was on re-presentation following an initial presentation to primary care, they did not identify any article that focused solely on this aspect in the diagnostic process. To retrieve the information required, the authors had to include articles that incorporated and gathered data from a number of stages in the diagnostic process, and varied in the way diagnostic stages were distinguished. A number of articles also make very general suggestions about patient involvement without expanding on these ideas, or providing any detail concerning what any strategy might include or require. Due to this, gathering data to answer the research questions was a difficult process, and it is possible that information not specific to the diagnostic stage of interest was included. To mitigate this, the authors applied a rigorous and consistent approach to the selection and collation of data using cross-checking and consensus opinion. They also drew upon a variety of articles using different methods to synthesise data to represent an overview of current thinking and findings.
In addition, articles or sections of articles that focused on patients’ symptom perception and help-seeking behaviour were excluded because of these components traditionally being regarded as contributing towards the delay in patients’ initial primary care consultation. One of the articles included in this review39 suggests that symptom perception and help-seeking behaviour before the first presentation may re-emerge and influence decisions and behaviour when a patient re-evaluates their symptoms following an initial presentation. As it is feasible that components identified in this review may operate in a continuum across diagnostic stages (pre-consultation and consultation, as well as post-consultation), it may transpire that findings from work with a focus on the pre-presentation stage, as well as the primary care consultation, are relevant for the development of interventions once the patient has presented. More work in this area is required to establish whether this is the case.
Comparison with existing literature
Though a previous systematic review of patient safety strategies targeted at diagnostic error20 found two studies that focused on patient education, the studies were for breast screening and mothers’ symptom decisions for their child, both of which would not have fitted the criteria for this review. This indicates that there is currently a gap in the evidence base in this field. It also reflects a pattern of a lack of development and evaluation of evidence-based interventions in the field of diagnosis found previously in literature searches conducted for system-related,18 cognitive,19 and safety-netting interventions.8
Implications for research and practice
The findings from this review can be used to guide the direction of future research and intervention development. Though a limited number of qualitative studies assessing the feasibility of safety-netting strategies have been identified and are an important step in understanding how safety netting could be operationalised in practice, there is still no evidence of intervention development in the context of cancer.44 Though this review found some evidence to suggest that ‘active’ (establishing a set time for a further appointment) rather than ‘passive’ (the patient making a further appointment if they feel it is required) safety netting was perceived to be important to ensure the patient returns, further work is required to establish whether one approach rather than the other fosters patient involvement at post-presentation.8,43 In addition, though it is generally agreed that an important dimension in achieving better diagnostic outcomes is engaging patients in the diagnostic process, it is unclear whether patients will welcome such an initiative or what components are important to encourage and sustain patient involvement.45,46 In light of this, this review is timely and progresses the field by identifying barriers and facilitators, possible mechanisms of action, and measurable outcomes when considering patient involvement in achieving an earlier cancer diagnosis in a primary care setting across published articles.
The logic model presented in this review may help to bridge a gap between qualitative findings and quantitative potential through facilitating the testing of hypotheses, and the development and evaluation of evidence-based interventions that are currently lacking in the field of diagnosis.18,19 It also provides an initial testable model that can now be refined through further research.
Acknowledgments
The authors would like to thank reviewers for their comments on an earlier draft of this paper.
Appendix 1. MEDLINE and Embase search terms
|
Appendix 2. PsycINFO search terms
|
Appendix 3. Journal search — field and journal title
| Field | Journal title |
|---|---|
| Diagnosis and decision making | Diagnosis |
| Medical Decision Making | |
| Judgement and Decision Making | |
| Journal of Risk and Uncertainty | |
| Primary health care | Family Practice |
| British Journal of General Practice | |
| Annals of Family Medicine | |
| European Journal of General Practice | |
| Primary Health Care Research and Development | |
| Journal of Primary Care and Community Health | |
| Cancer | British Journal of Cancer |
| International Journal of Cancer | |
| European Journal of Cancer | |
| European Journal of Cancer Care | |
| Cancer | |
| BMC Cancer | |
| Journal of Cancer | |
| Patient Safety | BMJ Quality & Safety |
| Patient Education and Counselling | |
Appendix 4. Aim 1 inclusion and exclusion criteria
Articles were retained if they met all of the following inclusion criteria:
Articles were excluded if:
|
Appendix 5. Aim 2 inclusion and exclusion criteria
Articles were retained if they met all of the following inclusion criteria:
Articles were excluded if:
|
Notes
Funding
This paper presents research funded by Yorkshire and Humber Commissioning Support Research Capability Funding (RCF) (ref. RCF-2015-011) and the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care Yorkshire and Humber (NIHR CLAHRC YH) (ref. 2016-17) (http://clahrc-yh.nihr.ac.uk/). The views expressed are those of the authors, and not necessarily those of the NHS, the NIHR, or the Department of Health.
Ethical approval
Not applicable.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received June 22, 2017.
- Revision requested July 31, 2017.
- Accepted November 2, 2017.
- © British Journal of General Practice 2018
REFERENCES
In this issue









Jump to section
- Top
- Article
- Abstract
- INTRODUCTION
- METHOD
- RESULTS
- DISCUSSION
- Acknowledgments
- Appendix 1. MEDLINE and Embase search terms
- Appendix 2. PsycINFO search terms
- Appendix 3. Journal search — field and journal title
- Appendix 4. Aim 1 inclusion and exclusion criteria
- Appendix 5. Aim 2 inclusion and exclusion criteria
- Notes
- REFERENCES
- Figures & Data
- Info
- eLetters
More in this TOC Section
Related Articles
Cited By...

