


Abstract
Background Polymyalgia rheumatica (PMR) is one of the most common inflammatory arthritic disorders seen in older individuals. Most patients with PMR are diagnosed and managed exclusively in general practice, yet primary care-focused research is lacking.
Aim To identify and explore the challenges of diagnosis and management of PMR in general practice.
Design and setting A multi-methods study in UK primary care.
Method The multi-methods study comprised two complementary studies: a national questionnaire survey of 5000 randomly selected GPs from across the UK; and a qualitative semi-structured telephone interview study of UK GPs. Simple descriptive statistics were used to analyse questionnaire data. A thematic approach was used to analyse verbatim transcripts of the GP interviews.
Results In total, 1249 (25%) GPs responded to the questionnaire survey. From this total, 24 GPs were interviewed for the qualitative study. Features used by GPs to identify PMR were largely in line with current guidance. Diagnosis was found to be challenging, with GPs relying heavily on response to treatment with glucocorticoids. Investigations advised by current British PMR guidance to attempt to rule out other causes for symptoms were not routinely requested. Concerns surrounding ongoing treatment with glucocorticoids were widespread in relation to both potential adverse effects and ongoing monitoring.
Conclusion Focused strategies to investigate and therefore exclude non-PMR differential diagnoses are required for patients with new-onset suspected PMR symptoms. Additionally, ongoing active review for alternative causes for symptoms as well as vigilance for treatment complications needs to be implemented.
INTRODUCTION
Most patients in the UK with polymyalgia rheumatica (PMR) are diagnosed and managed exclusively by their GP.1,2 This is also the case in other countries where PMR has a significant prevalence.3 Bilateral shoulder and/or hip pain, stiffness, and muscle aches are classical features alongside raised inflammatory markers.4 It is rare in individuals <50 years of age and carries a lifetime risk of 2.4% in females and 1.7% in males,5 and, as reported by patients with PMR, can cause significant pain and disability often impacting on daily function and activity.6 Given that people are working and living longer, the prevalence of PMR is set to rise and its impact on society will become more significant.
However, the presentation of PMR can be highly variable, non-specific (especially in early disease), atypical,7 and the symptoms of PMR have a wide differential diagnosis.4 Additionally, patients in the typical PMR age range often suffer with multimorbidity, further adding to the diagnostic challenge,8 which, given no gold standard diagnostic test, means that potential for misdiagnosis is significant with some studies suggesting that GP diagnostic accuracy is around 50%.9 Previous research would also suggest that routine management of potential treatment adverse effects, for example osteoporosis, is not routine practice in primary care.2
Guidance for the identification and management of PMR has been developed and is freely available.4,10,11 In order to improve diagnosis and care for patients with PMR a greater understanding of the challenges and barriers faced by clinicians making the diagnosis and managing this, often neglected, condition is needed. A multi-methods approach was taken to create a more complete description of the study question,12 especially given that in settings like general practice multiple influences (such as early presentation, multimorbidity, local guidance) may impact diagnosis and management of illnesses.
METHOD
A national cross-sectional postal questionnaire survey of 5000 randomly selected UK GPs, identified from Binley’s database (now Wilmington healthcare (https://wilmingtonhealthcare.com/)), was undertaken. This large database contains the names and addresses of GPs working in the UK. In addition, it contains information on the type of practice, the practice population size, practitioner seniority, and some of the clinical services that they provide.13 The questionnaire could also be completed online. Non-responders were sent reminders by post after 2 weeks and 4 weeks. Responders to the survey were used as a sampling frame for a subsequent qualitative semi-structured telephone interview study of GPs from across the UK. Participants were purposively sampled in relation to years of clinical experience as a GP, sex, and seniority. Questionnaire findings contributed to the development of the topic guide for the interview study.
How this fits in
Polymyalgia rheumatica (PMR) can be a challenging illness to diagnose and manage, and the majority of patients with PMR are diagnosed and managed exclusively in general practice. However, most of the research previously conducted has been in secondary care settings. This study uses multiple methods to describe the diagnostic and PMR management practices of UK GPs, and highlights associated challenges and areas where changes could be made to improve outcomes for patients with this debilitating illness.
Survey questionnaire
A questionnaire was developed that built on findings from previously published work examining GP diagnosis and management of PMR2 and UK national PMR guidelines.4 Domains included questions relating to GP diagnosis, management, and any related challenges. Additionally, baseline demographics, participants’ role, experience, and characteristics of the practice that they worked in were requested. The questionnaire also incorporated evidence-based methods shown to improve questionnaire response.13,14 An incentive to win a bottle of champagne was given as this approach has been shown to be particularly effective in improving response rates.15 A reminder card was sent after 2 weeks and a further questionnaire after 4 weeks if no response was received. The questionnaire underwent a process of review and refinement by local clinicians (five GPs, two rheumatologists, and patient and public involvement) who provided input into the content, face validity, and flow of the questionnaire but did not take part in the main study.
Interview study
Semi-structured telephone interviews were undertaken with GPs who had completed the questionnaire survey and had agreed to further contact. To reflect a broad range of relevant practitioner experience, participants to the interview study were purposively sampled based on years of clinical experience as a GP (around 11 years, the median years of experience reported in the survey), sex, and clinical role: locum doctor, partner, or salaried doctor.
Topic guide
The topic guide for the qualitative study was informed by findings from the cross-sectional survey and relevant areas of interest from the wider PMR literature. This was reviewed and refined with feedback from GPs, rheumatologists, and qualitative researchers. As transcripts were reviewed, the topic guide was modified to focus on themes that emerged from the interviews.
Data analysis
The survey contained fixed and/or closed-response questions and open-response questions. Simple descriptive statistics were generated using SPSS (version 22) for fixed and/or closed response questions. For open-response questions thematic content analysis was used.16
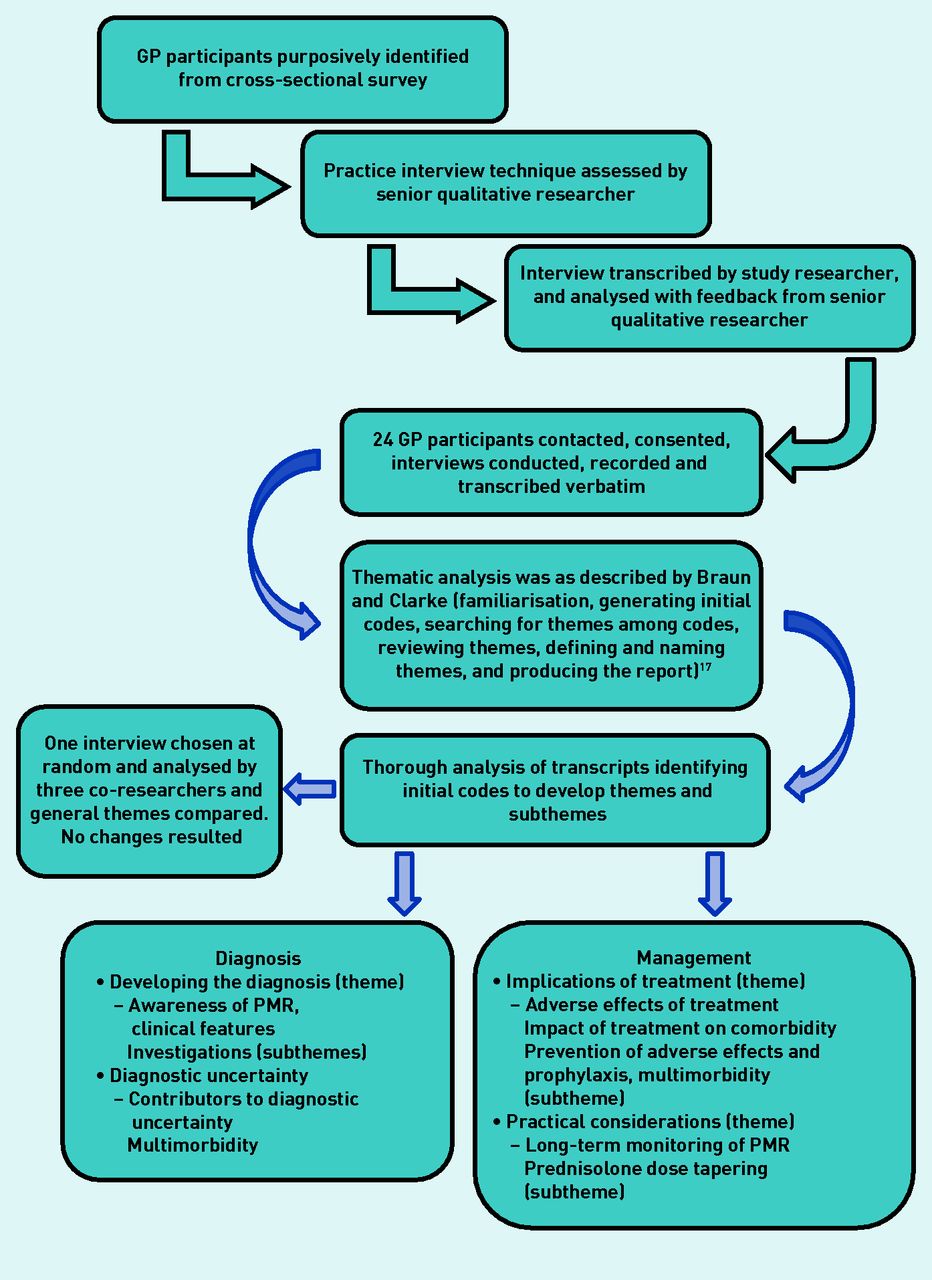
Interviews were audiorecorded and transcribed verbatim using an approved transcription company. Thematic analysis was used to analyse transcript data using the six phases described by Braun and Clarke (familiarisation, generating initial codes, searching for themes among codes, reviewing themes, defining and naming themes, and producing the report).17 One researcher performed the analysis and three others independently analysed a randomly selected transcript to identify general themes to compare with the first researcher’s findings. No changes resulted from this exercise. The qualitative study method is summarised in Figure 1.
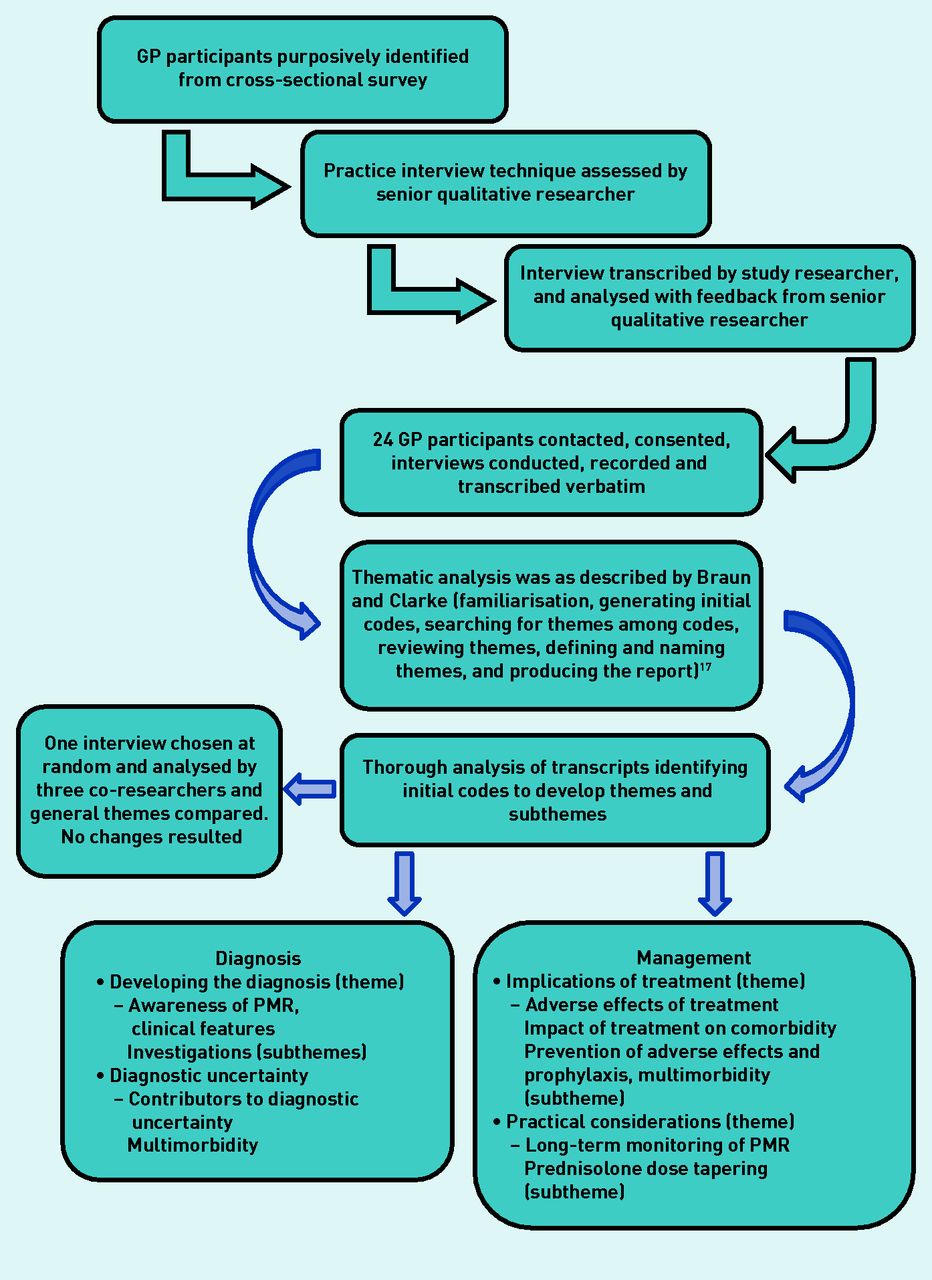
Summary of the qualitative telephone interview study. PMR = polymyalgia rheumatica.
RESULTS
A total of 1132 questionnaires were returned by post; 126 were completed online, and nine were duplicates (eight online, one postal). The overall response was 25% (1249 completed questionnaires). Table 1 illustrates the baseline characteristics of responders and non-responders based on data provided by Binley’s. There were 24 GPs interviewed for the qualitative telephone interview study.
Baseline characteristics of responders and non-responders
Diagnosis
Of the responders, 72% (n = 906) would exclude PMR in patients <50 years of age and rated most highly bilateral shoulder pain, raised inflammatory markers, and response to initial treatment with glucocorticoids as typical features of PMR. Muscle pain, morning stiffness, and hip girdle pain were also rated as important (Figure 2). Erythrocyte sedimentation rate (ESR) remained the inflammatory marker of choice (requested by 89%, n = 1118), although just over half of these (55%, n = 683) responders requested C-reactive protein (CRP). However, contrary to current UK guidance4 half indicated that they would offer a treatment trial if the inflammatory markers were normal and just over one-third of responders would exclude PMR as a potential diagnosis in this scenario.

Radar plot depicting median scores relating to GP rating of importance of presenting clinical features used to diagnose polymyalgia rheumatica.
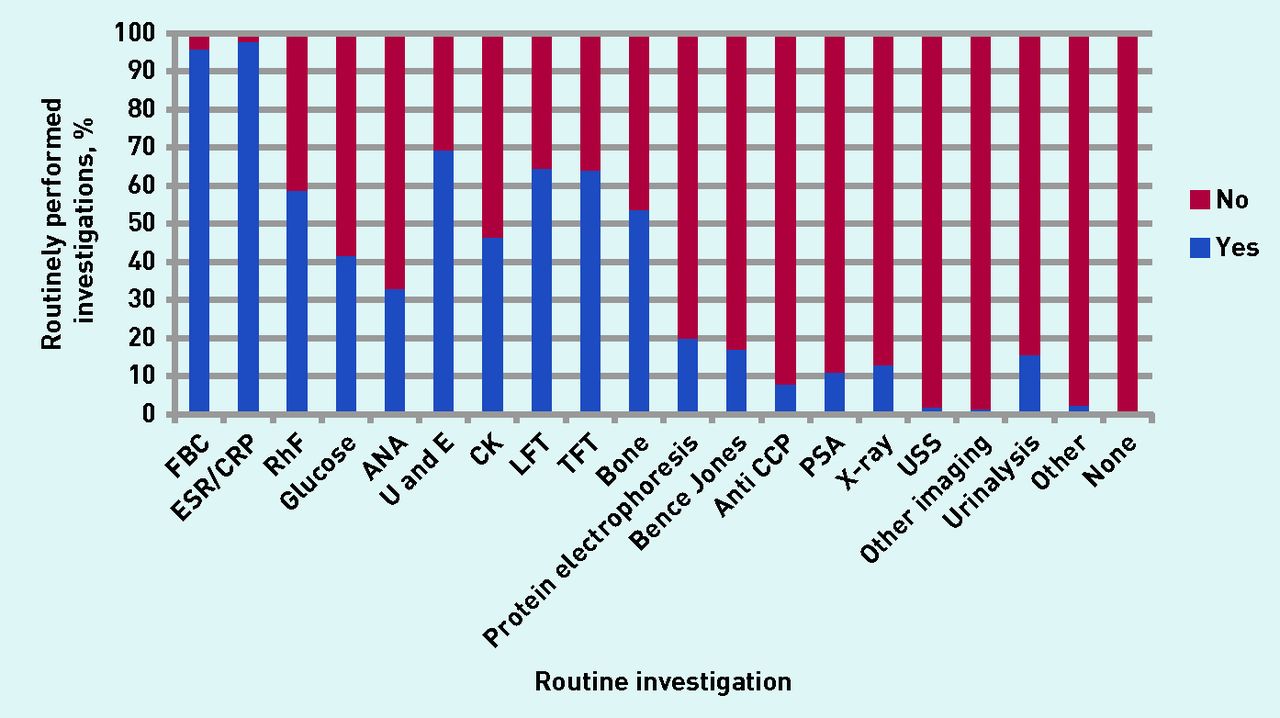
Full blood count and inflammatory markers were universally requested by responding GPs. However, other British PMR guideline-advised investigations to attempt to rule out other causes for symptoms were less routinely requested: urea and electrolytes (69%), liver function test (64%), bone analysis (54%), protein electrophoresis (20%), thyroid function (64%), creatinine kinase (46%), rheumatoid factor (59%), and anti-nuclear antibodies (33%).4 These results are summarised in Figure 3. Guidance also advises on core exclusion criteria for PMR: exclusion of giant cell arteritis, exclusion of infection, and exclusion of malignancy as a cause for symptoms. Eighty per cent of GPs reported that they would exclude giant cell arteritis as a cause for symptoms, 66% reported excluding infection, and 55% reported trying to exclude malignancy as a cause for symptoms.
{kind=link}
{kind=link}
{kind=link}
GP-reported routinely performed investigations for patients with suspected PMR. ANA = anti-nuclear antibodies. Anti CCP = anti-citrullinated protein antibody. CK = creatinine kinase. CRP = C-reactive protein. ESR = erythrocyte sedimentation rate. FBC = full blood count. LFT = liver function test. PSA = prostate-specific antigen. RhF = rheumatoid factor. TFT = thyroid function test. U and E = urea and electrolytes. USS = ultrasound scan.
Analysis of open-response questions identified two predominant themes relating to challenges associated with diagnosis. First, there were challenges surrounding atypical presentations, for example, a classical history but normal inflammatory markers or poor response to initial treatment with glucocorticoids. Second, there was the vague and non-specific way in which PMR can sometimes present clinically, especially given the greater age of patients with PMR, with wide differential diagnosis of possible mimicking disorders and associated high levels of multimorbidity in the age range typical of PMR. These two factors coupled with a lack of specific diagnostic testing for PMR contributed significantly to ongoing anxieties relating to diagnostic uncertainty.
The qualitative study reinforced the diagnostic challenges found in the cross-sectional survey. Two main themes were identified. The first, ‘developing the diagnosis’, related to how patients present and how GPs may identify and diagnose patients with PMR, with response to initial glucocorticoid treatment being specifically highlighted by interviewees as a common and important contributing feature for a PMR diagnosis. The second theme, ‘diagnostic uncertainty related to a range of factors affecting diagnostic confidence’. These two themes are inherently connected. There was clear recognition that PMR affected patients’ lives and function significantly:
‘It wrecks lives doesn’t it? You get people that are, kind of, you know, really active, and then all of a sudden they’ve got this awful thing.’
(GP22, 15 years [number of years as qualified GP], male [M], partner [P])
However, the GPs interviewed acknowledged that the diagnostic process for PMR was complex and not always typical:
‘I’m probably more inclined to refer now. I’ve actually seen two people recently who I’ve referred […] who had reasonably convincing symptoms but their inflammatory markers were entirely normal. They fitted the right demographic and their symptoms were quite convincing but I wasn’t convinced enough.’
(GP13, 5 years, Female [F], Salaried [S])
A broad spectrum of experience was found among the GPs interviewed. Participants indicated that they were responsive to individual clinical presentations and aware of the variety of ways in which patients with PMR can present:
‘I think the majority of the time people do come in with what’s described as the classic symptoms […] I suppose there are then people who come in with much more generalised non-specific aches and pains, and it can then take a little bit longer for PMR to come to the forefront of your mind when seeing them.’
(GP13, 5 years, F, S)
Accounting for the impact of multimorbidity as a confounding factor when making a diagnosis was a key area identified, as was concern about missing differential diagnoses such as other rheumatic disorders or malignancy:
‘And also ruling out other causes. I had a patient a few years ago who presented with really barn-door polymyalgic symptoms […] improved within a couple of days of the steroids. But it seemed that she had a, sort of, paraneoplastic thing. She actually had a — oh, what do you call it? A 5HIAA secreting tumour, serotonin-secreting tumour.’
(GP21, 7 years, F, S)
Guidelines can potentially be over-simplistic, giving the impression of a standard phenotype for PMR that is easily recognisable. For PMR, however, and especially in general practice, patients may present early in the disease course, and so multiple consultations are often required to build a diagnostic picture using a variety of clinical and laboratory features based on both experience and guidance. Additional verbatim quotations relating to diagnosis from both the survey and qualitative study are shown in Appendix 1.
Management of PMR
There are two key areas of primary care management of PMR: initial treatment with glucocorticoids and long-term treatment encompassing glucocorticoid dose reduction as well as identification, prevention, and management of potential adverse effects of glucocorticoid treatment. The median initiating dose of prednisolone among survey responders was found to be 20 mg with a most frequent initiating dose of 15 mg. Just over half, 56.4% (n = 704), of responders would initially treat PMR as per UK guideline recommendations4 with either 15 mg or 20 mg of prednisolone.
Glucocorticoid dose reduction was identified as the main challenge associated with long-term treatment of PMR. This was closely followed by the potential adverse effects of long-term glucocorticoid use. Bone protection was routinely offered by 81% (n = 1016) of responders whereas gastric protection was offered by 69% (n = 860). Responders indicated that referral for specialist review was undertaken mostly in cases of diagnostic uncertainty (poor response to initial treatment with glucocorticoids) (79.3%, n = 991), young patients (43.5%, n = 543), and for those with normal inflammatory markers (31.9%, n = 399).
The predominant theme identified from the qualitative study surrounded the ‘implications of treatment’, with a second recurring theme ‘practical considerations’ relating more to pragmatic aspects of treating patients with PMR. It was clear from the interviews that there are significant concerns surrounding the long-term treatment of patients with PMR. This relates mainly to the potential adverse effects associated with glucocorticoids and, given that this is currently the only proven effective treatment option available to GPs, it represents an area of significant challenge.
A variety of approaches to ongoing management was undertaken and volunteered by participants. Initial treatment is often very effective, with patients having a significant and rapid improvement in most of their symptoms. However, ongoing treatment becomes more challenging and has to be negotiated in order to balance the beneficial effects of the treatment (improved function and/or less pain) against potential adverse effects, which become more prevalent with duration of treatment and may need additional treatment to prevent or manage:
‘Yes. If I’m going to be committing someone to a long course of steroids, I will often start them on a PPI, to prevent them from getting gastrointestinal side effects. And, also, I often start them on a bisphosphonate as well, providing they’re able to tolerate it, and calcium supplements.’
(GP22, 15 years, M, P)
The GPs interviewed tended to take a shared-management approach that was individualised for each patient. GPs were aware of how the treatment could affect their patients given any coexisting morbidity and multipharmacy:
‘In terms of starting steroids, people in most cases don’t seem too resistant to that idea initially. I suppose it’s because they’re in pain and they think it’ll make them better. It’s later on, when they’re on them and getting side effects, that they have more concerns about it […] Yes, I’ve certainly got a lady who developed diabetes for the first time while she was on steroids.’
(GP13, 5 years, F, S)
They were also balancing confidence in the patient and the patient’s own ability to self-manage their illness:
‘So, if the patient is sensible I’ll explain to them what I’m expecting to do with the reduction and often will then only follow them up, you know we have people book phone appointments and I’ll tell them to book a phone appointment every 8 weeks after an intervening reduction’
(GP16, 17 years, M, P)
However, compliance with treatment titration was recognised as a challenge, with patient fears relating to the return of their symptoms in addition to patients often attributing a variety of symptoms, rightly or wrongly, to their PMR:
‘Yeah, oh definitely and then you try and get them off them and they get, I don’t know it seems to me that they get very attached to the steroids in a funny way and they, if they start to ache again they come back and say oh I think I should increase my steroids which is maybe the right thing to do but it’s just, as I say, woolly.’
(GP17, 11 years, F, P)
Additional verbatim quotations relating to management from both the survey and qualitative study are shown in Appendices 1 and 2.
DISCUSSION
Summary
This is the first UK national study investigating PMR in primary care where the majority of PMR diagnosis and management occurs,1,2 and as such it makes a needed contribution to the literature.
Strengths and limitations
The main strength of this study relates to the use of a multi-methods approach that has created a large national dataset of quantitative and qualitative data. This has provided an in-depth understanding of the issues faced by GPs diagnosing and managing PMR in the community. The main weakness of this study was the suboptimal response and, therefore, the potential lack of generalisability of data. However, a response rate of 25% is comparable with similar musculoskeletal GP surveys conducted by the authors’ own research institute,18 and, although a low response rate may increase the probability of bias, responder demographics of the questionnaire study relating to age, sex, and GP role were comparable with national GP demographics.19 Accessing non-responders to surveys remains a significant challenge and, as discussed in the Method section, techniques shown to try to enhance response rates were employed in this questionnaire survey. Other methods that have been shown and could have been used to improve response include enclosing monetary or voucher incentives irrespective of completion of the survey, as does pre-notification of a study.20 However, given the size of the survey, significant additional funding would have been required to undertake these methods and there is evidence suggesting that engagement in research surveys in general practice may be declining.21 A further weakness relates to the questionnaire used for this study, which was designed specifically to investigate the primary care diagnosis and management of PMR but did not use predetermined and validated items or instruments. Although piloted among patients and clinicians, no formal validation testing of the questionnaire was undertaken.
Undertaking a qualitative study, in combination with the survey, has enabled an in-depth exploration of areas of interest and importance identified from the survey. This is important in an area where limited previous research exists and has added more detailed clarification of the challenges associated with PMR in primary care. Limitations of the qualitative study include method of interview and analytical issues influencing findings. Telephone interviews allowed participants to be conveniently interviewed from across the UK, allowing a wide range of experiences from different areas of the country, but are often criticised for lack of rapport building and appreciation of non-verbal communication. However, developments in internet technology and accessibility to applications such as Skype and Google Hangouts will become commonplace and allow face-to-face interaction while conducting studies remotely. These factors are unlikely to have impacted on the quality of data given the probable highly motivated status of participants, who were potentially interested in the subject, and it was clear that participants often had a certain level of ‘PMR intelligence’ or significant experiences relating to PMR that they wanted to voice, as well as the very clinical nature of the questioning. Analysis was undertaken by a single researcher, which has the potential to affect theme development due to preconceptions and misinterpretations; however, an inter-rater analysis was undertaken to improve trustworthiness and reliability of developed themes. Qualitative methods do not seek to create generalisable findings but aim to gain the richest possible data from the participants interviewed, thus, the resulting participants’ experiences of PMR in the qualitative study allowed a thorough exploration of a wide range of challenges that PMR poses in primary care.
Finally, there was also the potential for disparities to exist in reported behaviour and actual behaviour with survey and qualitative methodologies. For example, survey data in this study suggested that GPs were reporting using typical features to identify patients with PMR, yet a clinical records review would suggest that GPs may not be adhering to published criteria.1 Additionally, GPs responding to the present survey offered prophylactic medication more regularly than research using consultation databases would suggest,2 perhaps reflecting that those responding to the questionnaire were more likely to be interested in the condition and thus be aware of current guidance.
Comparison with existing literature
This study represents the first study specifically aimed at investigating the challenges and barriers of PMR diagnosis and management in general practice. Additionally, very few studies have been carried out in this setting and so comparisons with existing literature are limited.
Despite emerging evidence on the role of biomarkers and imaging, making an accurate diagnosis of PMR is still dependent on identifying the classical cluster of clinical signs and symptoms described in published classification criteria22 coupled with an active exclusion of other causes for symptoms.4 Although GPs reported using well-recognised features of PMR to make a diagnosis, they found diagnosis challenging, especially with atypical presentations. Guidelines can potentially be over-simplistic, giving the impression of a standard phenotype for PMR that is easily recognisable. However, for PMR, and especially in general practice, patients may present early in the disease course and so multiple consultations are often required to build a diagnostic picture using a variety of clinical and laboratory features based on both experience and guidance. Misdiagnosis was a key concern (estimated 24–50%)9,23 with GPs anxious about alternative, and more sinister, diagnoses and the implications of inappropriate treatment with glucocorticoids. Despite this, an adequate formal exclusion of alternative diagnoses does not appear to be routine in UK primary care, representing a missed opportunity to potentially improve diagnostic accuracy. Likewise, requesting the full range of investigations that are suggested in current guidance4 prior to making a diagnosis of PMR was not routine. However, excluding conditions that may mimic PMR symptoms can be challenging, particularly in the early stages of disease, for example, cancer or rheumatoid arthritis. Additional investigations may not be adequate to completely exclude alternative causes for symptoms, with current PMR guidance making no provision for multimorbidity.
Guidance on glucocorticoid treatment is conflicting, with different clinical guidelines providing different advice.4,11 Furthermore, guidance is based largely on expert secondary care consensus, rather than on high-quality research evidence. Recently published guidance from the European League Against Rheumatism (EULAR)/American College of Rheumatology (ACR) advocate, using a minimum effective initiating dose of glucocorticoid of 12.5–25 mg of prednisolone equivalent, with the precise dose being guided by the presence of other morbidities, risk of relapse, and risk of adverse effects.11 Such a wide dosing range is likely to cause confusion rather than reassurance to GPs. What is clear, however, is that 40% of responders to the questionnaire postal survey indicated that they were initiating patients with PMR on doses of prednisolone of >30 mg, a level that is highlighted in guidance as being inappropriately high.11 It is unclear why higher doses of prednisolone are being used. A hallmark of PMR is its responsiveness to low/medium-dose glucocorticoids; higher doses have the potential to treat a wider scope of inflammatory illnesses and therefore increasing the possibility of misdiagnosis. In addition, higher doses of glucocorticoids have been shown to be associated with more adverse effects, for example, osteoporotic fractures.24 Additionally, findings in the present study demonstrate that, contrary to current UK guidance,4 half of the responders indicated that they would offer a treatment trial for patients who have features of PMR but with normal inflammatory markers, yet these types of scenarios were a significant area of challenge for GPs. Studies have shown that normal inflammatory marker are seen in 7–22% of patients25 and, although a good response to glucocorticoid treatment can improve diagnostic accuracy and consistency with PMR,4,9 it has also been demonstrated that a response to glucocorticoid treatment does not increase the accuracy of current provisional PMR classification criteria.26
For long-term management, although the recent EULAR/ACR guidance11 does not discuss glucocorticoid prophylaxis, GPs appear to be providing prophylaxis based on patient need and an assessment of comorbidity and associated risk factors. This remains an area where further research is needed to clarify the magnitude of risk of long-term low-dose glucocorticoid treatment and evidence-based indications to identify high-risk patients in need of active prophylactic treatment or consideration of glucocorticoid-sparing agents.
Although many chronic diseases, such as diabetes and asthma, have well-formulated systems for ongoing medical review, this is not the case for patients with PMR, who frequently suffer from a lack of coordinated or structured follow-up. This not only impacts on treatment for PMR but also presents challenges for medication titration, and for active surveillance of both the disease, its sequelae, for example, coronary heart disease,27 and potential adverse treatment effects, including diabetes, hypertension, and osteoporosis.24 A more structured follow-up process with vigilant review for alternative diagnoses as a cause for symptoms, especially if new or unusual features emerge, coupled with careful glucocorticoid tapering, and active surveillance for common adverse effects could potentially improve outcomes for patients with PMR.
Implications for research and practice
This study suggests that PMR is challenging to diagnose and manage. However, there is opportunity to improve outcomes for patients with PMR in general practice by systematic diagnostic exclusion of other causes for symptoms and treating initially with guideline-suggested doses of glucocorticoids.4,11 Active vigilant follow-up for the development of other illnesses that may have been the cause of initial symptoms with appropriate screening and early prophylaxis, along with management of developing treatment-adverse effects, could improve care for patients with PMR. Future research would benefit from inclusion of patients with PMR from all settings, including primary care. Study findings can then be generalised to a primary care setting where the majority of patients in the UK are diagnosed and managed.1
Evidence on the optimal dosing regimen, and the associated titration in response to treatment, is largely based on limited, low-quality, secondary care trials. There continues to be a need for a large pragmatic trial recruiting patients with PMR from all clinical settings to provide GPs and specialists with the evidence needed to optimise the diagnosis and management of this group. Given the potential complications of initial overtreatment of PMR with prednisolone and the implications of a poor response if undertreated initially, the researchers of this study advocate an initiating dose of 15 mg of prednisolone as outlined in the current British Society for Rheumatology/British Health Professionals in Rheumatology guidelines.4
Additionally, the use of standard outcome measures28 and classification criteria26 would allow improved evidence synthesis and ensure more robust and relevant conclusions.
Acknowledgments
The authors are grateful for the participation of all of the GPs who responded to the questionnaire and gave up their precious time to participate in the telephone interviews. Special thanks go to Edward Jutsum and Antonia Middleditch for their help in interview and topic guide development. The authors also wish to thank the Research Institute for Primary Care and Health Sciences, Keele University, and the Keele administration and management teams who supported the study.
Appendix 1. Verbatim quotations obtained from qualitative study and open-response questions relating to diagnosis of PMRa
| Theme | Subtheme | Verbatim quote |
|---|---|---|
| Diagnosis | Awareness of PMR | ‘I think a lot of the time it’s much older people, and they’ve just, kind of, gone, “Well, it’s part of getting old. I’m a lot achier than I was this time last year”, and they don’t realise that it’s necessarily something we could perhaps help with.’ (GP23, 13 years, F, S) |
| ‘Well, I suppose, quite unusual, maybe the GPs aren’t aware of it. Or, you know, it’s not something that you see all the time …’ (GP8, 10 years, F, S) | ||
| Developing the diagnosis | Clinical features | ‘Typically, when they’re complaining of shoulder pain, and they say, “I’ve had real trouble washing my hair or brushing my hair.” And there’s difficulty with getting up out of the chair because of the leg pain, you know, the, sort of, ones that give you the high index of suspicion.’ (GP23, 13 years, F, S) |
| Investigations | ‘I mean obviously the cardinal things I’m looking for are raised inflammatory markers so CRP and the ESR would be the two that I would be sort of looking at. However I would be doing a full blood count […] renal function […] liver function […] HbA1C […] creatinine kinase. If there’s been any weight loss already or any other sort of slightly sort of more sort of red flag symptoms I’d be considering things like an autoimmune profile or myeloma screen, tend to do a chest X-ray at baseline when I’m starting with the steroids but earlier than that if there’s any other systemic features. (GP6, 20 years, F, S) | |
| Factors causing diagnostic uncertainty | ‘There is no diagnostic test so it’s a clinical diagnosis with suggestive blood results which can be hard to feel certain about and hard to convey convincingly to the patient, also there being lots of other conditions with similar presentations makes this even harder.’ (Participant 4814, 2 years, F, S) | |
| Contributors to diagnostic uncertainty | Multimorbidity | ‘I think it impacts at every stage, doesn’t it? It makes diagnosis harder because people often have conditions where symptoms overlap and so it makes it harder to assess. If their function is limited by something else then the usual things you might look for are already affected by their other things, so you can’t use your normal clues when going through their history. Often you see people who are on several other painkillers or who are maybe on steroids for something else, so it makes it difficult.’ (GP12, 15 years, F, S) ‘Often symptoms in older patients with multiple comorbidities, difficult sometimes to distinguish between any related symptoms including osteoarthritis and fibromyalgia.’ (Participant 1955, 17 years, F, P) |
| Disorders mimicking PMR | ‘Other things you know occasionally something else will be going on and kind of odd rheumatological things kind of I don’t know, where you’ve got cross over symptoms, vitamin D deficiency’s one that I’ve found where someone, we live in the west of the country which is a bit cloudier and white people are getting significant vitamin D deficiency who don’t go out very much and that can cause very similar symptoms. B12 deficiency again is something that I’ve picked up on the odd occasion and kind of I can’t think now what the, how that’s happened but I’ve certainly had to review the diagnosis.’ (GP16, 17 years, M, P) | |
↵a Identifiers in brackets after the quotes: GP followed by numeral = GPs who took part in the qualitative interview and their identifying number. Number of years = years as qualified GP. Participants followed by numeral = GPs who provided quotes from the survey. F = female. M = male. P = partner. S = salaried. CRP = C-reactive protein. ESR = erythrocyte sedimentation rate. HbA1C = glycosylated haemoglobin. PMR = polymyalgia rheumatica.
Appendix 2. Verbatim quotations obtained from qualitative study and open-response questions relating to management of PMRa
| Theme | Subtheme | Verbatim quote |
|---|---|---|
| Management | Lack of alternatives to glucocorticoids | ‘The lack of other options, really … and that nothing else does seem to work particularly well for it, and ‘you’re a little bit stuck if, for any reason, they can’t tolerate the steroids, and aren’t getting on with them. You are a little bit stuck with what else to suggest. Yes, it’s not exactly a nice option.’ (GP24, 12 years, F, S) |
| Implications of treatment | Adverse effects of treatment | ‘There’s just the sense of people that were quite well old people turning in to people who suddenly have a lot of problems and they’re on more medication and they’re just not as well at the end as they were at the beginning.’ (GP17, 11 years, F, P) |
| Prevention of adverse effects and drug prophylaxis Impact of treatment on existing comorbidity | ‘So, then I say “And here’s another tablet for you. I’m sorry.” “And, actually, here’s a PPI [proton pump inhibitor] as well.’” (GP 24, 12 years, F, S) | |
| ‘Oh, definitely, yes, their diabetes control, definitely. I mean, they’ve usually got type 2 diabetes […] so they don’t run into any crises, but definitely, their diabetes control gets worse.’ (GP 24, 12 years, F, S) | ||
| Practical implications of treatment and monitoring for PMR | Long-term monitoring of PMR | ‘Yes, again, sometimes people do get lost to follow-up, with all the will in the world, don’t they? So I had one lady who had been seeing me very regularly. We were bringing it [steroids] down. Something else cropped up with her, and she ended up, sort of, seeing somebody else for a while about another thing. And then she just had been left on this dose of prednisolone.’ (GP24, 12 years, F, S) |
| ‘Keeping follow-up and reduction in steroids, not enough appointments to bring patients back routinely, patients need to be aware of the treatment plan and be proactive if arranging tests and for symptom review.’ (Participant 3529, 5 years, F, S) | ||
| ‘Long-term steroid complications require careful and frequent follow-up, national and local guidelines and even within practice is muddled and lacks agreement, difficult access to secondary care, concerns they mix up diagnosis and timelines.’ (Participant 3927, 18 years, F, P) | ||
| Treatment dose tapering | ‘I mean, I like my PMR patients because they are fairly straightforward. There’s a kind of loose structure of reducing this drug, seeing how they respond. I will kind of go clinically; I don’t push them to have blood tests every month. I mean, it just seems pointless. I judge their response by symptoms, not inflammatory markers.’ (GP18, 22 years, M, S) | |
| ‘Main challenge is coming off steroids; most patients are completely delighted when their symptoms resolve after a week on steroids but become despondent and anxious when they start to experience steroid side effects (e.g. weight gain) and discover when they try to step down off their steroids their symptoms re-occur.’ (Participant 1665, 11 years, F, P) | ||
| ‘Frequent input with steroid regimens/doses especially when they struggled with dose reduction, no matter how slowly it was done — some patients feel dependent on steroids and will end up taking more (without consulting you) to control symptoms even when perhaps their symptoms might not be due to PMR.’ (Participant 818, 4 years, M, P) | ||
↵a Identifiers in brackets after the quotes: GP followed by numeral = GPs who took part in the qualitative interview and their identifying number. Number of years = years as qualified GP. Participants followed by numeral = GPs who provided quotes from the survey. F = female. M = male. P = partner. S = salaried. PMR = polymyalgia rheumatica.
Notes
Funding
This study was funded by an Arthritis Research UK Clinician Scientist Award to Christian Mallen. Christian Mallen is funded by the National Institute for Health Research (NIHR) Collaborations for Leadership in Applied Health Research and Care West Midlands, the NIHR School for Primary Care Research, and an NIHR Research Professorship in General Practice (reference number: NIHR-RP-2014-04-026). Toby Helliwell is funded by an NIHR Clinical Lectureship in General Practice and was funded by an NIHR In-Practice Fellowship and an NIHR School for Primary Care Research GP career progression award during the time that this research was undertaken. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health.
Ethical approval
The Keele University ethics review panel granted ethical approval for this study (reference for qualitative study: ERP178, reference for survey: ERP2206).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received December 22, 2017.
- Revision requested January 23, 2018.
- Accepted June 3, 2018.
- © British Journal of General Practice 2018
REFERENCES
In this issue









Jump to section
- Top
- Article
- Abstract
- INTRODUCTION
- METHOD
- RESULTS
- DISCUSSION
- Acknowledgments
- Appendix 1. Verbatim quotations obtained from qualitative study and open-response questions relating to diagnosis of PMRa
- Appendix 2. Verbatim quotations obtained from qualitative study and open-response questions relating to management of PMRa
- Notes
- REFERENCES
- Figures & Data
- Info
- eLetters
More in this TOC Section
Related Articles
Cited By...

