


Abstract
Background Polypharmacy is common among older adults, with increasing numbers also using prescription drugs with herbal medicinal products (HMPs) and dietary supplements. There is no reliable evidence from the UK on concurrent use of HMPs and dietary supplements with prescription drugs in older adults.
Aim To establish prevalence of concurrent prescription drugs, HMPs, and dietary supplements among UK community-dwelling older adults and identify potential interactions.
Design and setting Cross-sectional survey of older adults registered at two general practices in South East England.
Method A questionnaire asking about prescription medications, HMPs, and sociodemographic information was posted to 400 older adults aged ≥65 years, identified as taking ≥1 prescription drug.
Results In total 155 questionnaires were returned (response rate = 38.8%) and the prevalence of concurrent HMPs and dietary supplements with prescriptions was 33.6%. Females were more likely than males to be concurrent users (43.4% versus 22.5%; P = 0.009). The number of HMPs and dietary supplements ranged from 1 to 8, (mean = 3, median = 1; standard deviation = 1.65). The majority of concurrent users (78.0%) used dietary supplements with prescription drugs. The most commonly used dietary supplements were cod liver oil, glucosamine, multivitamins, and vitamin D. Others (20.0%) used only HMPs with prescription drugs. Common HMPs were evening primrose oil, valerian, and Nytol Herbal® (a combination of hops, gentian, and passion flower). Sixteen participants (32.6%) were at risk of potential adverse drug interactions.
Conclusion GPs should routinely ask questions regarding herbal and supplement use, to identify and manage older adults at potential risk of adverse drug interactions.
INTRODUCTION
Polypharmacy is a recognised patient safety risk among older adults.1,2 Although standard definitions of polypharmacy do not generally include herbal medicinal products (HMPs) and dietary supplements, they increase the risk of adverse drug events through potential interactions.3–5 Use of herbal medicines and dietary supplements by older adults is common.6–10 Also, medication-related problems are higher among older adults because of comorbidities and reduced clearance of pharmacologically active compounds.11
A recent systematic review12 established that concurrent use of prescription drugs and HMPs is substantial among older adults, with potential interactions from some herb–drug combinations such as garlic–aspirin and ginseng–warfarin. However, the only available UK study on this issue among older adults13 is nearly 15 years old, included people aged ≥50 years, and relied on a self-selected sample from a magazine’s readership.
The aims of the study were to establish prevalence, and to identify patterns and potential herb–drug interactions from concurrent use of prescription drugs, HMPs, and dietary supplements among UK community-dwelling older adults.
METHOD
A cross-sectional survey was conducted using self-administered questionnaires between January and April 2016. Data were from a purposive sample of community-dwelling older adults registered at two general practices in South East England. Practice A was a small village practice in Essex, with a predominantly white population and about 19.5% aged ≥65 years. Practice B was a large urban practice in Haringey, North London, with a sizeable black, Asian, and minority ethnic (BAME) population, of up to 9% aged ≥65 years.
Informed by findings from a systematic review on concurrent use of HMPs with prescription drugs,12 the questionnaire covered demographics, prescription drugs, HMPs, and dietary supplements not prescribed by the GP, the rationale for taking them, and how often. Participants were also asked about side effects and perceived benefits of medicines and/or HMPs (further information is available from the authors on request).
As no consistent terms exist for HMPs, some examples of common HMPs were included to show participants the possible breadth of responses. The questionnaire was piloted among 15 community dwelling older adults and, following minor amendments, the questionnaire consisted of 18 questions and took between 20 to 30 minutes to complete.
How this fits in
Older adults use herbal medicinal products (HMPs) and dietary supplements with prescription drugs to manage chronic conditions and to maintain health. The use of HMPs and dietary supplements with prescription drugs among older adults is under-researched. Concurrent use of HMPs and dietary supplements with warfarin, statins, and anti-inflammatory drugs is common among UK older adults. One in three concurrent users is at risk of a potential herb–drug or supplement–drug interaction.
Sample size calculation and sampling
The sample size was based on previous research evidence that up to 50% of older adults use HMPs.14–16 To achieve a confidence interval (CI) of 95% and ±7.5% accuracy, a power calculation (using G*Power version 3.1.9.2) gave the total sample size required as 171 responders (using the worst-case scenario of actual proportion being 50%).
Purposive sampling17,18 was used to obtain a sample of older adults registered at two general practices, in Essex and Haringey. Participants had to be ≥65 years, using at least one prescription drug, and able to consent. Terminally ill patients, patients with dementia, or patients assessed as lacking capacity were excluded.
To account for attrition from low responses, which are common with mailed surveys, 200 participants who met inclusion criteria were randomly selected from a list of patients in each of the two practices. Practice administrators posted study packs (a letter of invitation addressed personally to the patient, participant information sheets [PIS], the questionnaire, and a reply-paid envelope) to selected patients. Reminder letters were sent after 2 weeks. If there was no reply, new study packs were sent to all non-responders.
Data analysis
Responders were defined as ‘concurrent users’ if they reported using HMPs or dietary supplements. Anonymised data were recorded and double checked; discrepancies were corrected and analysed using SPSS (version 23.0). Descriptive statistics were calculated to summarise the sample. Using Fisher’s exact test, associations between concurrent use and demographic factors, such as sex, educational qualifications, and living arrangements, were tested. Statistical significance was measured at 5% level.
Potential interactions between combinations of prescription drugs, HMPs, and dietary supplements were assessed using Stockley’s Herbal Medicines Interactions (https://about.medicinescomplete.com/publication/stockleys-herbal-medicines-interactions-2/). Stockley’s Herbal Medicines Interactions is a comprehensive evidence database. Information regarding potential interactions between herbal medicines (including nutritional supplements and some food) and conventional medicines are expertly assessed with practical advice provided and regularly updated.
Interactions are rated on three criteria: whether action is required to address the interaction (action); likely effect of the interaction on the patient if unmanaged (severity); and weight of available evidence regarding the interaction (evidence). Based on these criteria, drug–herb or drug–supplement combination is described by one of five outcomes ranging from no interaction, doubt about outcomes, potentially hazardous outcomes, significant hazard, and life-threatening outcomes.
All drug–herb and drug–supplement combinations were assessed and rated for potential interactions by one author and double checked by a second author who is a registered pharmacist. Any disagreements on rating were resolved through discussion.
RESULTS
Table 1 shows sociodemographic characteristics of the 149 responders included in the final analysis (six responders were excluded for not providing information on medications). A power calculation based on 80% power and significance level of 5% for a two-tailed test showed that a sample of 128 (64 in each group) was sufficient to detect medium standardised effect size, and thus the results are unaffected by the shortfall in the desired number of responders.
Demographics of concurrent users and non-concurrent users (n = 149)
Of these 149 responders, 76 (51.0%) were female and 71 (47.7%) were male; two participants did not indicate gender. The majority (106; 71.1%) were aged 65–74 years; none were ≥95 years. About half of participants (73; 49.6%) lived with a partner or spouse, whereas 31.3% lived alone. Most responders identified as white (126; 85.7%), with 15 (10.1%) black or black British and only one Asian or Asian British.
There was almost an even split in educational level between responders: 70 (46.9%) with further education after secondary school and 77 (51.7%) with no education beyond secondary school. Only one participant, a concurrent user, had a clinical background in nursing.
Prevalence and pattern of concurrent use
Approximately one-third of responders reported concurrent use of HMPs and dietary supplements with prescribed medications in the last 12 months. The prevalence of concurrent use is thus 33.6%.
Females were more likely than males to be concurrent users (43.4% versus 22.5%, P = 0.009). There is little difference between groups that had or had no further education with each having about one-third reporting concurrent use. Similarly, there were little differences between the categories of living arrangements. Those living with children reported somewhat lower levels of concurrent use but this was not statistically significant.
Concurrent users (n = 50) reported 55 herb–drug and supplement–drug combinations. The number of HMPs and dietary supplements ranged from 1 to 8, mean value of 3 (standard deviation = 1.65, median = 1).
All responders were taking ≥1 prescription drugs on a regular basis, range 1 to 18 (median = 3). A total of 180 different types of prescription drugs were reported by 149 participants (mean = 3.96, standard deviation = 2.52). The most reported drug classes were statins (69; 46.3%), beta-blockers (26; 17.4%), calcium channel blockers (23; 15.4%), non-steroidal anti-inflammatory drugs (NSAIDs) (19; 12.7%), biguanides (18; 12.1%), angiotensin-converting enzyme (ACE) inhibitors (18; 12.1%), and proton pump inhibitors (18; 12.1%).
Ten concurrent users (20.0%) used only HMPs with prescriptions. Thirty-six different herbs (used either singly or as a combination product) were reported. The most commonly used HMPs were evening primrose oil, valerian, Nytol Herbal® (a combination of hops, valerian, gentian, and passion flower), and garlic (Figure 1).
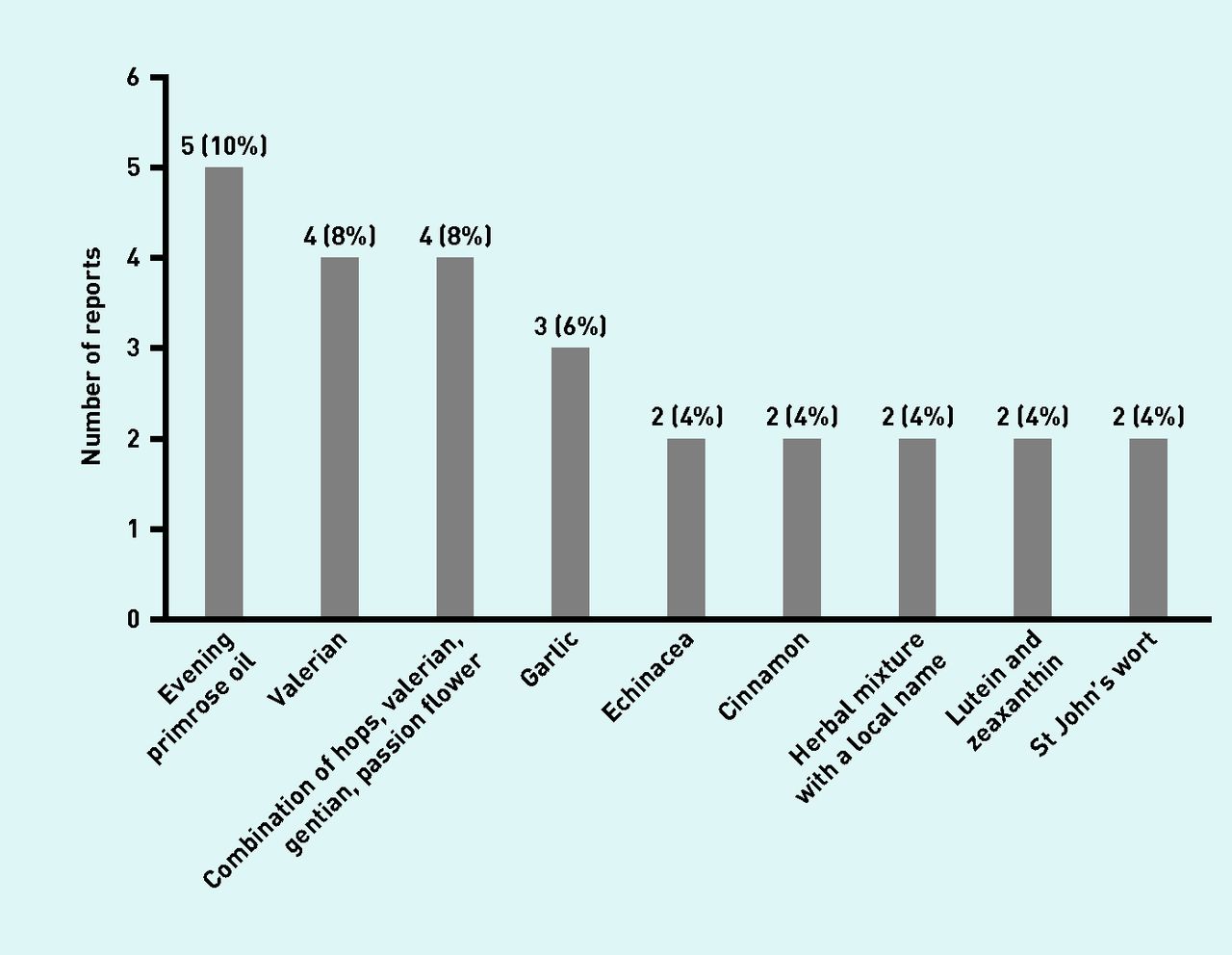
HMPs most frequently used concurrently with prescription by UK older adults. Percentages sum to more than 100% as individuals could report more than one HMP.
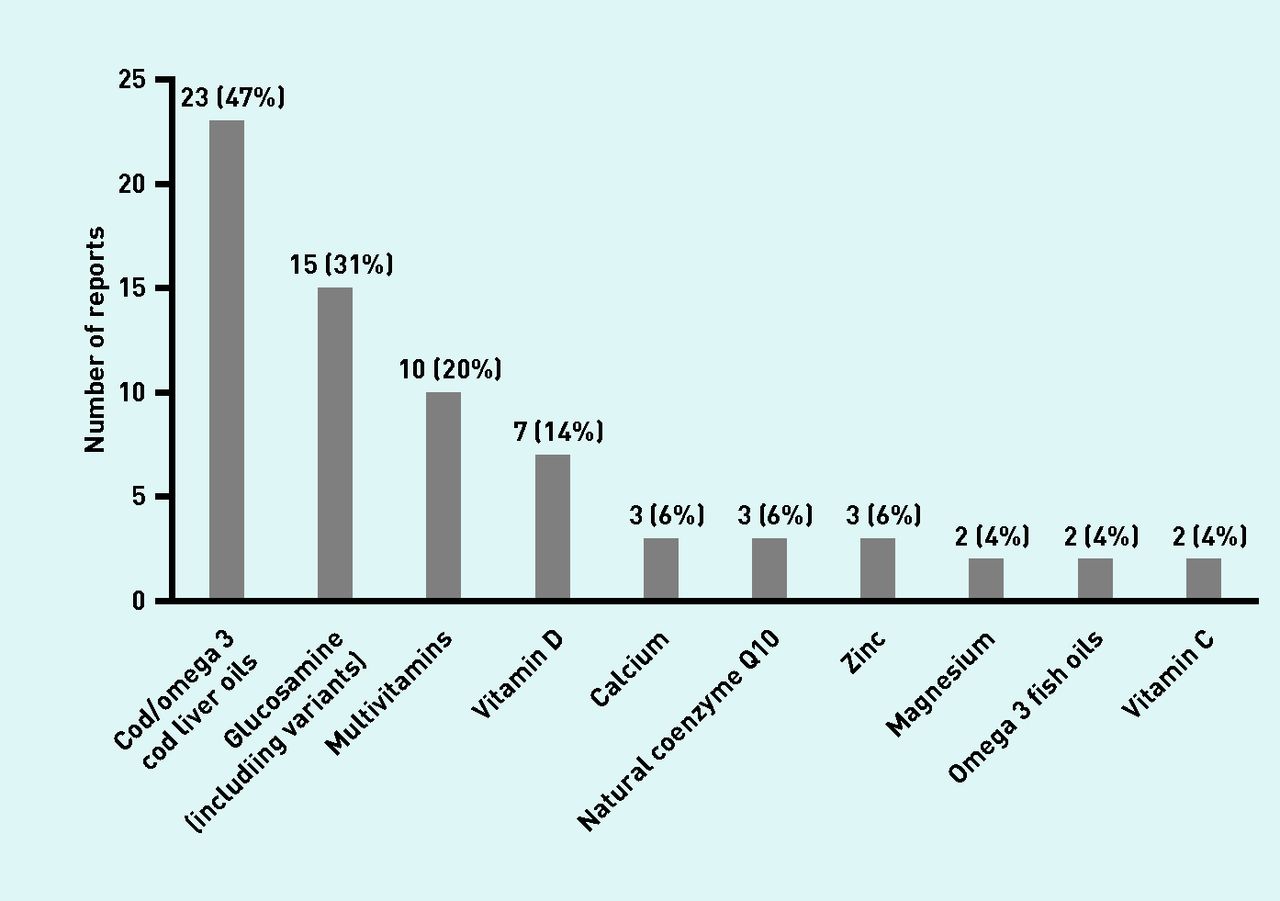
The majority of concurrent users (39; 78.0%) were taking dietary supplements, including vitamins and minerals. The most combined dietary supplements were cod liver oil, glucosamine, multivitamins, and vitamin D (Figure 2). Of the 50 concurrent users, 13 (26.5%) reported using both HMPs and dietary supplements concurrently with prescription drugs: 38.8% of concurrent users used ≥3 HMPs or dietary supplements concurrently with prescription drugs.

{kind=link}
{kind=link}
Supplements that are most frequently used concurrently with prescription by UK older adults. Percentages sum to more than 100% as individuals could report more than one HMP.
Potential interactions between HMPs, dietary supplements and prescription drugs
Just over half of the 55 herb–drug and supplement–drug combinations (n = 28, 50.9%) were assessed as ‘no interaction’ or ‘no interaction of clinical significance’. However, 21 combinations were categorised as interactions with ‘doubts about the outcome of concurrent use’. Three combinations were rated as ’potentially hazardous’ and three of ‘significant hazard’ (Box 1).
Evaluation of potential interactions from HMPs, dietary supplements, and prescription drugs
| HMPs/dietary supplement | Prescription medicine [number of patientsa] | Possible interactionsb |
|---|---|---|
| HDI category: Significant hazard, dosage adjustment or close monitoring is needed | ||
| Bonecal (Pharmanutra) | Levothyroxine | The efficacy of levothyroxine has been reduced by calcium carbonate. Calcium acetate and calcium citrate reduced levothyroxine absorption in pharmacokinetic studies |
| Peppermint | Lansoprazole | Antacids may compromise the enteric coating of some commercially available peppermint oil capsules. H2-receptor antagonists and proton pump inhibitors may interact similarly |
| St John’s wort | Amlodipine | St John’s wort significantly reduces the bioavailability of verapamil. Other calcium channel blockers would be expected to interact similarly |
| HDI category: A potentially hazardous combination | ||
| Glucosamine | Metformin | In a controlled study, glucosamine supplements with chondroitin had no effect on glycaemic control in patients taking oral antidiabetic drugs, but increases in blood glucose concentrations have occurred in patients with treated and untreated diabetes |
| Omega 3 fish oil | Bisoprolol [2] | The hypotensive effect of propranolol might be enhanced by fish oils |
| Ginkgo | Rabeprazole | Ginkgo modestly reduces omeprazole levels. Most other proton pump inhibitors are likely to be similarly affected |
| HDI category: Doubt about outcome of concurrent usec | ||
| Omega 3 fish oil | Aspirin [2] | The concurrent use of aspirin and fish oils caused at least additive effects on bleeding time in healthy subjects, but clinical studies in patients taking aspirin alone and with clopidogrel have found no evidence of an increase in incidence of bleeding episodes |
| Cod liver oil | Aspirin [2] | The concurrent use of aspirin and fish oils caused at least additive effects on bleeding time in healthy subjects, but clinical studies in patients taking aspirin alone and with clopidogrel have found no evidence of an increase in incidence of bleeding episodes |
| Cod liver oil | Bisoprolol Propranolol | The hypotensive effect of propranolol might be enhanced by fish oils |
| Flaxseed | Rivaroxaban | Limited evidence suggests that flaxseed oil may have some antiplatelet effects, which could be additive with those of conventional antiplatelet drugs, and increase the risk of bleeding with anticoagulants |
| Green tea | Lisinopril | Both black and green tea might cause a modest increase in blood pressure, which might be detrimental to the treatment of hypertension. Green tea reduced the effects of nadolol on blood pressure in healthy subjects |
| Senna pods | Indapamide | Theoretically, patients taking potassium-depleting diuretics could experience excessive potassium loss if they also regularly use, or abuse, anthraquinone-containing substances such as senna |
| Glucosamine | Co-codamol Paracetamol | Limited evidence suggests that glucosamine might reduce the efficacy of paracetamol (acetaminophen) |
| Glucosamine | Furosemide Bendroflumethiazide [2] | Limited evidence from a large open study suggests that unnamed diuretics might slightly reduce the efficacy of glucosamine to some extent |
| Echinacea | Midazolam | Echinacea does not appear to alter the AUC and clearance of oral midazolam, although the bioavailability may be increased. Clearance of intravenous midazolam may be modestly increased in patients taking Echinacea |
| Hawthorn | Nifedipine | Limited evidence suggests that there may be additive blood pressure-lowering effects if hawthorn is taken with conventional antihypertensives, but the effects are small |
| Visionace® (Vitabiotics) (lutein, carotenoids, myrtillus, flavonoid compounds) | Lansoprazole | The desired effect of betacarotene supplementation may be reduced in those taking proton pump inhibitors |
| Evening primrose oil | Aspirin | Evening primrose oil can inhibit platelet aggregation and increase bleeding time. It has therefore been suggested that it may have additive effects with other antiplatelet drugs, but evidence of this is generally lacking |
↵a The number of patients exposed to the particular combination of HMPs/dietary supplement and prescription drug.
↵b Potential interaction reports from Stockley’s Herbal Medicines Interactions.
↵c Guidance about possible adverse effects and/or some monitoring may be needed. AUC = area under the curve. HDI = herb–drug interaction. HMP = herbal medicinal product.
The HMPs implicated in the potential risk for interaction include:
flaxseed;
evening primrose oil;
St John’s wort;
peppermint;
senna;
Echinacea;
hawthorn;
green tea; and
ginkgo.
The five dietary supplements implicated are:
glucosamine;
cod liver oil;
omega 3 fish oil;
calcium carbonate; and
a multivitamin.
A majority of the identified interactions involved potential alterations in the concentration or effect of the prescription drugs, including calcium channel blockers, HMG-CoA reductase inhibitors (statins), and aspirin. The seven herb–drug and supplement–drug interactions assessed as having the potential for hazardous outcomes relate to increase in blood glucose concentrations, risk of bleeding, and reduced efficacy or bioavailability of the prescription drug.
DISCUSSION
Summary
Almost one-third of older adults (33.6%) in this study’s sample were using an HMP or supplement concurrently with prescription drugs. About one in three concurrent users was at risk of a potential herb–drug or supplement–drug interaction. If applied to the UK population that would mean 1.3 million older adults in the UK are at risk of at least one potential herb–drug or supplement–drug interaction. Importantly, six combinations (Box 1) have potential for hazardous outcome or significant hazard.
Strengths and limitations
To the authors’ knowledge, this is the first UK study in over 10 years assessing concurrent use of prescriptions, HMPs, and dietary supplements among older adults.13 The study participants were community-dwelling older adults recruited from general practices; previous UK studies have researched patients with cancer,19 diabetes,20,21 and pregnant women.22
A response rate of 39% is disappointing but high for a study of this kind and enough to provide credible findings. Examples of HMPs and dietary supplements were included in the questionnaire. It is possible that some participants did not consider products such as garlic or ginger used for medicinal purposes as HMPs and did not report them.
Comparison with existing literature
The prevalence of concurrent prescription, HMPs, and supplement use among older adults varies from country to country, between 9% and 88.3%.23–33 The prevalence of 33.6% reported in this study is similar to studies in North America.23 However, lower prevalence of 15%27 and 22.8%28 were reported in two other US studies. Variation in prevalence could be explained by different definitions and inclusion criteria for HMPs and level of detail required about HMPs. Not all studies focused exclusively on older people and some were more successful in recruiting people from BAME backgrounds.
Another possible explanation for discrepancies in prevalence of concurrent use in this study and those in the literature may be problem of recall. Some studies asked participants to recall products using self-completed questionnaires.13,28–30,34 Others interviewed face-to-face, checked and recorded medications.26,27,31,35,36 Some patients do not consider HMPs and dietary supplements as medicines. Even when questioned, they may not always remember to disclose them. This highlights the need for direct questioning and for healthcare practitioners to ask about use of those HMPs and supplements by name, which this research has shown to be most at risk of interactions.
All older adults in the study sample were using at least one prescription drug; the range of prescription drugs was similar to those reported by older adults in a previous US study.37 The number of prescription drugs taken ranged from 1 to 18, with 35% of the sample taking ≥5 prescription medications. This is consistent with findings of a study among US adults38 and UK data.39 The number of HMPs and supplements used by the study participants ranged from 1 to 8, and unexpectedly almost half of the concurrent users were using ≥3 HMPs and supplements.
Certain demographic and clinical characteristics are associated with concurrent medicine use. Females,13,36 older age groups,35 people with chronic conditions such as diabetes and high blood pressure,3,31 people with less than high school education,31,40 and people on low income40 are more likely to be concurrent users. The finding that 43.4% of females were concurrent users compared with 22.5% of males confirms previous findings that women tend to use more herbal and dietary supplements.13,14,36 The increased odds for a co-user to be female (34% versus 18%, P = 0.001) has been previously reported.34 This is likely to be for many reasons: women generally tend to live longer than men,41,42 they are the main carers for children and older people,43 tend to buy medicines and remedies for the home, and also tend to use more weight-loss products than men.44
Age was not significantly associated with concurrent use in this study, and in two other similar studies.31,32 However, concurrent use was highest among the participants in the age group 65–74 years (34.9%) but declined among those ≥85 years. Arcury et al 45 reported significant association between age and use of herbal remedies but observed a similar trend of decreased use among those aged ≥75 years.
Implications for practice
This research has highlighted potential risk of interactions with certain combinations of prescription drugs, HMPs, and dietary supplements. Therefore, healthcare professionals should routinely ask questions regarding use of other medications that are not prescribed. The problem with recall and what patients think are HMPs or supplements or not needs to be addressed. There are stages in the process of prescribing and dispensing that could also be optimised, such as, printing a warning on prescriptions or looking at counselling given by pharmacists on dispensing. Targeted questioning about use of any alternative medicine or supplements could initiate conversations about wider HMP use and possible interactions. Liaising with community pharmacists could also raise awareness of a potential problem, particularly for older people on warfarin and statins.
Acknowledgments
The authors thank all the patients and general practices that participated in this study. The authors also thank the Patient in Research Group (PIRg) of the Centre for Research in Public Health and Community Care (CRIPACC), for reviewing and suggesting changes to the study protocol, questionnaire, and participant information sheets.
Notes
Funding
No sources of funding were used to assist in the conduct of this study or the preparation of this article.
Ethical approval
Ethics review and support were obtained from the London — Hampstead Research Ethics Committee (15/LO/1870).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received May 8, 2018.
- Revision requested June 2, 2018.
- Accepted July 8, 2018.
- © British Journal of General Practice 2018
This article is Open Access: CC BY-NC 4.0 licence (http://creativecommons.org/licences/by-nc/4.0/).
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

