


Article Figures & Data
Figures
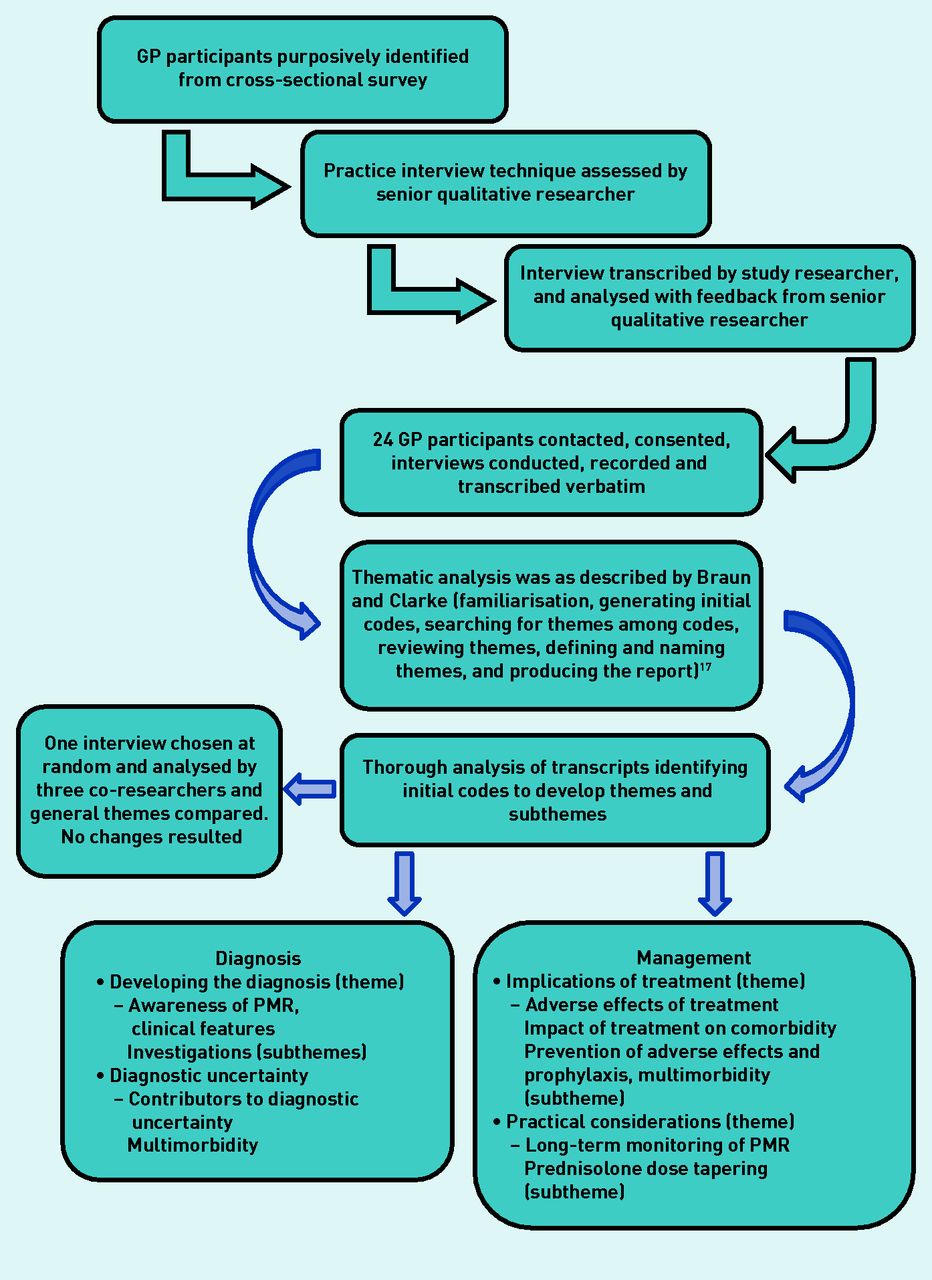
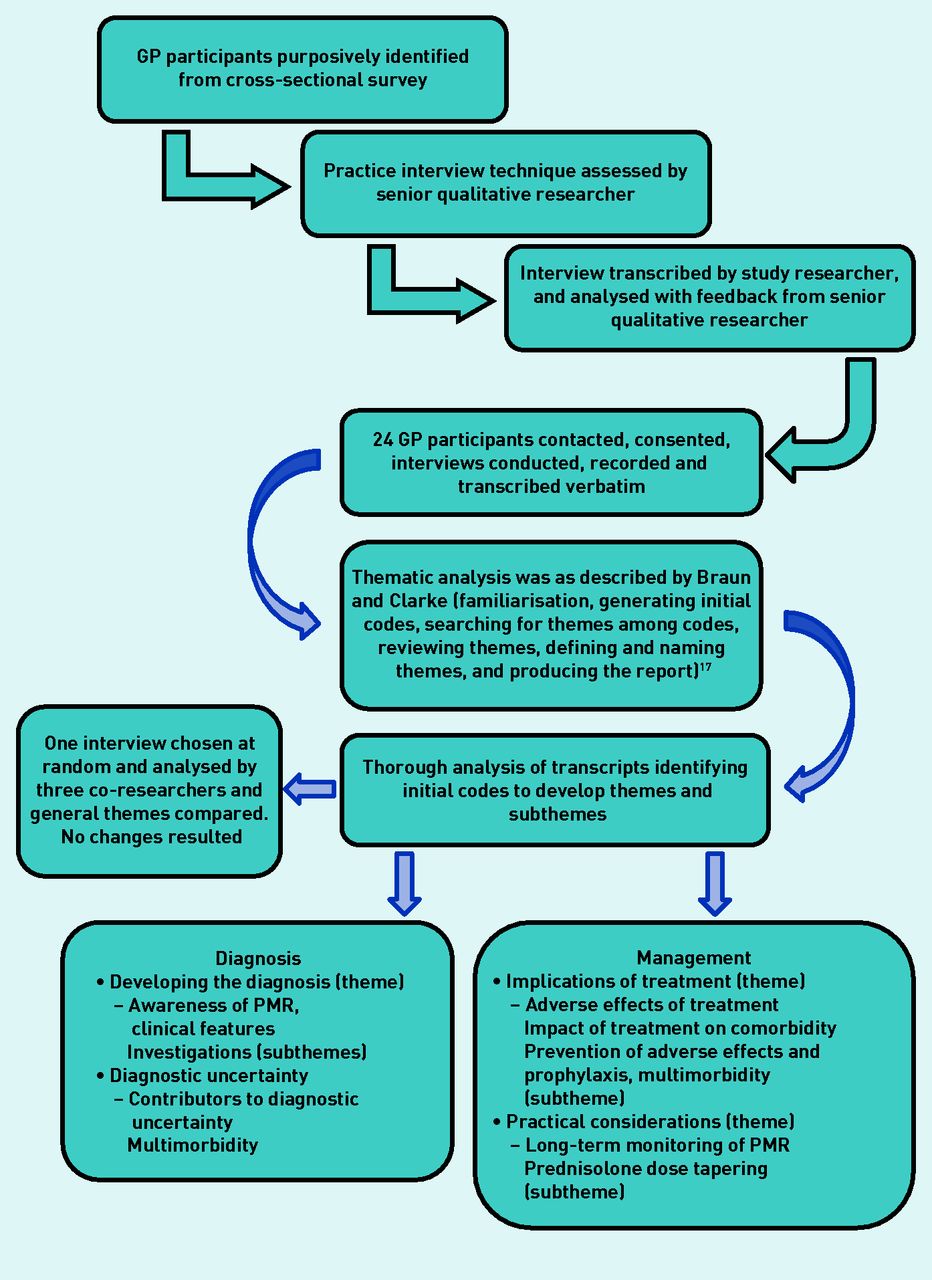
- Figure 1.
Summary of the qualitative telephone interview study. PMR = polymyalgia rheumatica.
- Figure 2.
Radar plot depicting median scores relating to GP rating of importance of presenting clinical features used to diagnose polymyalgia rheumatica.
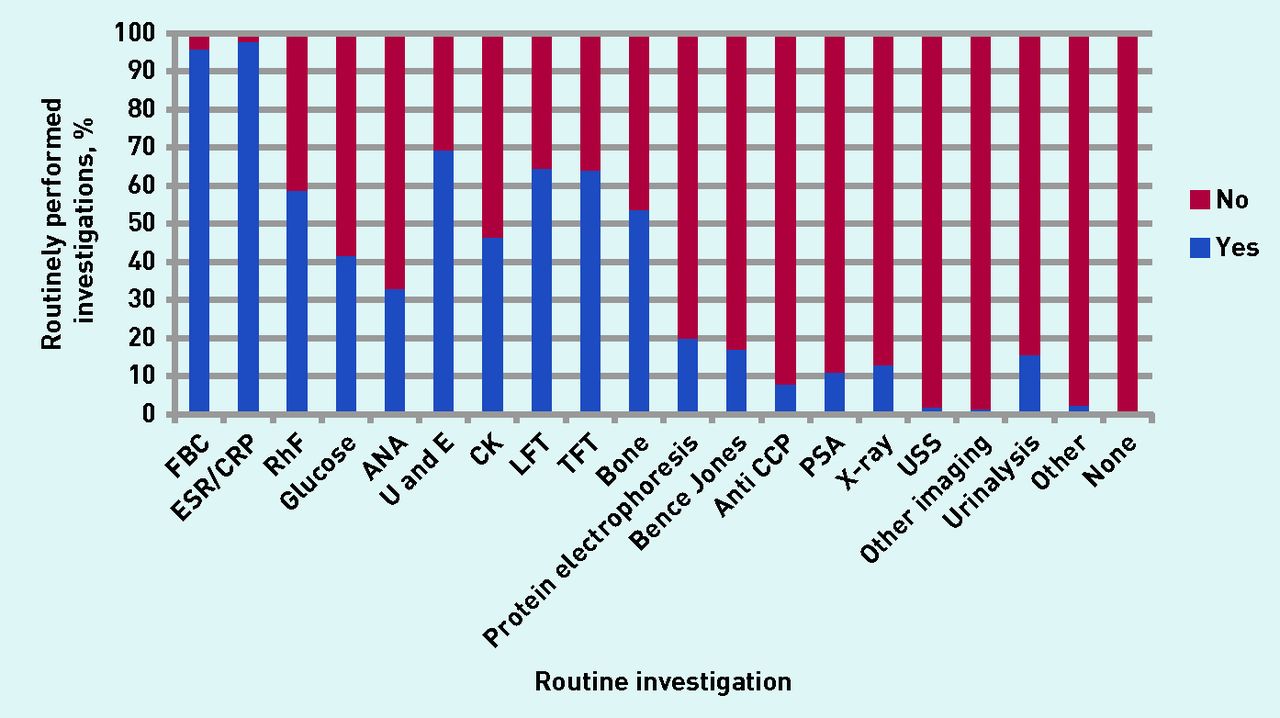
- Figure 3.
GP-reported routinely performed investigations for patients with suspected PMR. ANA = anti-nuclear antibodies. Anti CCP = anti-citrullinated protein antibody. CK = creatinine kinase. CRP = C-reactive protein. ESR = erythrocyte sedimentation rate. FBC = full blood count. LFT = liver function test. PSA = prostate-specific antigen. RhF = rheumatoid factor. TFT = thyroid function test. U and E = urea and electrolytes. USS = ultrasound scan.

{kind=link}
{kind=link}
{kind=link}
Tables
Characteristic Overall respondersa N= 1249 Postal respondersa N= 1132 Online respondersa N= 126 Non-responders N= 3751 Practice list size Mean 7129 7098 7519 6574 Median 6463 6375 7000 5700 IQR 3713–9313 3625–9125 4413–9588 3900–7500 Number of GP partners Mean 3.78 3.76 4.02 3.24 Median 4 4 4 3 IQR 2.5–5.5 2.5–3.5 2.5–3.5 1–5 Age, years, mean (SD) 44.05 (9.25) 44.48 (9.45) 40.79 (7.73) n/a Females, n (%) 649 (52) 598 (53) 68 (55) n/a Seniority, n (%) Senior partner 172 (13.8) 165 (14.7) 7 (5.7) n/a Partner 757 (60.6) 673 (59.8) 83 (67.5) n/a Salaried 260 (20.8) 234 (20.8) 26 (21.1) n/a Locum 31 (2.5) 29 (2.6) 2 (1.6) n/a Time qualified as a doctor, years Mean 20.1 20.4 16.3 Median 18 18 15 n/a IQR 10.5–25.5 6–30 10.5–19.5 Time qualified as a GP, years Mean 13.5 13.8 9.5 Median 11 11 15 n/a IQR 4–18 3.5–18.5 10.5–19.5 ↵a There were 8 duplicates online and 1 postal. IQR = interquartile range. SD = standard deviation.
Theme Subtheme Verbatim quote Diagnosis Awareness of PMR ‘I think a lot of the time it’s much older people, and they’ve just, kind of, gone, “Well, it’s part of getting old. I’m a lot achier than I was this time last year”, and they don’t realise that it’s necessarily something we could perhaps help with.’ (GP23, 13 years, F, S) ‘Well, I suppose, quite unusual, maybe the GPs aren’t aware of it. Or, you know, it’s not something that you see all the time …’ (GP8, 10 years, F, S) Developing the diagnosis Clinical features ‘Typically, when they’re complaining of shoulder pain, and they say, “I’ve had real trouble washing my hair or brushing my hair.” And there’s difficulty with getting up out of the chair because of the leg pain, you know, the, sort of, ones that give you the high index of suspicion.’ (GP23, 13 years, F, S) Investigations ‘I mean obviously the cardinal things I’m looking for are raised inflammatory markers so CRP and the ESR would be the two that I would be sort of looking at. However I would be doing a full blood count […] renal function […] liver function […] HbA1C […] creatinine kinase. If there’s been any weight loss already or any other sort of slightly sort of more sort of red flag symptoms I’d be considering things like an autoimmune profile or myeloma screen, tend to do a chest X-ray at baseline when I’m starting with the steroids but earlier than that if there’s any other systemic features. (GP6, 20 years, F, S) Factors causing diagnostic uncertainty ‘There is no diagnostic test so it’s a clinical diagnosis with suggestive blood results which can be hard to feel certain about and hard to convey convincingly to the patient, also there being lots of other conditions with similar presentations makes this even harder.’ (Participant 4814, 2 years, F, S) Contributors to diagnostic uncertainty Multimorbidity ‘I think it impacts at every stage, doesn’t it? It makes diagnosis harder because people often have conditions where symptoms overlap and so it makes it harder to assess. If their function is limited by something else then the usual things you might look for are already affected by their other things, so you can’t use your normal clues when going through their history. Often you see people who are on several other painkillers or who are maybe on steroids for something else, so it makes it difficult.’ (GP12, 15 years, F, S)
‘Often symptoms in older patients with multiple comorbidities, difficult sometimes to distinguish between any related symptoms including osteoarthritis and fibromyalgia.’ (Participant 1955, 17 years, F, P)Disorders mimicking PMR ‘Other things you know occasionally something else will be going on and kind of odd rheumatological things kind of I don’t know, where you’ve got cross over symptoms, vitamin D deficiency’s one that I’ve found where someone, we live in the west of the country which is a bit cloudier and white people are getting significant vitamin D deficiency who don’t go out very much and that can cause very similar symptoms. B12 deficiency again is something that I’ve picked up on the odd occasion and kind of I can’t think now what the, how that’s happened but I’ve certainly had to review the diagnosis.’ (GP16, 17 years, M, P) ↵a Identifiers in brackets after the quotes: GP followed by numeral = GPs who took part in the qualitative interview and their identifying number. Number of years = years as qualified GP. Participants followed by numeral = GPs who provided quotes from the survey. F = female. M = male. P = partner. S = salaried. CRP = C-reactive protein. ESR = erythrocyte sedimentation rate. HbA1C = glycosylated haemoglobin. PMR = polymyalgia rheumatica.
Theme Subtheme Verbatim quote Management Lack of alternatives to glucocorticoids ‘The lack of other options, really … and that nothing else does seem to work particularly well for it, and ‘you’re a little bit stuck if, for any reason, they can’t tolerate the steroids, and aren’t getting on with them. You are a little bit stuck with what else to suggest. Yes, it’s not exactly a nice option.’ (GP24, 12 years, F, S) Implications of treatment Adverse effects of treatment ‘There’s just the sense of people that were quite well old people turning in to people who suddenly have a lot of problems and they’re on more medication and they’re just not as well at the end as they were at the beginning.’ (GP17, 11 years, F, P) Prevention of adverse effects and drug prophylaxis Impact of treatment on existing comorbidity ‘So, then I say “And here’s another tablet for you. I’m sorry.” “And, actually, here’s a PPI [proton pump inhibitor] as well.’” (GP 24, 12 years, F, S) ‘Oh, definitely, yes, their diabetes control, definitely. I mean, they’ve usually got type 2 diabetes […] so they don’t run into any crises, but definitely, their diabetes control gets worse.’ (GP 24, 12 years, F, S) Practical implications of treatment and monitoring for PMR Long-term monitoring of PMR ‘Yes, again, sometimes people do get lost to follow-up, with all the will in the world, don’t they? So I had one lady who had been seeing me very regularly. We were bringing it [steroids] down. Something else cropped up with her, and she ended up, sort of, seeing somebody else for a while about another thing. And then she just had been left on this dose of prednisolone.’ (GP24, 12 years, F, S) ‘Keeping follow-up and reduction in steroids, not enough appointments to bring patients back routinely, patients need to be aware of the treatment plan and be proactive if arranging tests and for symptom review.’ (Participant 3529, 5 years, F, S) ‘Long-term steroid complications require careful and frequent follow-up, national and local guidelines and even within practice is muddled and lacks agreement, difficult access to secondary care, concerns they mix up diagnosis and timelines.’ (Participant 3927, 18 years, F, P) Treatment dose tapering ‘I mean, I like my PMR patients because they are fairly straightforward. There’s a kind of loose structure of reducing this drug, seeing how they respond. I will kind of go clinically; I don’t push them to have blood tests every month. I mean, it just seems pointless. I judge their response by symptoms, not inflammatory markers.’ (GP18, 22 years, M, S) ‘Main challenge is coming off steroids; most patients are completely delighted when their symptoms resolve after a week on steroids but become despondent and anxious when they start to experience steroid side effects (e.g. weight gain) and discover when they try to step down off their steroids their symptoms re-occur.’ (Participant 1665, 11 years, F, P) ‘Frequent input with steroid regimens/doses especially when they struggled with dose reduction, no matter how slowly it was done — some patients feel dependent on steroids and will end up taking more (without consulting you) to control symptoms even when perhaps their symptoms might not be due to PMR.’ (Participant 818, 4 years, M, P) ↵a Identifiers in brackets after the quotes: GP followed by numeral = GPs who took part in the qualitative interview and their identifying number. Number of years = years as qualified GP. Participants followed by numeral = GPs who provided quotes from the survey. F = female. M = male. P = partner. S = salaried. PMR = polymyalgia rheumatica.
In this issue









Jump to section
- Top
- Article
- Abstract
- INTRODUCTION
- METHOD
- RESULTS
- DISCUSSION
- Acknowledgments
- Appendix 1. Verbatim quotations obtained from qualitative study and open-response questions relating to diagnosis of PMRa
- Appendix 2. Verbatim quotations obtained from qualitative study and open-response questions relating to management of PMRa
- Notes
- REFERENCES
- Figures & Data
- Info
- eLetters
More in this TOC Section
Related Articles
Cited By...

