


Abstract
Background Polypharmacy is becoming more prevalent and evaluation of appropriateness of medication use is increasingly important. The primary care physician often conducts the deprescribing process; however, there are several barriers to implementing this.
Aim To examine the feasibility and safety of discontinuation of medication, with a focus on studies that have been conducted in the community, that is, primary care (or general practice) and nursing homes.
Design and setting This systematic review included randomised controlled trials published in 2005–2017, which studied withdrawal of long-term drugs prescribed in primary care settings and compared continuing medication with discontinuing.
Method PubMed and EMBASE searches were conducted and the extracted data included the number of patients who successfully stopped medication and the number of patients who experienced relapse of symptoms or restarted medication.
Results A total of 27 studies reported in 26 papers were included in this review. The number of participants in the studies varied from 20 to 2471 and the mean age of participants ranged from 50.3 years to 89.2 years. The proportion of patients who successfully stopped their medication varied from 20% to 100%, and the range of reported relapse varied from 1.9% to 80%.
Conclusion Only a few studies have examined the success rate and safety of discontinuing medication in primary care, and these studies are very heterogeneous. Most studies show that deprescribing and cessation of long-term use seem safe; however, there is a risk of relapse of symptoms. More research is needed to advise physicians in making evidence-based decisions about deprescribing in primary care settings.
INTRODUCTION
The number of drug prescriptions per patient is slowly rising1 and polypharmacy — that is, the use of multiple drugs administered to the same patient (usually more than four or five medicines) — is becoming more prevalent. Evaluation of appropriateness of medication use is increasingly important, given the mounting evidence for harm. Recent studies report that the risk for adverse drug reactions, falls, disability, and mortality rises significantly with each additional medication used.2 In addition, using multiple medications increases the risk of adverse drug events, drug interactions, medication non-adherence, decreased functional status, and geriatric syndromes.3 Several studies have emphasised the importance of reducing unnecessary medication use4 and polypharmacy,5 and suggested deprescribing of medication.6–8 Deprescribing is the process of withdrawal of an inappropriate medication, supervised by a healthcare professional with the goal of managing polypharmacy and improving outcomes.9 Little is known about the clinical effectiveness of stopping medication in patients, both positive and negative.
A systematic review10 found some evidence that specific classes of medications can be withdrawn in a substantial proportion of older people without generating any harm. Unfortunately, the included trials were small and only studied withdrawal of thiazide diuretics or psychotropic medication. A more recent meta-analysis covering a wide range of conditions and medications11 concluded that deprescribing is often achieved without adverse changes in quality of life or health outcomes and might improve longevity. This review included studies in different settings, such as hospitals, outpatient facilities, general practice, and retirement villages.
Care for patients with chronic diseases predominantly takes place in the community. The primary care physician, or nursing home specialist if the patient is living in a nursing home, plays a crucial role in reviewing and managing a patient’s medication, as they have detailed knowledge of their patient’s past and current diagnoses and treatments. Thus, it would be most appropriate if the primary care physician conducted the deprescribing process. However, there are several barriers to implementing this. Patients in general practice have a wide variety of comorbid conditions and tend to be less compliant.12 Also, because of the individual needs and preferences of patients, implementation of guidelines can be difficult in general practice.13 Additionally, fear of specialists’ disapproval can impact on the success of stopping medication.14 GPs need more evidence to support them in successfully completing the deprescribing process and it is important that they are able to inform their patients about the feasibility and potential risks of stopping medication.
How this fits in
Deprescribing has been shown to have a low risk of adverse changes in health outcomes in hospital settings. The success rate of deprescribing interventions in general practice in terms of duration of discontinuation or relapse of symptoms is not clear. Research articles about deprescribing interventions in general practice often do not report on the number of long-term discontinuations, frequency of relapse of symptoms, or frequency of restarting medication. This systematic review showed that deprescribing can be done safely; however, risk of relapse should be considered.
Therefore, the aim of this review was to examine the feasibility and safety of discontinuation medication, with a focus on studies that have been conducted in the community, that is, primary care (general practice) and nursing homes.
METHOD
Search strategy
PubMed and EMBASE were searched for randomised controlled trials (RCTs) published between 2005 and 2017, using the keywords discontinu* or withdraw* or deprescribing or cessation or stop* of treatment or drugs (the full search strategy is available from the authors on request).
Selection of publications
Screening of search results was performed by two authors, who reviewed all papers independently. First selection was based on titles and abstracts. Full texts were examined for eligibility of potentially relevant reports. Additional references were sourced through reviewing bibliographies of identified trials. Discrepancies were resolved by consulting a third author.
Inclusion and exclusion criteria
The following inclusion criteria were used: withdrawal of one or more long-term drugs, the study aimed to assess effectiveness of withdrawal on clinical outcomes (as opposed to laboratory outcomes), RCT, comparison of continuing medication versus discontinuing, and patients treated in primary care or nursing home. Long-term medication was defined as use of >4 weeks. Not all studies explicitly mentioned the setting, in which case it was considered whether the medication was likely to be prescribed or stopped by a GP or nursing home specialist. A decision about this was made in consensus between the authors, who are all experienced clinicians in primary care.
Studies performed in secondary and tertiary care (for example, medications prescribed by medical specialists, such as chemotherapy, anti-HIV medication, anti-epileptics, or rheumatoid arthritis drugs) or focusing on children aged <18 years, and pregnant women were excluded. Studies aimed at withdrawal of addictive substances (for example, tobacco, alcohol, and opioids) were also excluded.
Extraction of items
All authors agreed on a list of data, relevant to medication withdrawal, to extract based on their clinical experience and a pilot data extraction on three papers. The included studies were classified based on the health domain for which the medication was prescribed. Data were extracted from each article by two authors and entered into an Excel spreadsheet.
Study characteristics
Basic study characteristics included study duration, location, population size, and age of participants.
Outcomes
Feasibility of deprescribing was the number of patients who successfully stopped medication. Safety was defined as the number of patients who experienced relapse of symptoms or restarted medication. When relapse of symptoms or recommencing medication were not mentioned, early dropout of the study, which could be considered as a proxy of the tolerability of stopping or continuing medication, was also reviewed. Additionally, the estimate of effect on the primary outcome of the study was considered.
Risk of bias
Risk of bias was assessed using the Cochrane Collaboration’s tool for assessing risk of bias, that is, selection, performance, detection, and attrition bias.15 Assessment of random sequence generation, allocation concealment, and blinding (where appropriate) is reported.
RESULTS
Selection of publications
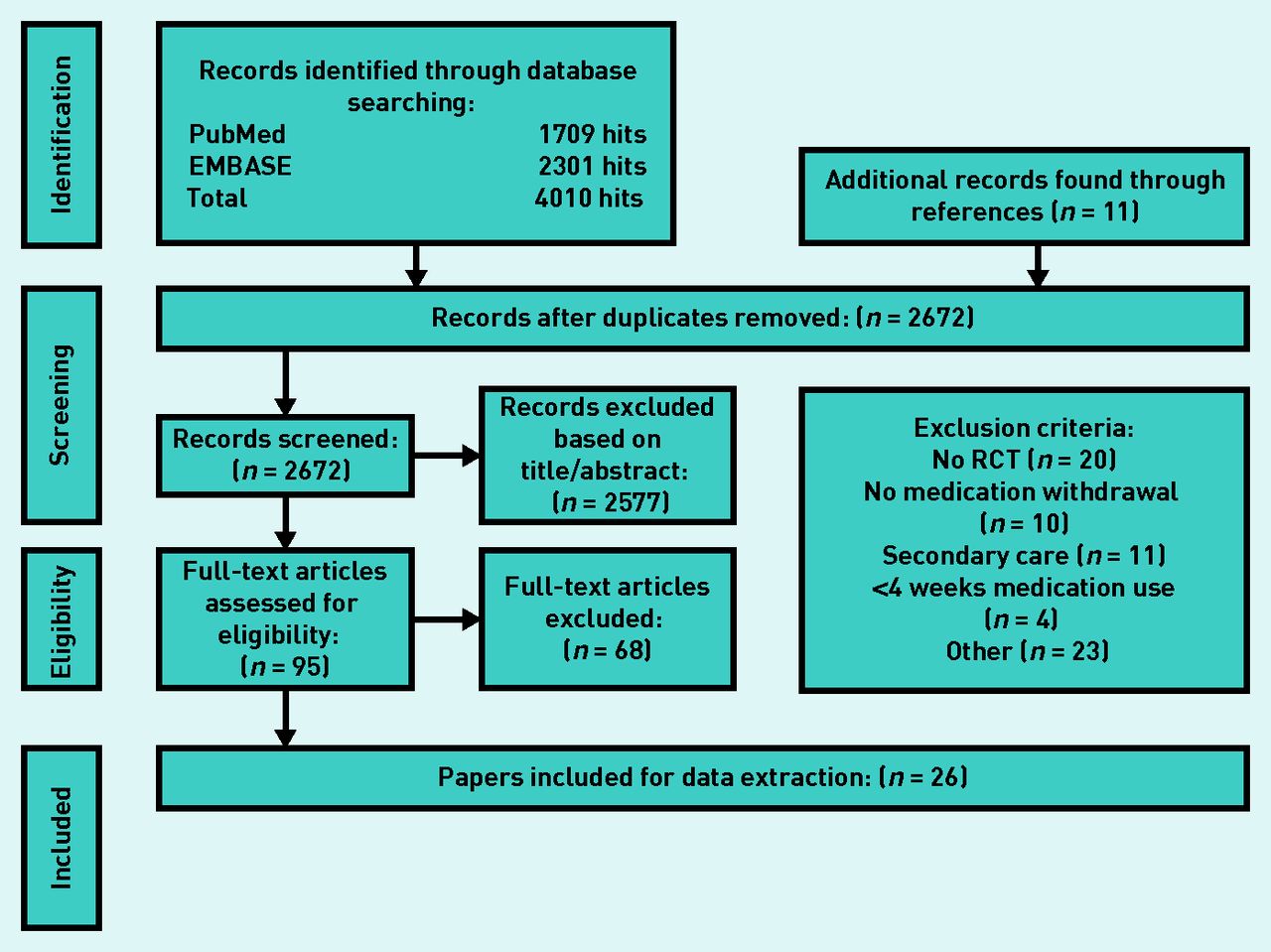
The search identified 2672 publications of which 95 were included for full-text screening. A total of 27 studies reported in 26 papers were included in this review (Figure 1). Of the 95 full texts most were excluded because they were not RCTs (n = 20), there was no medication withdrawal (n = 10), medication was prescribed in secondary care (n = 11), or medication was used <4 weeks (n = 4).

Flowchart of study inclusion.
Characteristics of selected publications
Sixteen placebo-controlled trials and eleven trials that compared continuing versus discontinuing medication were included. Seven trials also added a third arm. Overall, the studies were very heterogeneous. There was a large variety of medications studied, variable group sizes, differences in mean age, and in follow-up time (further details are available from the authors on request). Therefore, a meta-analysis was not appropriate and results are reported as aggregated data in tables.
The studies were classified based on the health domain for which the medication that was evaluated was prescribed (Table 1). The domains were empirically classified based on the selected papers. Six studies investigated deprescribing in cardiovascular disease, six in psychiatric and behavioural disease, and five studies in cognitive impairment. Categories with three or less studies were classified as ‘other’ (for example, medication for benign prostate hypertrophy or osteoporosis, inhalation corticosteroids, proton pump inhibitors, and withdrawal of multiple medications).
Summary of study characteristics and outcomes
The number of participants in the studies varied from 20 in the smallest study16 to 2471 in the largest study.17 The mean age of participants varied between 50.3 years18 and 89.2 years.19 Seven studies included patients with a mean age <65 years and 19 studies had a mean age >65 years; in one study age was not mentioned.
The follow-up time varied from 4 weeks20 to 5 years.21 Most studies were conducted in Europe (n = 13) and the US (n = 8), with two studies from Taiwan, one study from Canada, one from Australia, one from Brazil, and one from South Korea. Eleven studies were conducted in general practices or in outpatient clinics,16,18,22–30 five in nursing homes,19,31–34 three were done in hospitals as well as individual physician practices17,35,36 and one was conducted in a palliative care setting.37 The other papers did not specify the setting of the study20,21,38–41 (further details are available from the authors on request).
Risk of bias within studies
Randomisation procedures were in place in 84.6% of the studies. However, in 50% of studies allocation concealment was not done or unclear. Blinding of study personnel and participants, and blinding of outcome assessors, was ensured in 65.4% and 42.3% respectively (Box 1).
Risk of bias
| Study | Random sequence generation | Allocation concealment | Blinding of study participants and personnel | Blinding of outcome assessment |
|---|---|---|---|---|
| Ahmed, 200717 |
 |
 |
 |
 |
| Kutner, 201537 |
 |
 |
 |
 |
| Lemos, 201438 |
 |
 |
 |
 |
| Lewin, 201220 |
 |
 |
 |
 |
| Moonen, 201522 |
 |
 |
 |
 |
| Moonen, 201630 |
 |
 |
 |
 |
| Ballard, 200931 |
 |
 |
 |
 |
| Bergh, 201232 |
 |
 |
 |
 |
| Devanand, 201116 |
 |
 |
 |
 |
| Devanand, 201235 |
 |
 |
 |
 |
| Huijbers, 201618 |
 |
 |
 |
 |
| Ruths, 200833 |
 |
 |
 |
 |
| Gaudig, 201139 |
 |
 |
 |
 |
| Herrmann, 201619 |
 |
 |
 |
 |
| Howard, 201229 |
 |
 |
 |
 |
| Scarpini, 201123 |
 |
 |
 |
 |
| Lee, 201226 |
 |
 |
 |
 |
| Liaw, 200640 |
 |
 |
 |
 |
| Lin, 201441 |
 |
 |
 |
 |
| Black, 200621 |
 |
 |
 |
 |
| Naylor, 201024 |
 |
 |
 |
 |
| Choudhury, 200725 |
 |
 |
 |
 |
| Wouters, 200536 |
 |
 |
 |
 |
| Zwisler, 201527 |
 |
 |
 |
 |
| Boye, 201728 |
 |
 |
 |
 |
| Potter, 201634 |
 |
 |
 |
 |
| Total | 22/26 = 84.6% | 13/26 = 50% | 17/26 = 65.4% | 11/26 = 42.3% |
Green = low risk of bias. Red = high risk of bias. Yellow = unclear risk of bias
Synthesis of results
Eleven studies focused on the feasibility of medication cessation as well as on clinical outcomes.18–20,23,25,27,33–35,37,41 The other 16 studies reported effects on biological markers or clinical outcomes.
Success of medication cessation
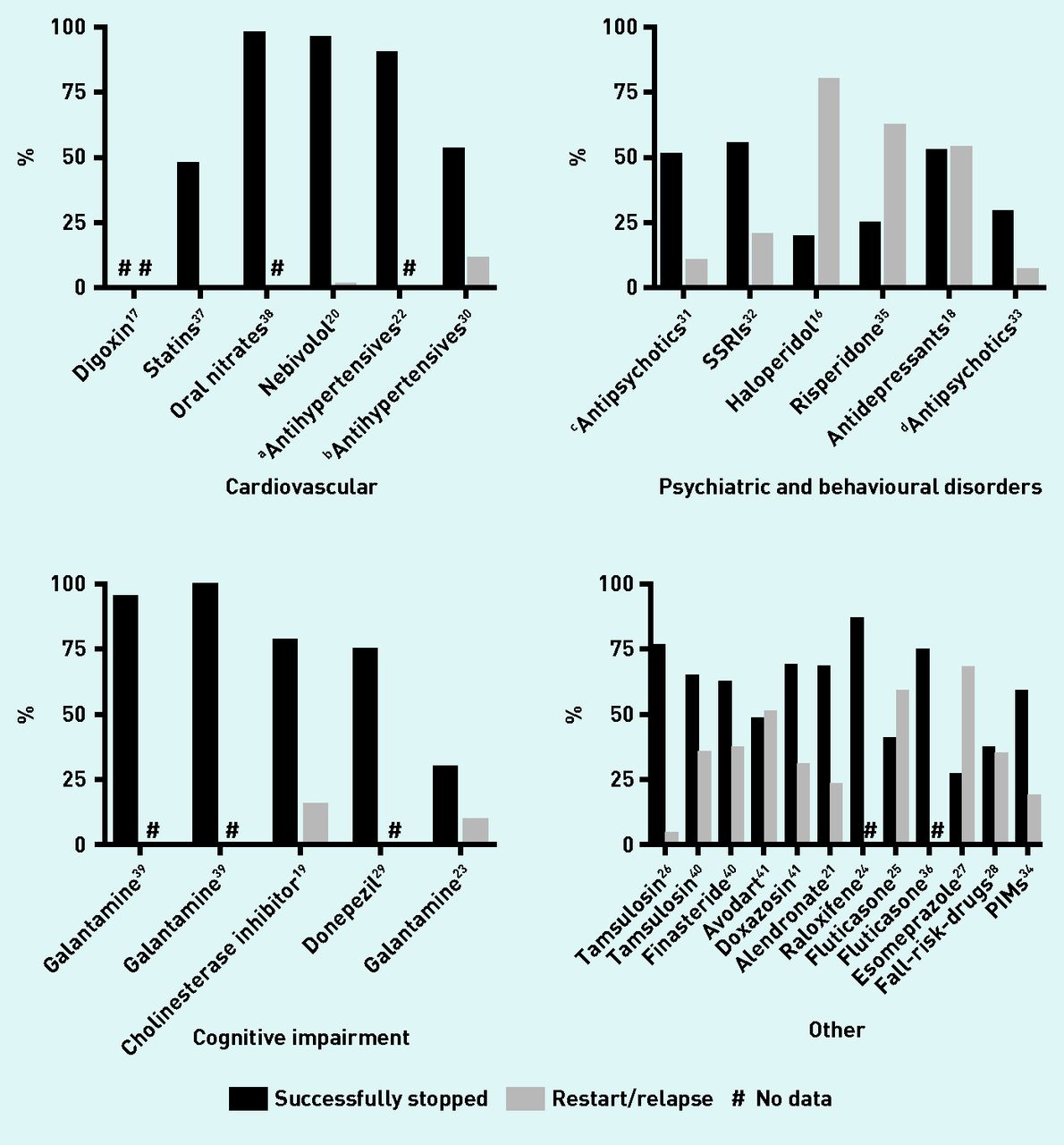
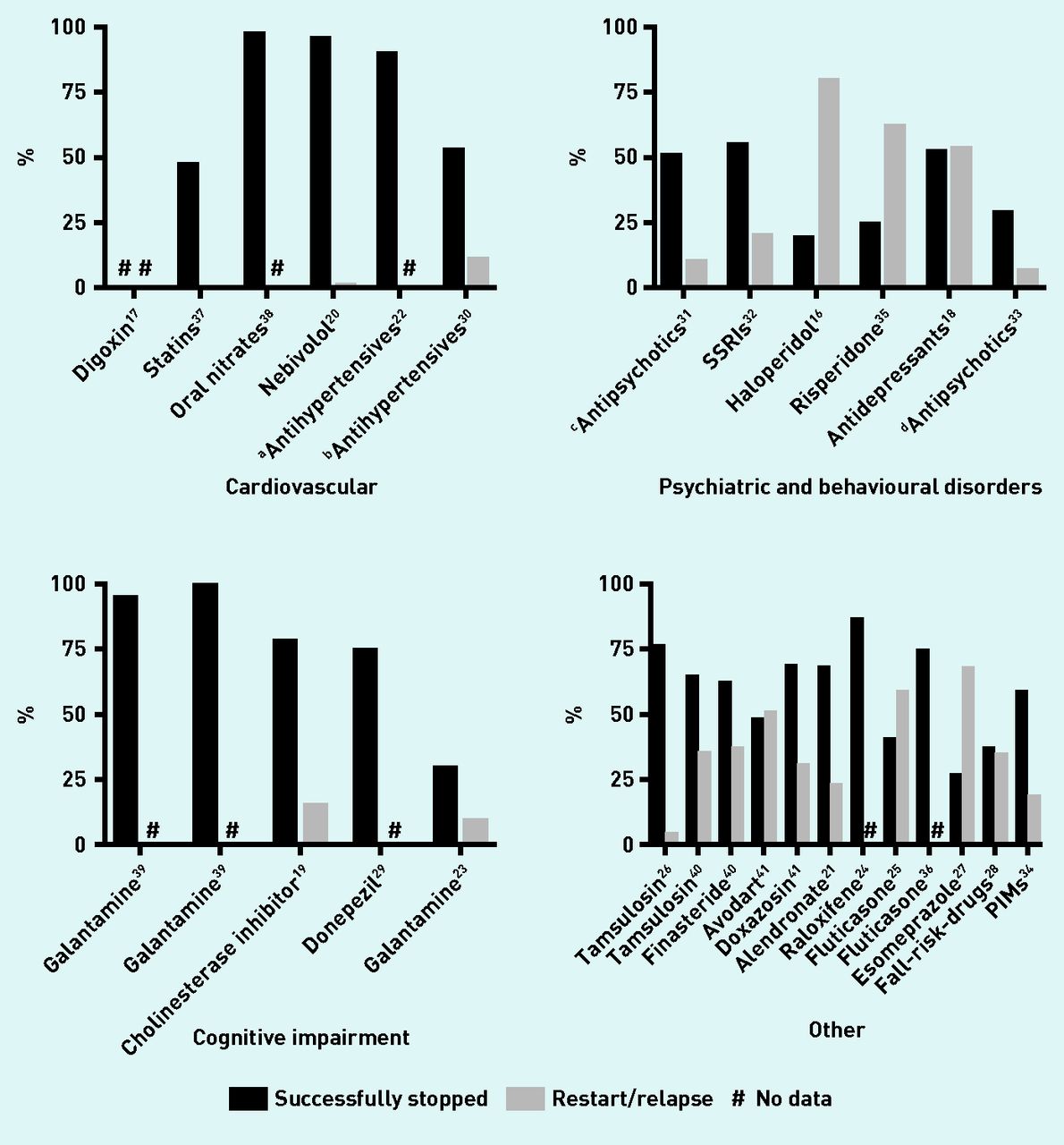
The proportion of patients who successfully stopped their medication varied from 20%16 to 100%39 (Table 2). In 19 studies the proportion of participants that had successfully stopped medication was >50% (Figure 2).
Proportion of subjects with successful stopped medication, relapse, or early dropout
{kind=link}
{kind=link}
Percentages of successful medication cessation and restart of medication or relapse of symptoms. aBB, diurectic, ACEI, ATII-blocker, and CCB or combination. bDiuretic, BB, AT-blocker, ACEI, and CCB. cRisperidone, haloperidol, and other antipsychotics. dRisperidone, haloperidol, olanzapine. ACEI = angiotensin-converting enzyme inhibitor. AT = angiotensin. BB = beta-blocker. CCB = calcium channel blocker. PIM = possible inappropriate medication. SSRI = serotonin selective reuptake inhibitor.
Restart of medication and relapse of symptoms
The number of patients experiencing relapse of symptoms or whose medication was restarted was mentioned in 16 of 27 studies. The range of reported relapse varied from 0%37 to 80%16 (Table 2).
Nine studies reported rate of relapse for both placebo and control groups. Five of these studies found a significant difference between both groups, with more relapse in the intervention group compared with the control group: 20.6% versus 6.2%,32 80.0% versus 40.0%,16 62.5% versus 46.9%,35 54.0% versus 38.8%,18 and 68.2% versus 18.6%27 in intervention group versus control group respectively, and three did not perform statistical testing19,21,25 (Table 1). The other eight studies reported relapse for only the intervention group or for the entire research population. One study did not find a significant difference23 and seven did not perform statistical testing of the observed difference.20,26,28,30,31,33,34
Drop out of the study
Seven studies that did not report relapse of restarting medication reported early study termination: five studies (including two by Gaudig et al39) found a dropout rate of <15%22,24,38,39 and two of >15%.29,36 Five29,36,38,39 of these seven studies reported more dropouts in the control group than the intervention group, but no statistical analyses are reported.
Adverse events
Eight studies21,29,30,34–36,39 found no significant difference between comparator groups and seven studies18,19,22,26,27,37,38 reported that adverse events were rare and no serious adverse events occurred. One study20 reported more serious adverse events in the control group but did not report significance calculation. The other 10 studies16,17,23–25,28,31–33,40 did not provide detailed information about adverse events (further information is available from the authors on request).
Primary outcomes
All studies used statistical tests to analyse the differences between the intervention group (placebo or discontinue medication) and control group (continue medication) for their primary outcome. The primary outcomes of the studies varied widely and can be categorised in three groups: mortality, clinical outcomes (for example, change in clinical observation tools such as health-related quality of life, Neuropsychiatric Inventory, Alzheimer’s Disease Assessment Scale-Cognitive Subscale-11 and Mini Mental State Exam, chronic obstructive pulmonary disease exacerbation frequency, number of new falls, number of medications taken, or time to discontinuation with trial medications), and biological outcomes (for example, mean change in diastolic and systolic blood pressures, prostatic volume, total hip bone mineral density, differences in bone markers, and forced expiratory volume in 1 second) (further information is available from the authors on request). Twelve studies found a significant difference in favour of the control group, of which eight looked at clinical outcomes16,18,27,29,32,35,38,39 and four at biological outcomes,20,21,24,36 two studies found a significant difference in favour of the intervention group, of which one looked at mortality31 and one34 at the number of medicines successfully discontinued, and 12 studies found no difference between the groups, of which two reported mortality,17,37 seven clinical outcomes,19,22,23,25,28,33,39 and three biological outcomes.26,30,40 One study found a significant difference of stopping one medication over another regarding biological outcomes.41
DISCUSSION
Summary
This systematic review found that between 2005 and 2017 only a few studies examined the feasibility and safety of discontinuing medication in primary care settings. The identified trials were heterogeneous, studying a wide variety of medications, with large differences in the number of participants, age, and follow-up time. There is a large variety between studies in the number of patients who successfully stopped medication, but most studies found that >50% of participants in the deprescribing group were able to successfully stop medication.
Safety of stopping medication was not specifically examined in the studies included in this review. It was considered that the negative effects of stopping medication would be relapse of symptoms or the need to restart medication, and therefore these factors were chosen as a measure of safety. Only six of the 27 studies assessed the difference between intervention and control group regarding the proportion of patients experiencing relapse of symptoms or the need to restart the discontinued medication. Most of these studies reported significantly more relapses in the group that discontinued medication. However, despite the greater relapse risk in these groups, a clinically important proportion of patients was still able to successfully stop the medication.16,18,27,32,35
A large number of included studies did not have sufficient concealment of allocation, blinding of participants, researchers, or outcome measurements. This could have caused substantial bias with regard to the outcomes on relapse symptoms.
Primary outcomes reported in the included studies were mortality, clinical outcomes, and biological outcomes. Twelve studies found a significant difference in favour of the control group on primary outcomes. However, 12 studies did not find a significant difference, which means that stopping medication was not worse than continuing, and two studies did find a significant difference in favour of the intervention group. It was not possible to identify a medication class for which deprescribing was more successful.
Strengths and limitations
The strength of this systematic review is that it included only RCTs, which allowed examination of the effects of deprescribing compared with continuing medication or usual care. The primary outcomes of the studies included in this review mainly focus on clinical or biological effects of deprescribing and not on the number of participants who successfully stopped or who experienced a relapse of symptoms. Because of this it is difficult to draw a firm conclusion about feasibility of deprescribing.
The search was restricted to PubMed and EMBASE, which means the authors may have missed studies. However, these two databases cover a wide range of studies, including non-English language publications. Studies published after 2005 were included, as this would reduce the risk of including drugs that are no longer relevant to current practice. It is possible that some publications have been missed that could have been relevant for the research question. Page et al 11 reviewed deprescribing studies without date limit, and the authors found that 13 studies included in their review would have met the inclusion criteria of the current review if a date limit had not been set. Five of these studies investigated the effect of deprescribing diuretics, a class of medication that was not studied in the cohort of studies published after 2005.42–46 The other eight studies in the Page review studied similar medications as included in the papers in the current review covering deprescribing studies published between 2005 and 2017 (for example, nitrates, selective serotonin reuptake inhibitors, antipsychotics, benzodiazepines, and inhalation corticosteroids).47–54
Presumably, the way a deprescribing intervention is implemented might be more important than the type of drug that is deprescribed. This review did not explore the strategies used to cease the long-term medication. A better understanding of successful strategies or tools can assist clinicians and patients. Anderson et al showed that knowledge and information are important enablers for professionals to start deprescribing.55 Therefore, availability of evidence-based tools, such as deprescribing algorithms, may play an important role in the success of the intervention.56
Comparison with existing literature
The authors of a recent systematic review of deprescribing in older adults (>65 years)11 came to similar conclusions: deprescribing is feasible, but there is a large variation in clinical effects and no specific drug class is more likely to be successfully deprescribed. However, the review by Page et al included studies conducted in outpatient departments and hospitals, and focused on the outcome mortality.11 The current systematic review focused specifically on primary care, as this is where most deprescribing occurs. It chose to assess the effectiveness on clinical outcomes, success rate, and safety, rather than mortality, as this information is relevant for individual physicians and patients.
Another systematic review10 also concludes that medications can be stopped without causing harm, and that when symptoms recur these could be easily treated by recommencing the medication. The authors note that most studies are of limited quality and argue that clinical trials measuring effectiveness of medication cessation need to be redesigned to facilitate the specific characteristics of withdrawal studies.
An earlier review of trials57 investigated the effects of drug cessation on falls, delirium, and cognitive impairment, and on cessation of inappropriate medication in end-of-life situations. They concluded that cessation of psychotropic medication was associated with a reduction in the occurrence of falls and improvement of cognitive function. The authors also point to the fact that sufficient evidence about the effects of deprescribing is still missing.
Implications for research and practice
Research reports about deprescribing interventions often do not report on the number of long-term discontinuations, frequency of relapse of symptoms, or frequency of restarting medication, which would be important to know for clinicians as well as individual patients. Only a few studies have considered the feasibility and safety of discontinuing medication in primary care. Most studies show that deprescribing and cessation of long-term use of medication seems safe; however, there is a risk of relapse of symptoms. Therefore, decisions around deprescribing need to be made by weighing the available evidence and applying this to each individual patient. Studies investigating the effectiveness of deprescribing in primary care need to report patient-relevant outcomes and provide clear data on all effects, including risk of relapse or harm.
More research looking at the most effective strategies for deprescribing, as well as how to overcome doctor and patient barriers, is needed to support physicians and patients in making evidence-based decisions about deprescribing in primary care settings.
Acknowledgments
The authors thank the librarians of LUMC Walaeus Library for their help in conducting the PubMed and EMBASE search. They also thank Patrick Rijkschroeff for his help in configuring the graphs.
Notes
Funding
None.
Ethical approval
Not applicable.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received April 13, 2018.
- Revision requested June 19, 2018.
- Accepted August 20, 2018.
- © British Journal of General Practice 2018
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

