


Abstract
Background Statins substantially reduce the risk of cardiovascular disease when taken regularly. Though statins are generally well tolerated, current studies show that one-third of patients discontinue use of statins within 2 years. A qualitative approach may improve the understanding of attitudes and behaviours towards statins, the mechanisms related to discontinuation, and how they are managed in primary care.
Aim To identify factors related to statin discontinuation and approaches for long-term statin adherence.
Design and setting A qualitative study of German GPs’ experiences with statin therapy in rural and urban settings in primary care.
Method Semi-structured interviews (n = 16) with purposefully recruited GPs were recorded, transcribed, and analysed using qualitative content analysis.
Results Sociodemographic patient factors, the nocebo effect, patient attitudes towards primary prevention, and negative media coverage had significant impacts on statin therapy according to GPs. To overcome these barriers, GPs described useful strategies combining patient motivation and education with person-centred care. GPs used computer programs for individual risk–benefit analyses in the context of shared decision making. They encouraged patients with strong concerns or perceived side effects to continue therapy with a modified medication regimen combined with individual therapy goals.
Conclusion GPs should be aware of barriers to statin therapy and useful approaches to overcome them. They could be supported by guideline recommendations that are more closely aligned to primary care as well as comprehensible patient information about lipid-lowering therapy. Future studies, exploring patients’ specific needs and involving them in improving adherence behaviour, are recommended.
INTRODUCTION
The efficacy of statin therapy in the prevention of cardiovascular events in adults with dyslipidaemia is well established.1 However, the use of statins in clinical practice is suboptimal.2,3 In a large meta-analysis of international studies assessing long-term adherence to preventive cardiovascular treatments including the use of statins, adherence was found to be as low as 50% in primary prevention and 66% in secondary prevention.4 Although substantial evidence supports the use of statins in secondary prevention of cardiovascular diseases, where adults aged 40–75 years with established cardiovascular disease should be treated with high-intensity statin therapy,1,5 less evidence is available for primary prevention. The latter applies to patients without cardiovascular disease but with increased cardiovascular risk based on individual evaluation using risk scores.1,6 Statin treatment for primary prevention in adults >75 years remains uncertain owing to sparse research evidence.7 Patients who are more likely to have multiple comorbidities and are undergoing polypharmacy treatment were under-represented in randomised controlled trials. Their long-term adherence to statin therapy is reported to decline substantially over time.8
Poor long-term adherence to statin therapy is associated with higher hospitalisation rates and higher total direct healthcare costs compared with good adherence to therapy over the first 2 years of use.9 In addition, statin discontinuation is associated with an increased risk of cardiovascular events that affects overall mortality, particularly in high-risk patients.10,11 Though deemed safe and well tolerated, statins have been associated with side effects, especially at high doses, such as muscle symptoms, new-onset diabetes mellitus, central nervous system-related, and hepatic side effects.12 However, side effects are not the only reason for statin discontinuation as inferred from the low rate of long-term adherence; the reported incidence of side effects among statin users is 5–10% in randomised clinical trials and 10–30% in observational studies.13
The latter might be due to symptoms perceived by the patient that are not statin related but still contribute to the higher frequency of side effects observed in clinical practice. In this respect, both treatment- and non-treatment-related factors, including patients’ characteristics, could contribute to statin discontinuation. Previous studies exploring attitudes towards statin side effects and reasons for statin discontinuation, from the perspectives of both patients14–17 and physicians,18,19 identified several subjective and potentially modifiable factors that could be utilised to improve the long-term adherence to statin therapy. These factors include, but are not limited to, intake of multiple drugs per day (polypharmacy), misunderstanding of treatment benefits, misconception of hypercholesterolaemia as a disease that requires treatment, physician–patient miscommunication, and concerns about side effects. Accordingly, these factors need to be addressed to improve the long-term adherence to statin therapy.
How this fits in
Medication adherence is needed to achieve the full effect of statins in secondary as well as in primary preventive care. Though side effects caused by statins affect only a minority of patients, current studies indicate that approximately one-third of patients discontinue the use of statins within 2 years. This study identified factors leading to statin discontinuation in primary care from the GP’s perspective. Primary care professionals reported multifaceted barriers to long-term adherence to statin therapy and implemented strategies to improve adherence in order to provide the best possible patient outcomes.
GPs represent the healthcare professionals likely to be involved in the initial discussion of statin therapy with patients,20 and in the management of long-term medication. For that reason, a qualitative approach to the proponents of primary care may be useful to identify barriers as well as working strategies for statin therapy. This can contribute to the development and implementation of interventions that enhance therapy adherence and ultimately patient outcomes.
METHOD
This research is an independent qualitative study on German GPs’ experiences with statin therapy. Sixteen interviews with GPs were conducted between April 2016 and July 2016 by three different researchers with varied academic and clinical backgrounds (general medicine, pharmacology, and pharmacy). Physicians with a specialisation in general medicine, who worked in a primary care sector as an employee or a practice owner, were selected from both the Research Network of the Berlin Institute of General Practice Charité (ANCHOR) and from other independent GP practices in Berlin and Brandenburg. Purposive sampling was employed at this stage to ensure that the sample represented a maximum variation of diverse characteristics such as sex, practice type, size, and grade of urbanisation, including the socioeconomic profile of the patients. In a further step, the sample was carefully selected to make sure there were no personal relationships between the interviewer and the interviewed GP. After contacting the GPs with a sufficient variety in characteristics via an email invitation, 16 GPs agreed to take part. The interviews were based on an interview guide formulated by the authors and based on literature and expert opinions.21 The semi-structured interviews were conducted face to face at the GPs’ practices and lasted 20–45 minutes; details of the interview questions are available from authors on request. The interviews were recorded and transcribed verbatim. The transcripts were encoded and analysed by the interviewers using qualitative content analysis, according to Mayring,22 who describes an approach of systematic, rule-guided, qualitative text analysis. Two procedures are central: the inductive category development and the deductive category application approach to identify, analyse, and report patterns in the data. Categories were carefully synthesised from both the initial ideas and material, and revised within the process of analysis. First, a preliminary coding scheme was developed and tested by the three researchers coding independently. Points of difference were discussed and revisions were made until a common approach was agreed. Subsequently, all data were coded and used until the final stage, in which some items deemed irrelevant to the research question were not included. This process formed the structure of the results; quotations were used to explicate the subjects. The original German quotations were translated into English.
RESULTS
This study was based on 16 interviews with GPs. The demographics of the participants show variability in sex, additional specialisation, degree of urbanisation, and practice type (Table 1).
Characteristics of participating GPs
Generally, there was an overwhelming agreement among GPs that long-term therapy with statins is unsatisfactory. GPs indicated that they encounter several challenges when discussing statin therapy in daily practice. They attributed statin discontinuation mainly to the patients. Nevertheless, they pointed out that attitudes and behaviours on both sides, patients and doctors, could lead to the frequent failure of long-term statin therapy. However, most of the GPs were convinced that confidence in doctors and a stable doctor–patient relationship were strongly associated with patients’ adherence to statin treatment. Consequently, they emphasised ways to manage these challenges and motivate patients to therapy through communication skills and person-centred care. The latter focuses on the dynamics of patient–physician communication and is guided by patients’ values and preferences to achieve satisfaction with their care.23 This study aimed to extract issues specific to statins as described below:
Patient characteristics
GPs perceived that patients’ sociodemographic status influenced the long-term therapy with statins. They implied that a low educational level and older age posed a high risk for statin discontinuation. Though these groups of patients prefer to follow the GPs’ advice at first, they tend to miss GP appointments to get a new prescription, or fill it at the pharmacy. They also tend to forget the evening intake, according to GPs:
‘I guess that people with a lower educational level have difficulties in taking a therapy on a regular basis, to understand at all what might happen to them in the future …’
(GP5, male [M])
‘Most of our patients are not highly educated; they do not decline the therapy or have any concerns, they rather forget to take the statins.’
(GP15, female [F])
On the other hand, GPs emphasised that patients with a higher educational level could also be particularly challenging. This resulted from scepticism about medications, evidence from clinical trials, as well as the expertise of GPs. A few even conceded that they felt uncomfortable or stressed out around this group of patients. According to GPs, these patients are excessively concerned about developing muscle symptoms that could affect their quality of life or they question the necessity of further therapy after reaching low-density lipoprotein-cholesterol (LDL-C) standard values:
‘Many patients, especially those with a higher educational level, are concerned about side effects …“I will not be able to ride the bicycle any more because I will get muscular pain”, that is how they react. I get that a lot.’
(GP10, F)
The nocebo effect
The nocebo effect is a detrimental effect on health produced by psychological or psychosomatic factors such as negative expectations of treatment or prognosis.24 Most of the participants suspected that a significant part of perceived symptoms from statins resulted from the nocebo effect.
They observed that patients with psychiatric comorbidities such as anxiety and depression were more prone to the nocebo effect:
‘Anxious patients with a tendency to hypochondria often develop perceived side effects.’
(GP9, F)
GPs feared that talking about side effects could lead to poor adherence. As a result, this group of patients were not comprehensively informed about side effects and were less frequently asked about complaints. Some GPs reported that they completely avoid talking about statins with anxious patients:
‘To prescribe a statin and point out to pay attention to side effects … is not a good start.’
(GP11, M)
At the same time, almost all GPs were convinced that less informed patients were more prone to influences from the media and non-expert opinions, which might adversely affect doctor–patient relationships and adherence to statin therapy.
They perceived this situation as a dilemma.
The impact of media coverage
More than half of GPs supposed that recent media coverage of statins had a negative impact on patients and contributed to patient concerns about statins and discontinuation of statin therapy.
They stated that media-influenced patients tended to express critical views about side effects and the need for lipid-lowering therapies in general:
‘When statins are critically discussed in the media, more patients raise doubts about statin therapy and refer to that media source.’
(GP16, M)
The participants emphasised that media coverage mainly affected patients with lower cardiovascular risk levels or those with no history of cardiovascular disease.
Perspectives and attitudes towards primary prevention
Most of the GPs considered the relevance of statin therapy to be low, particularly in primary prevention. Some questioned the guidelines and were unconvinced of the evidence for the efficacy of statins in low-risk patients:
‘I have second thoughts concerning the primary prevention; I am unconvinced of the data situation. If I recommend statins, it has to make sense for me.’
(GP4, F)
A few GPs were concerned that statins in primary prevention were used as a substitute for lifestyle change and for that reason were more likely to follow a patient’s request to stop primary prevention with statins.
A number of GPs were keen to omit statin therapy first in older patients receiving polypharmacy in order to reduce pill burden, regardless of whether statins were prescribed for primary or secondary prevention.
Approaches to improving long-term therapy
In addition, the researchers explored approaches and actions undertaken by GPs to improve long-term therapy with statins. The main themes that emerged were patient education, person-centred care, and patient motivation (Figure 1).
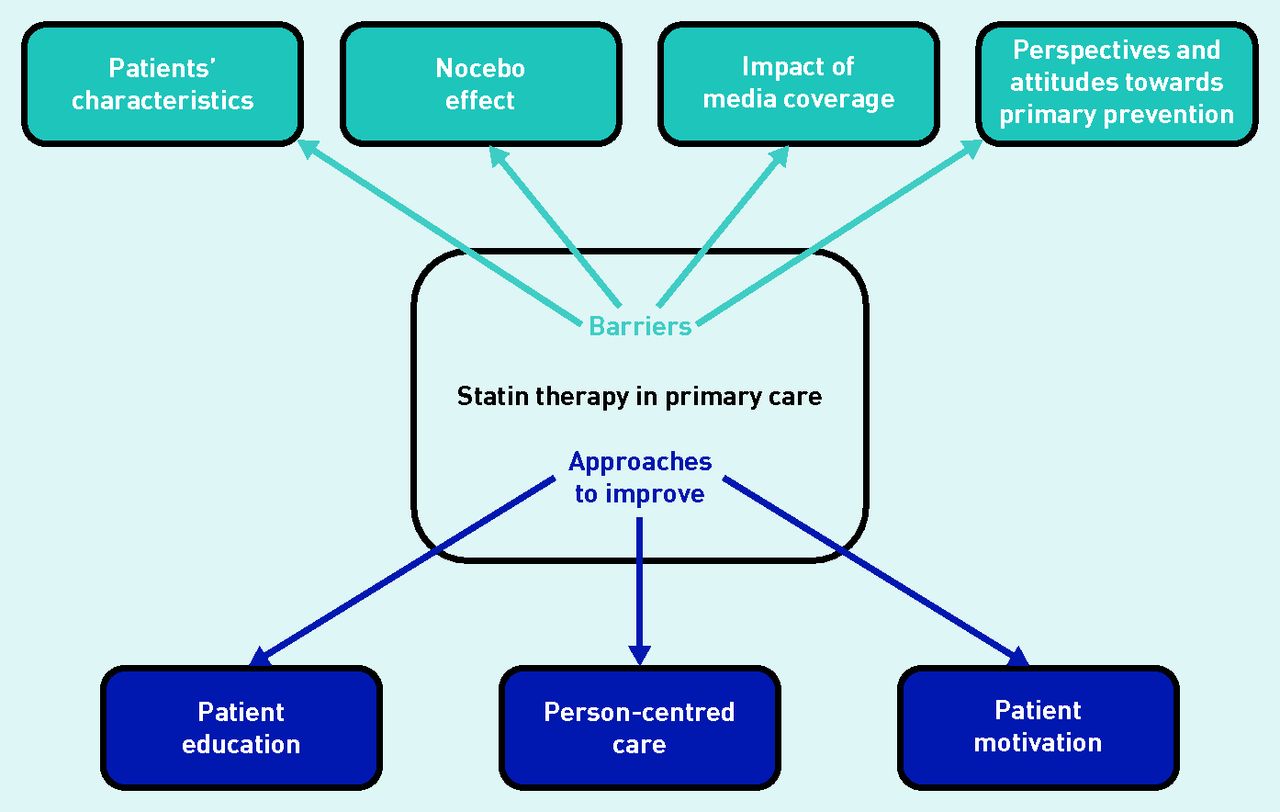
{kind=link}
Main barriers in statin therapy and approaches to improve adherence according to GPs.
There was strong agreement among GPs that ongoing patient motivation was needed in statin therapy. They remarked that both the prevention of a discontinuation as well as its management required communication skills and expertise in patient education:
‘Usually, you have to motivate patients to statins because hypercholesterolaemia does not cause any discomfort … Yes, you have a great deal to do to motivate patients.’
(GP9, F)
‘For example, if the patient mentions that he doesn’t want the medication, he has concerns, or he is afraid to take it, we discuss jointly his situation and also his individual risk profile. If the patient finally decides against the statin, this is acceptable to me … This is how it works! At the very end, the patients decide …’
(GP5, M)
The majority of the GPs used computer programs to calculate and visualise the benefits of a cholesterol-lowering therapy. Generally, German GPs prefer two risk profile calculators, the PROCAM risk calculator, based on the results of a large epidemiological study on the German population (Prospective Cardiovascular Münster Study) and the ARRIBA risk calculator, based on the Framingham score. Owing to the different illustrations of risk profiles (charts or smileys), most of the GPs installed both programs and utilised them depending on the patients’ educational level. This forms the basis, according to GPs, for a shared decision-making process concerning the therapy regimen:
‘I find it easy to work with a computer program, to discuss the risk profile together, that’s a good motivation for patients.’
(GP14, F)
‘It depends on the intellectual abilities of the patients if I use the PROCAM program or show the patients the “risk profile smileys” on the ARRIBA program.’
(GP5, M)
GPs emphasised the importance of educating patients about the potential interaction of both specific lifestyle changes and statin therapy on cholesterol levels, as well as the limited impact of lifestyle changes alone, for achieving target LDL-C levels. Furthermore, a couple of participants provided patients with printed therapy plans to take with them as well as advice on the evening intake at the time of their first prescription.
A few GPs had a good experience with the frequent monitoring of LDL-C levels or checking prescription refill records to assess statin intake and to address patients with adherence problems specifically. Most of the GPs prioritised a stable, long-term therapeutic relationship over the achievement of LDL-C targets or following the guideline recommendations. They suggested a person-centred approach to overcome concerns and resistance or manage perceived side effects:
‘It’s essential to take patients’ concerns and physical complaints seriously, even if you were convinced that they were not caused by statins … It’s important to omit the statin first. The patients experience physically that the back pain hasn’t gone away and wasn’t caused by the statin.’
(GP15, F)
In addition, most of the GPs switched to another statin after temporary discontinuation instead of returning to their original medication, for psychological reasons:
‘Re-exposure is almost never successful, usually causes the same complaints. That’s why I always switch the statin, these patients are more likely to continue the medication.’
(GP1, F)
There was a strong agreement among GPs that long-term adherence to statins can be improved by being aware of barriers and combining the individual approaches, supports (such as technical tools), and guideline recommendations with questions about the patient’s personal situation.
DISCUSSION
Summary
The present study offers some insights into GPs’ expectations of why long-term adherence to statins is deficient and how they handle this issue in daily routine care. Almost all of the GPs had experiences of challenging patient conversations about statin therapy. They observed different types of resistance in patients, mostly depending on sociodemographic factors. A low educational level and an older age could be, for different reasons, a predictor for poor long-term adherence to statins, according to GPs. In addition, they considered that the recent media coverage of lipid-lowering therapy had a negative impact on patients’ adherence. Attitudes and doubts about the appropriateness of statin use in low-risk patients were perceived to be important barriers affecting both the patients’ adherence and the doctors’ prescribing behaviour. They suspected that exaggerated concerns about statins, particularly in patients with psychiatric comorbidities, such as anxiety and depression, led to a nocebo effect and ended in statin discontinuation.
GPs described various approaches to manage these barriers. They attached great importance to connecting patient education and motivation with person-centred care. For example, individual risk assessment with different computer programs were combined with a shared decision-making process to reach patients of all educational levels. Further approaches to assess and improve adherence such as monitoring of LDL-C levels, checking prescription refill records, printed therapy plans, advice for the evening intake, or switching the statin for psychological reasons were considered helpful.
Strengths and limitations
The intent of this qualitative study was to understand the range of perspectives and individual views that GPs hold in relation to statins and to add to the knowledge about factors that may affect adherence with statin treatment. Though limited in their generalisability, qualitative research can point to specific patterns and typologies. However, it is not possible to identify causal links to all of the findings in this study and draw a single conclusion or response to the several barriers associated with statin treatment.
Though a relatively low total number of 16 interviews were conducted in the present study, the meaningfulness of the results is supported by the saturation of content noticeable in the progression of the interviews. Being interviewed by another physician may have influenced the results and might not always represent a GP’s actual behaviour. Another limitation concerns the sampling process: the sampling was restricted to two federal states in Germany and most of the interviewed GPs were working in urban settings. Nevertheless, this study achieved a well-balanced sample concerning characteristics like sex, type of practice, and specialisation. Because GPs had to agree to be interviewed, a sampling bias of very interested and motivated GPs cannot be excluded. In addition, there was no patient involvement so the study only shows the GP’s perspective.
Comparison with existing literature
According to the participating GPs, statin discontinuation was mostly initiated by patients, which concurs with the existing literature.19 Though statins were often discontinued without a prior medical consultation, physicians still play a crucial role in improving adherence and avoiding discontinuation, as highlighted by several studies.25–28 Patient adherence to therapy can be influenced by physicians in several ways; overall, compliance of GPs with cholesterol management guidelines, which recommend regular follow-up of patients, improves patients’ adherence to statin therapy.28 In addition, the lack of adequate information about the disease provided by the GPs, as well as the benefits and potential side effects of statins are strong contributors to non-adherence.29,30 The importance of the physician–patient relationship in adherence was repeatedly expressed by GPs in the present study. A previous survey indicated that patients who were taking statins had more confidence in their latest interaction with a GP than those who had stopped or never taken statins.20 The interviewed GPs were more inclined to involve the patients in decision making and to take responsibility for their own treatment choices; however, they emphasised encountering several barriers. For example, they were concerned that the nocebo effect significantly influenced patients’ compliance. The nocebo effect is a well-established phenomenon in pharmacotherapy and refers to side effects subjectively perceived from drug therapy due to prior expectation.24 It has been indicated that the nocebo effect is one reason for the high rate of side effects, especially muscle symptoms attributed to statins in observational studies and clinical practice.31 The nocebo effect seemed to affect both the patients and the GPs. Some GPs conceded that they should be more cautious when educating about statin side effects, fearing this could lead to poor adherence. A study conducted in patients discontinuing their statin therapy concluded that being less informed and unconvinced about the treatment were among the most common reasons for statin discontinuation.32
There is much less agreement among physicians about statins in primary prevention than in secondary prevention,20 which was also expressed by the interviewed GPs. A few participants considered the overall relevance of statins in cardiovascular primary prevention. This group tended to stop statins in case of any physical discomforts, polypharmacy, or at a patient’s request.
Furthermore, GPs observed that negative information about statins promoted by media coverage led to concerns and discontinuation of statin treatment in patients. Various studies have shown that discontinuation of statin therapy was temporarily influenced by negative media coverage.33–36 The present interviews emphasised that barriers to statin therapy depended on demographic characteristics, especially socioeconomic status and educational level. These seemed to be important predictors of adherence to statins according to GPs. Patients with higher socioeconomic status and higher education showed a greater level of long-term statin adherence,25,37 which was also noticed by the majority of GPs.
In order to motivate patients to therapy and lifestyle changes, most of the GPs used computer programs with graphic presentations of individual risk profiles and benefits of therapy, for example, the ARRIBA38 and PROCAM tools,39 to actively involve patients in healthcare decision making. Several studies indicate that motivational strategies combining patient education, follow-up and monitoring with computer programs led to a lower rate of discontinuation.27 International guidelines, for example, the guidelines of the National Institute for Health and Care Excellence (NICE), emphasise shared decision making in the prevention of cardiovascular disease and contain recommendations to involve patients in decisions about their medication therapy.40
Implications for research and practice
Shared decision making supported by computer-assisted programs seems to be a successful strategy to motivate patients and might serve as a valuable tool in primary care to promote patients’ adherence. There is a need for implementing more comprehensible and interactive information about the risk of cardiovascular diseases and risks associated with statin therapy to educate patients. Information leaflets and software applications for lipid-lowering therapy, a healthy lifestyle, evening intake, and clear instructions in case of side effects could be helpful. Switching to statins that could be taken in the morning, for example, newer statins with a longer half-life should be considered if the evening intake is regularly forgotten, and when higher costs do not limit this approach.
Practice guidelines with recommendations that are closer to management of patients in daily routine would be supportive for GPs. This can be achieved by incorporating reference case studies in guidelines describing alternative proceedings, such as deviations from LDL-C target values, intermittent dosing therapy, and statins in a polypharmacy situation.
Qualitative studies to explore patients’ perspectives are needed to reveal further barriers to long-term therapy with statins, particularly the nocebo effect, focusing on the impact of media coverage on patients. Quantitative studies to investigate the efficacy of approaches and strategies employed by GPs for improving adherence to statin therapy are also important areas for future research.
Acknowledgments
The authors wish to acknowledge the help and support of the participants who were interviewed. The authors are immensely grateful to Thomas Riemer for assistance with the language editing and proofreading of the manuscript.
Notes
Funding
This research received no specific grant from any funding agency in public, commercial, or non-profit sectors.
Ethical approval
Interviewing healthcare professionals required an approval of the responsible ethics committee according to the German legislation. Ethical approval for the study was provided by the ethics committee of the Charité — Universitätsmedizin Berlin, Germany (EA2/017/17).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received July 25, 2017.
- Revision requested October 26, 2017.
- Accepted January 2, 2018.
- © British Journal of General Practice 2018
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

