


Abstract
Background Statins are effective in preventing cardiovascular disease (CVD) events and are recommended for at-risk individuals but estimated adherence rates are low.
Aim To describe patients’ perspectives, experiences, and attitudes towards taking statins.
Design and setting Systematic review of qualitative studies reporting perspectives of patients on statins.
Method PsycINFO, CINAHL, Embase, MEDLINE, and PhD dissertations from inception to 6 October 2016 were searched for qualitative studies on adult patients’ perspectives on statins. All text and participant quotations were extracted from each article and analysed by thematic synthesis.
Results Thirty-two studies involving 888 participants aged 22–93 years across eight countries were included. Seven themes were identified: confidence in prevention (trust in efficacy, minimising long-term catastrophic CVD, taking control, easing anxiety about high cholesterol); routinising into daily life; questioning utility (imperceptible benefits, uncertainties about pharmacological mechanisms); medical distrust (scepticism about overprescribing, pressure to start therapy); threatening health (competing priorities and risks, debilitating side effects, toxicity to body); signifying sickness (fear of perpetual dependence, losing the battle); and financial strain.
Conclusion An expectation that statins could prevent CVD and being able to integrate the statin regimen in daily life facilitated acceptance of statins among patients. However, avoiding the ‘sick’ identity and prolonged dependence on medications, uncertainties about the pharmacological mechanisms, risks to health, side effects, costs, and scepticism about clinicians’ motives for prescribing statins were barriers to uptake. Shared decision making that addresses the risks, reasons for prescribing, patient priorities, and implementing strategies to minimise lifestyle intrusion and manage side effects may improve patient satisfaction and continuation of statins.
INTRODUCTION
Cardiovascular disease (CVD) is responsible for more than 30% of deaths worldwide and prevention is a public health priority.1–3 Elevated low-density lipoprotein (LDL) cholesterol is a major risk factor of CVD,4,5 and affects more than half the adult population in countries including the US and UK.3,6 HMG-CoA reductase inhibitors (statins) are effective in improving lipid profiles and reducing the risk of CVD events.7,8 Although the relative risk reductions from statins are relatively consistent — around a 22% reduction in major vascular events per 1 mmol/L reduction in LDL cholesterol — the balance of risks and benefits of statins, and their cost-effectiveness, depends largely on an individual’s absolute risk of a future cardiovascular event.7,8 Hence, the recommendation that statins be offered to individuals at high risk of future CVD, including those with existing CVD and those with risk factors conferring high risk, is well established. Increasingly, statins are also recommended for primary prevention of CVD in those at more moderate levels of absolute risk, on the basis of effectiveness and cost-effectiveness, such that the proportion of adults for whom statins should be recommended is projected to exceed 40% in the UK and US.1,9 However, concerns have been raised about the medicalisation of the population and diminishing potential benefits to individuals, particularly for those who are at low absolute risk of CVD events.
Mortality from CVD has fallen by over 75% in the last 40 years in many industrialised countries, with statin use likely to be a contributing factor.10,11 However, data indicate that the majority of individuals in whom statins are indicated are not using them, including individuals with existing CVD and those at high primary risk.12 Currently, adherence rates after 2 years for statins are estimated to be 57% for primary CVD prevention and 76% for secondary prevention.13 Whether or not to use statins is a decision for each individual patient in partnership with their health professionals, and there are likely to be multiple reasons for the differential between recommendations and use, including practitioner, health system, and patient factors.
A systematic review of qualitative studies on patient perspectives on statins for CVD prevention across healthcare contexts and populations can generate broad and in-depth insights into values, knowledge, and beliefs that influence their behaviours and decisions regarding statin use. This review aims to provide a comprehensive synthesis of patient perspectives to inform shared decision making, strategies, and interventions targeted at improving the use of statins, and ultimately treatment satisfaction and outcomes.
How this fits in
Statins are effective in preventing cardiovascular disease (CVD) events and are recommended for at-risk individuals. Adherence rates are around 57% for primary and 76% for secondary prevention. This study adds to previous knowledge by consolidating and building on current barriers to uptake and continuation of statins such as side effects, uncertainties about the benefits, lifestyle intrusion, costs, fear of additional harms to health, avoiding the ‘sick’ identity, and scepticism about clinicians’ motivations for prescribing statins. Transparent and informed shared decision making that addresses the risks and benefits, reasons for prescribing statins, strategies for managing the statin regimen, and patient goals may improve patient satisfaction and improve continuation of statins in patients at high risk of CVD.
METHOD
The Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) framework was followed in this study.14 Searches in MEDLINE, Embase, PsycINFO, and CINAHL were conducted from inception to 6 October 2016. Google Scholar and reference lists of relevant studies and reviews were also searched. PhD dissertations were searched in ProQuest Dissertations and Theses database, British Library Electronic Digital Thesis Online Service (EThOS), and the Europe E-theses Portal. One author screened the search results by title and abstract, and excluded those that did not meet the inclusion criteria. Full texts of potentially relevant articles were assessed for eligibility (details of search strategies are available from the authors on request). Qualitative studies that reported patients’ perspectives on statins were included. Studies involving adult patients at risk of CVD, and patients receiving statins as primary or secondary preventive therapy for CVD, were eligible. Articles that only included patients with familial hypercholesterolaemia (as this is a specific genetic condition) or perspectives from health professionals were excluded, as well as studies that used structured surveys and reported only quantitative data, or were epidemiological studies, reviews, or editorials. Non-English articles were excluded due to limited resources for translation.
Data extraction and quality assessment
All the text and participant quotations from the Results or Discussion/Conclusion sections were extracted for each article, and entered verbatim into HyperRESEARCH (version 3.0.3) to code textual data. Two authors independently assessed the transparency of reporting using the Consolidated Criteria for Reporting Qualitative Research (COREQ),15 which includes criteria specific to the research team, study methods, context, analysis, and interpretations. Any discrepancies were resolved by discussion among the reviewers.
Data synthesis and analyses
Using thematic synthesis,16 one researcher coded the data line by line, and inductively identified preliminary concepts that described patients’ perspectives on statins. Similar concepts were grouped into themes and sub-themes. Two other researchers, who had also read all of the articles, discussed the themes to ensure that the coding framework and themes captured the full range and depth of data reported in the primary studies. Any patterns and conceptual links among themes were mapped in a thematic schema.
A systematic review registration was not applicable for this study.
RESULTS
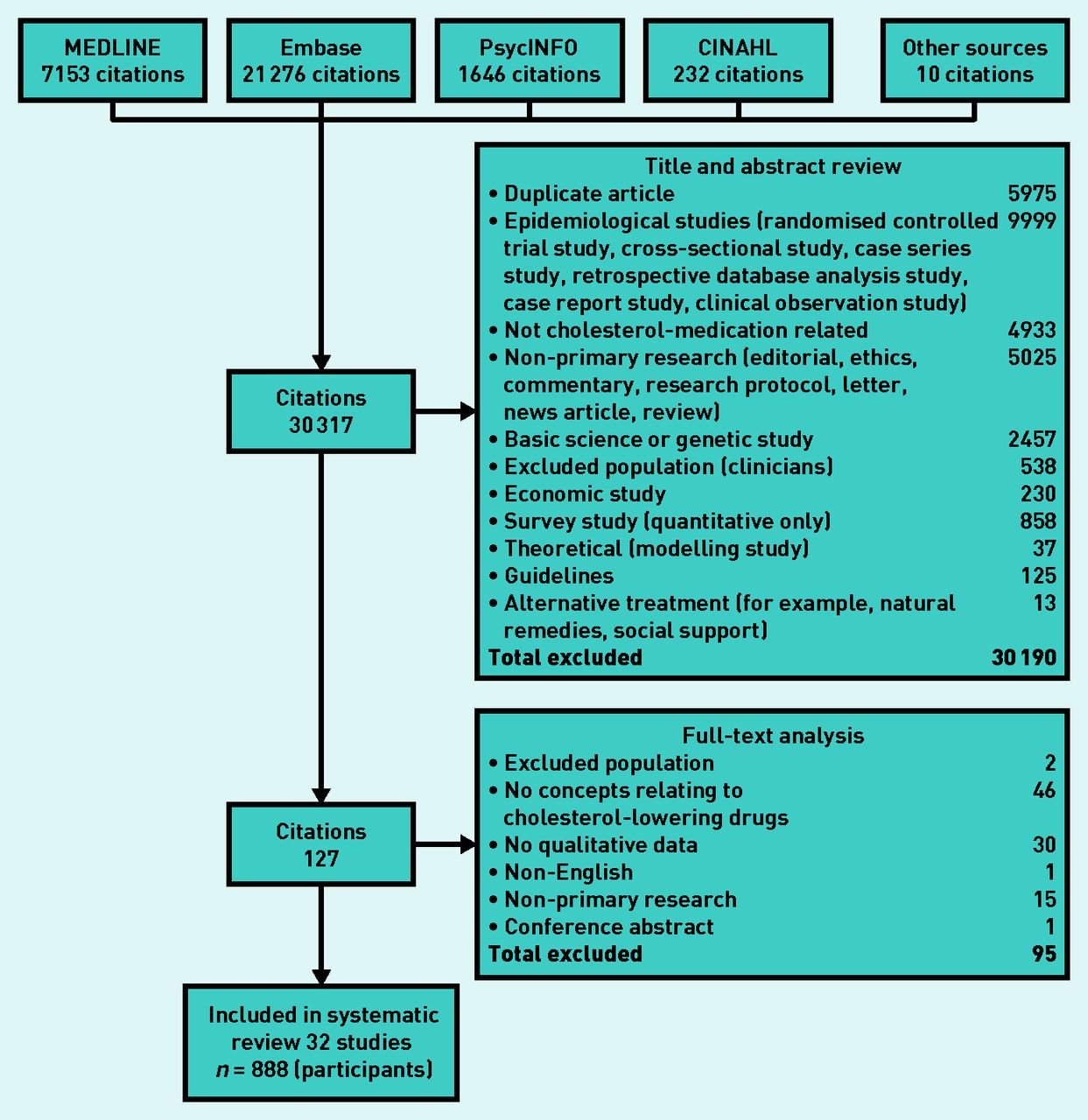
From 30 317 citations retrieved in the search, 32 studies were included involving 888 participants. Details of the search results can be found in Figure 1. In the 22 studies that reported the use of statins, at least 364 participants had previously or were currently taking statins. Of the 22 studies that specified the type of CVD prevention, 15 studies included at least 275 patients eligible for primary prevention and 11 studies included at least 165 patients receiving secondary prevention therapy. Twelve studies included both primary and secondary prevention patient groups. Across all the studies, at least 41% of the patients were taking or had taken statins (eight studies did not specify the number of patients on statins). The studies were conducted across eight countries with the majority in the US and UK. Data were collected using interviews, focus groups, and open-ended surveys. The study characteristics are summarised in Table 1.

Search results.
Characteristics of included studies
Comprehensiveness of reporting
Comprehensiveness of reporting was variable, with studies reporting 5–18 out of the 27 possible items included in the COREQ framework. Although all studies described the participant characteristics, the participant selection strategy was reported in 28 (88%) studies. Researcher triangulation (multiple investigators involved in data coding and analysis) was stated in 22 (69%) studies. Fourteen studies (44%) reported theoretical saturation. The two studies conducted with non-English-speaking participants reported the language in which the data were collected and analysed (details of comprehensiveness of reporting in included studies are available from the authors on request).
Synthesis
Seven themes were identified: confidence in prevention, routinising into daily life, questioning utility, medical distrust, threatening health, signifying sickness, and financial strain. The respective sub-themes are described in the following section. The themes pertain to both primary and secondary prevention of CVD unless otherwise specified. Illustrative quotations for each theme are provided in Box 1. The conceptual links among themes are presented in Figure 2.
Illustrative quotations
| Theme | Quotations | Sources |
|---|---|---|
| Confidence in prevention | ||
| Trust in efficacy | ‘I feel good about it because the medication’s working, and so I feel like I’m gonna be healthier because of the medication.’ (F65) ‘I’m on two cholesterol medicines. My bad cholesterol was 110 and that’s down to 48. My good was 35 and now it’s up to 78.’ (F60) ‘Whew! It’s like, gee, take medicine and see how quickly it changes those numbers.’ (F60) ‘I would say what comes to my mind first is that it’s amazing that … or able to take something that has effects. I feel lucky that I’m able to do that.‘ (M62) | 17,21,31,45,51,53,57 |
| Minimising long-term catastrophic CVD | ‘I feel like it’s a good time to be looking into this because it’s going to be preventative for the future.’ (M27) ‘Something to take now, to help you for the future.’ (M≥18) | 17–21,31,45,50 |
| Taking control | ‘I realise that, you know, I have some control there. So, that’s hopeful.’ (M45) ‘Reassuring … It’s just a kind of comforting. Just knowing what I’m doing, probably better for me.’ (M59) | 17,21,45 |
| Easing anxiety about high cholesterol | ‘I think it gives me a peace of mind … my general concern about my health is decreased because of the fact that I take the medication that ultimately is very effective regulating cholesterol level.’ (M62) ‘I guess I don’t worry much about it, because of the drugs I am taking.’ (F64) | 17,45 |
| Routinising into daily life | ‘It’s the same routine I get up, and go through sort of early morning routine, shave, make my coffee, and take my medication same time, pretty much every morning.’ (M58) ‘Initially, I was prescribed to cut the tablet in half, and for some reason that just became so inconvenient, I would just put it off and just never took it.’ (U≥18) | 17,21–25,27,30,31,46 |
| Questioning utility | ||
| Imperceptible benefits | ‘I don’t find any difference, but, erm, because they say that my cholesterol level is slightly higher that it should have been I think, if I don’t take it, I don’t find any difference.’ (F69) ‘I certainly don’t feel anything. So, the only proof comes empirically through the follow-up with my doctor.’ (M46) ‘To be quite honest with you, I don’t even know if I should be taking any of them. I feel all-right.’ (M≥18) | 17,19,23,24,31,47,50,51 |
| Uncertainties about pharmacological mechanisms | ‘I don’t know what it is. I don’t know where it comes from. I don’t know where it goes.’ (U) ‘I’ll be honest with you, I wouldn’t retain all that [information] … because of our limitations of our education with tablets and things … we only have so much knowledge of tablets you know. Like take it, it’s as simple as that, that’s about as much as we want to know really about a tablet … ‘ (U) ‘I didn’t really like taking [lovastatin] because I had heard some negative things about it before. It was hard on your system in some ways … It wasn’t good to take a lot of it for a long time. I can’t remember specifics; I just heard that it was kind of a powerful thing and better not to take it if you can avoid it.’ (U) | 23,25–28,30,47,48,50,51,56 |
| Medical distrust | ||
| Scepticism about overprescribing | ‘Because of the lowering [recommended cholesterol levels], GPs are being advised to put [more] people on the tablets.’ (M≥18) ‘And I thought well things change by the week you know, next week it might be something else.’ (M≥18) ‘I feel sometimes people just say, “well that’s what you’ve got so there’s this tablet”.’ (F≥18) Statins were, in the eyes of participants, now being offered regardless of cholesterol levels or whether an individual’s cholesterol was inside or outside the current recommended thresholds. | 18–20 |
| Pressure to start therapy | ‘Well, he wanted me to start it when I went to see him. Every single time for the last … 2 or 3 years. Until I gave in … I don’t remember [what he said] apart from him threatening me … saying that I could risk getting a blood clot too.’ (M27) | 29 |
| Threatening health | ||
| Competing priorities and risks | ‘I won’t go on the medication because my husband and I are going to try to have children and you can’t get on that medication if you want to try to have kids. So, I’m kind of a ticking time bomb right now.’ (F≥18) ‘I went on cholesterol medication and I was on that for 2 years until I got muscle weakness and actually crashed my car into other cars twice in 1 week.’ (F≥18) ‘And I knew it was because — and then when I realised it was because of [my medication], I stopped taking it immediately and told my doctor I’d rather die of a heart attack than die in a car accident.’ (F≥18) | 17,21,29 |
| Debilitating side effects | ‘It’s brutal … At the moment, I’m tired and I tend to blame it on this very strong medication.’ (U≥18) ‘I have problems taking that medication for the other cholesterol, Crestor®; I took it several different times and I noticed side effects, you know, where I think it affected my heart … I can’t tolerate the Crestor … if something affects me a whole lot or puts pain on me or affects my heart, then I don’t think I should take it. I am thinking of doing an experiment of not taking it for 1 or 2 weeks. And then I would see during the 1 or 2 weeks if my pain gets better, then I will know for sure it’s a statin.’ (M46) ‘I can take Zetia®, but not statins. My muscles turn to jelly. Every join in my body aches.’ (F85) | 17–21, 23, 27–29, 31, 33, 48, 49, 52–54, 57, 59 |
| Toxicity to body | ‘I don’t want a load of trash in me. I’m a natural kind of guy! […] well, it has to be absolutely necessary. Because, as I said before, I won’t take medication to prevent disease. I’d rather have another herring.’ (M65) ‘Well I’m introducing some chemical and I don’t know what the side effects of it are.’ (M61–70) ‘If you could get a cholesterol drug that didn’t degrade the muscles and didn’t endanger my kidneys or my liver, I think I would take it in a second.’ (F≥18) | 21, 23, 25, 27, 29, 31, 33,51, 52, 55, 59 |
| Signifying sickness | ||
| Fear of perpetual dependence | ‘I worry that I may have to take cholesterol medicine for the rest of my life.’ (U≥18) ‘Once I start taking [statins], I have to continue them.’ (U≥18) Responders’ impression was that once they began cholesterol-lowering medication it was something they would have to continue indefinitely for the rest of their lives. | 19,21,23,30,31,53 |
| Losing the battle | ‘It’s hard to accept it, [pauses] you are dependent on [statins], I have to take tablets to stay alive … and that’s a bit upsetting at times.’ (M≥18) ‘I’m a sick man now, I have to take tablets.’ (M≥18) Those who were on medication, taking their pills (usually each morning) was a daily reminder that their health had been compromised. | 19,21,23,24,30,52,54,56 |
| Financial strain | ‘I have cut back on social and recreational activities in order to pay for my cholesterol medicine.’ (U≥18) A patient discontinuing cholesterol-lowering therapy (CLT) reported having difficulty travelling to the clinic to obtain low-cost medications. | 21,31–33 |
Identifiers in brackets after the quotes: F = female, M = male, U = unknown sex, number = age in years; ≥18 = adult but unknown age.

{kind=link}
{kind=link}
Thematic schema.
Dark blue boxes = strong themes that explain barriers to taking statins. Blue text, black box outline = not as strongly expressed across the included studies but still mentioned by some patients (barriers to taking statins). Black text, blue box outline = facilitators to statin consumption. Light blue box = the outcome/end result affected by the barriers and facilitators requiring further investigation.
Confidence in prevention
Trust in efficacy
Participants reported noticing improvements in their cholesterol levels. Some regarded taking statins as ‘somewhere between essential and critical’ and felt fortunate that they had the option of effective medication to control their cholesterol and ‘potentially prolong [their] life’.17 Some patients tolerated undesirable side effects as they viewed stopping statins as ‘committing suicide’.18 Patients on secondary prevention in particular had strong beliefs that the improvement in their condition was attributable to statins. Some considered statins as more effective than alternatives such as behavioural and dietary changes.
Minimising long-term catastrophic CVD.
Some participants regarded statins as a preventive measure for serious health conditions that could occur in the long term, in particular CVD. They would ‘rather take these things [statins] now’ than being admitted into hospital with ‘some kind of stroke’,19 which they saw as life threatening or would impair their quality of life. As a result, some participants were hopeful that statins could prolong their lives. On the other hand, there were patients who felt that statins should not be used as a method of prevention, but only as a cure. One patient likened taking statins ‘for prevention’ to a person with a high risk of breast cancer undergoing a ‘double breast operation, removal’.20
Taking control
Taking statins was seen as a way of regaining control of compromised or deteriorating health. It gave participants a ‘sense of pride and accomplishment’, as they felt they were actively fighting against high cholesterol.17 Through this control, they were ‘hopeful’ about being able to restore health.21
Easing anxiety about high cholesterol
By taking statins, participants expressed relief from the stress and anxiety caused by the knowledge of their high cholesterol. Some participants found ‘a peace of mind’ and comfort in believing that statins protected them against CVD.17 Patients on secondary prevention reported an increase in confidence of managing problems related to CVD.
Routinising into daily life
Most participants perceived statins to be a relatively convenient way to manage cholesterol. They were able to easily integrate the medication into their lifestyles or existing regimens. Some used visual cues such as placing their morning dose of statin in a visible location to remind themselves to take their medication22 while others took it ‘automatically’. In one study, a participant found it inconvenient to split the tablet in half to take the prescribed dose and ceased taking statins.23 Some mentioned that disruptions in lifestyles such as vacations caused them to forget and miss doses.
Questioning utility
Imperceptible benefits
Some participants reported uncertainty about the efficacy of statins due to the absence of visible improvements in their health condition. They expected to feel ‘nothing’ on cessation of statins.24 For these reasons, certain participants did not believe in the importance of statins, and, therefore, readily forgot or chose to discontinue statins. For example, some participants stated that it was easier to forget to take statins as compared with medications that provide palpable symptom relief.
Uncertainties about pharmacological mechanisms
Some participants were ‘baffled’ about how statins worked in the body — ‘I don’t know whether it works in the liver or what’25 — although some participants understood that statins reduced their risk of CVD, they were confused about the relationship between any ‘residual clogging’ they had, and using statins as preventive medication.26 The uncertainty of how such a ‘powerful’ medication was absorbed into the body to target cholesterol caused some to be wary about taking statins.23 As well as actively seeking information, participants formed their own theories about statins, which made them nervous about committing to the regimen. For example, some thought that the medication would be ‘all the more effective’ when they avoided taking it daily.27 One study reported that participants were concerned that if their statin ‘didn’t work well, [it] could cause lipid accumulation’.28 Others, however, felt it was unnecessary to understand the pharmacology of statins.
Medical distrust
Scepticism about overprescribing
Some suspected that their GP may be prescribing statins unnecessarily as an automatic response to a slightly elevated cholesterol level, rather than based on a detailed review and consideration of the individual’s clinical characteristics and CVD risk profile.
Pressure to start therapy
Certain participants felt pressure from doctors to begin statin therapy. Some commented that they had to ‘give in’ after refusing many times, as the doctor ‘persuaded’ and ‘threaten[ed]’ with the possibility of future CVD complications.29
Threatening health
Competing priorities and risks
The decision to start and continue statin therapy depended on how participants valued other priorities over the perceived benefits of statins. Patients with other comorbidities such as type 2 diabetes tended to prioritise other medication over statins. Some older individuals expressed that they prioritised their health and longevity, and believed in the necessity of statins. Others perceived being able to live without the ‘hassle’ of statins as more important than lowering cholesterol,17 emphasising that it had to be ‘absolutely necessary’. One participant who believed statins would expose her to pregnancy complications chose not to take the medications, and consequently she felt like a ‘ticking time bomb’.21
Debilitating side effects
Some participants attributed a variety of side effects to statins and in particular described tiredness, muscle weakness, and pain as ‘brutal’ and insufferable.27 It seemed paradoxical to require more medication to counteract the side effects. For some, the side effects led to discontinuation of statins. The debilitating impact on their lives was to the extent that participants would ‘rather die of a heart attack’ than endure such discomfort and ‘vowed to never take such medication again’.21 Some felt that they were not properly informed about side effects before starting therapy and this caused some to speculate that statins caused adverse effects and symptoms, which they later acknowledged ‘could have been [caused by] anything’.19 Others experimented by ceasing medication to determine if it was causing the side effect(s).
Toxicity to body
Some participants stated that they perceived statins as ‘a load of trash’ that could potentially cause harmful long-term effects on the body.29 As a result, they preferred or opted for what they considered to be alternatives to statins, including dietary and other lifestyle changes. Some were specifically worried about the depletion of coenzyme Q10 (CoQ10), which they described as an essential coenzyme for healthy functioning of organs such as kidneys.23 Others believed that their ‘body needs to rest’ and avoided taking statins every day.27
Signifying sickness
Fear of perpetual dependence
Some participants expressed concern about having to take statins indefinitely and found it difficult to accept that they may have to use them for the rest of their lives. This exacerbated anxieties about harmful long-term effects.
Losing the battle
Studies reported some participants regarded statins as medications indicated only for patients with serious health conditions. Some considered themselves ‘not ill enough’ to take statins, which would signify a compromised health status. For patients taking medication, statins were a daily reminder that they were a ‘sick man now’.30 Participants also perceived that taking statins was indicative of their failure to manage their health on their own through ‘natural’ methods such as controlling their diet. It was ‘upsetting’ and ‘hard to accept’ that they were ‘dependent’ on the tablets to live on. Such distressing thoughts motivated some to look for ‘other ways’ such as lifestyle modification to control their cholesterol without medication.21
Financial strain
The cost of statins financially impaired some participants from the US. For some, it meant they had to ‘cut back on social and recreational activities’ in order to afford cholesterol-lowering medication.31
DISCUSSION
Summary
A confidence in the efficacy of statins in minimising the risk of life-threatening CVD, gaining reassurance about lowering cholesterol, and being able to integrate the medication regimen into daily routine facilitated the acceptance and uptake of statins. The statin-based regimen served as a form of psychological empowerment where patients felt in control of their health condition, and enabled them to be less anxious about having high cholesterol. However, others were concerned about the potential adverse effects of statins on their physical and mental health, with some viewing statins as a constant reminder of their compromised health and were reluctant to be dependent on long-term medications. The pharmacological mechanisms and tangible benefits were considered unclear by some responders, which patients explained were reasons for discontinuing statins. Also, some patients were suspicious about their clinicians’ motivations for prescribing statins and felt undue pressure to commence statin therapy.
There were some apparent differences based on the patient’s individual characteristics such as age, type of prevention, and risk factors. Older patients were particularly grateful for statins, noting that preventive measures for CVD were not readily available until recent decades. Patients who were prescribed statins for secondary prevention had particularly strong motivations to be healthy, having vividly experienced their risk of mortality during a CVD event. Study participants expressed conviction that statins would improve their health, and considered them to be more effective than behavioural or lifestyle changes. Similar sentiments were expressed in patients with a family or personal history of CVD and seemed more likely to tolerate side effects. They reported being proactive and diligent about taking statins as they perceived an urgent need towards lowering their cholesterol in protecting their health, having already encountered and experienced the seriousness of a CVD event. For some patients diagnosed with other conditions such as type 2 diabetes, taking statins was of relatively lower priority as they had other medications to take.
Although themes were broadly common across studies conducted in different health and geographical contexts, this study identified barriers specific to certain countries. Patients from the US expressed concerns about the cost of statin therapy being prohibitive to accessing their medications,21,31–33 which is a commonly reported barrier for the uptake and continued use for other medications in that country.34 In the UK, some patients were sceptical about overprescribing of statins.18–20 This perception may partly be driven by the media coverage of the Quality and Outcomes Framework, a scheme designed by the National Institute for Health and Care Excellence (NICE) that introduced incentivised prescription of statins to promote wider use of the medication.35
Strengths and limitations
In this study patients’ perspectives on statins were synthesised using a transparent and robust methodology to generate a new and comprehensive framework of themes reflecting data across settings and patient populations. HyperResearch was used to code the data to enable a traceable development of themes, and investigator triangulation was carried out to ensure all data reported in the primary studies were captured in these themes. This study also included findings from relevant chapters of unpublished PhD dissertations. However, there are some potential limitations. The review was limited to studies published in the English language, thus the transferability of the findings may be limited. For most of the data, the researchers were unable to specify whether they were derived in the context of primary or secondary prevention of CVD. It was also difficult to compare opinions based on comorbidities, and whether the patients were taking, had previously taken, were offered or not offered statins, as such information was often not provided in the included studies. Furthermore, many of the included studies were not reported comprehensively.
Comparison with existing literature
The findings in this study are consistent with systematic reviews describing patient perspectives on taking medications other than statins, which have shown that side effects play a vital role in decisions about treatment uptake across different health conditions.36 In a systematic review of patients across different chronic conditions, patients who were symptomatic were more likely to be adherent compared with patients who did not have perceptible symptoms.36 Patients who had severe headaches associated with hypertension were more inclined to adhere to therapy.37 Fear of prolonged dependence and uncertainties about pharmacological mechanisms have also been identified as barriers to medication uptake in this patient population, similar to findings from the present review.
The review presented here also provides some explanation about the patterns of initiating and sustaining statin therapy in patients. A recent study showed that, although 70% of patients reported that their doctors explained the importance of lowering cholesterol levels for their health, they felt discontent with the information provided by their doctors.42 Findings in this study suggest patients may want to know more about the reasons for prescription, pharmacological mechanism of the drug, potential bodily harm, and side effects. Another study conducted in the UK showed an increase in initiation and continuation of statins over the past 20 years among patients who had already had a myocardial infarction.43 As shown in the present review, patients with a personal or family history of cardiovascular events recognised the need to treat their risk factors, and readily trusted and appreciated the efficacy of pharmacological intervention in preventing future CVD events.
Implications for research and practice
Developing and evaluating interventions to minimise or prevent side effects, and help integrate the statin regimen into daily routine, appear to be needed. For example, patients were notably concerned about statin-induced muscle pain yet there is a lack of evidence on the effectiveness of interventions (for example, adjusting dosage, exercise) on improving these symptoms.38,39 There is very limited evidence that suggests taking CoQ10 with statins may provide relief of statin-induced muscle pain.40,41 The authors suggest the need for high-quality randomised controlled trial (RCT) evidence of interventions targeting specific side effects that are important to patients. To reduce burden of medication taking for patients, RCTs could assess various interventions such as visual cues, mobile applications for embedding statins in daily routines, which may improve continuation of statin therapy.
There is increasing recognition of the importance of patient empowerment in improving patient care, outcomes, and satisfaction in cardiology.44 Patient empowerment is a process by which patients are equipped with knowledge and autonomy to make shared decisions with their healthcare providers. Communication about potential harms, pharmacological mechanisms, and pragmatic ways to support medication taking may help patients feel more in control in their decisions regarding medications for CVD prevention. This process of patient empowerment also requires explicit discussion that addresses the patients’ priorities, goals, doubts, and concerns about statins in the context of other interventions (exercise, diet, or other medications) targeted at preventing CVD. Such a collaborative and comprehensive approach may contribute to a more patient-centred and effective CVD prevention strategy by increasing patient satisfaction and adherence to therapy.
Patients commence and continue statins in the expectation that they will minimise their risk of CVD, and to gain reassurance that their health is under control. Statins are among the most commonly used medications worldwide, with the majority of people continuing long term, so the factors motivating use would appear, on a population level, to outweigh those inhibiting it. Side effects, lack of perceptible symptoms, being reminded of their compromised health status because of the need for medications, fear of causing additional bodily harm, costs, and concerns about long-term dependence on statins were barriers to accepting and taking statins. Some also questioned the motives of clinicians in prescribing statins. Explicitly addressing patient concerns and priorities by explaining reasons for prescribing statins and risks involved, informing possible ways to manage side effects, and implementing strategies to routinise medication taking, may improve patient satisfaction and continuation of statins. This may ultimately lead to better outcomes in the primary and secondary prevention of CVD.
Notes
Funding
This work is supported by a National Health and Medical Research Council Partnership Grant (NHMRC) (1092674), including support from the National Heart Foundation of Australia, and an NHMRC Program Grant (1092597). Allison Tong and Emily Banks are supported by NHMRC Fellowships (1106716 and 1042717, respectively). The funders had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Ethical approval
Ethical approval was not required.
Provenance
Freely submitted; externally peer reviewed
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received September 26, 2017.
- Revision requested October 10, 2017.
- Accepted October 24, 2017.
- © British Journal of General Practice 2018
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

