


Abstract
Background Psychological problems are common among adolescents. Many GPs consider these problems challenging, even after diagnosis.
Aim To explore how Norwegian GPs follow-up patients after a first diagnosis of a psychological problem at age 15–16 years.
Design and setting Nationwide longitudinal, register-based study using claims data for all GPs in the national list patient system, and for adolescents born in 1993 and 1994 (n = 129 499).
Method National databases and registers were used to determine how many adolescents received a first diagnosis of a psychological problem in a GP consultation at age 15 or 16 years. Further consultations, collaborative contacts in primary care, and referrals to secondary care during the year after diagnosis were then identified and used as outcomes in regression analyses to investigate associations with initial diagnosis, parental education, and GP characteristics.
Results In total, 6809 (5.3%) adolescents received a first diagnosis of a psychological problem in a GP consultation at age 15 or 16 years. Internalising problems constituted 50.5% of initial diagnoses among females and 28.8% among males. Behaviour and attention problems accounted for 21.3% for females and 45.0% for males. In total, 46.6% of females and 39.9% of males had ≥1 follow-up consultation, and 32.8% of females and 27.0% of males were referred to secondary care. GPs reported primary care collaboration for 22.1% of females and 19.1% of males. GPs with larger patient lists had higher referral rates, but collaborated less within primary care. Males with a male GP had more follow-up consultations than males with a female GP.
Conclusion GP follow-up after diagnosing psychological problems among adolescents is limited, but predominantly comprised referrals and some multidisciplinary cooperation. GP follow-up consultations should be studied more thoroughly, and the role of GPs warrants further policy discussions.
INTRODUCTION
Many young people experience psychological problems and,1 often, they do not know how to get help.2–4 Previous studies have shown that a substantial number of adolescents do seek help from their GP for psychological problems;5 however, when doing so, obstacles related to both the GP and the patient must be overcome to allow such problems to be recognised.3,4,6–11 Under-identification of psychological problems in GP consultations can be related to lack of time and knowledge among GPs.8 Alternatively, adolescents may not see their symptoms as psychological problems and, therefore, not present with them, or it may be that a lack of confidentiality or trust may hinder them from involving their GP when they have such problems.4
How GPs manage adolescents’ psychological problems once they have been recognised has received increased attention in terms of research.12,13 Many GPs consider psychological problems in adolescents challenging, particularly as GPs may lack the necessary education and skills to deal with these issues, and expectations of their role may be unclear.8,13–17 A recent study identified three different work styles, classifying GPs as one of the following three archetypes:
‘fixers’, who focus on the here and now, and aim to solve problems quickly;
‘future planners’, who delve deeper into the psychological distress; and
‘collaborators’, who emphasise the relationship with their young patients and more often cooperate with other services.14
Roberts et al also described a variety of shortcomings,18 related to the GP’s anxiety for their own professional performance when interacting with young patients, similar to those reported by Norwegian GPs.15
A GP’s ‘toolbox’ for adolescent mental health work includes counselling, offering follow-up appointments, and, sometimes, structured talking therapy.12,14,17 GPs may also collaborate with other first-line services, such as school health services, youth health clinics, or child care services.16 For serious mental health problems, referral to secondary mental health services for adolescents may be needed. In Norway, a comprehensive referral letter is required and, as in many Western countries — such as the UK, the Netherlands, and Denmark — GPs have this gatekeeper role,19 in some cases concerning adolescents; however, the child welfare services make the referrals, but most often in cooperation with the GP.
Most previous literature on how GPs work in this area is qualitative and based on representative samples of GPs or patients; there is a lack of larger, population-based studies. However, studies based on nationwide registers, such as those available in Norway, may provide an overview of how GPs approach this important task. As such, this study had two aims:
to investigate how Norwegian GPs follow-up patients aged 15–16 years after a psychological problem is diagnosed by a GP for the first time; and
to investigate whether variations in follow-up are associated with the initial diagnosis, parental education, or GP characteristics.
How this fits in
Among adolescents first diagnosed by a GP as having a psychological problem at age 15–16 years, internalising problems — depression, anxiety, and stress — were most common. Among males, externalising and attention problems — drug misuse, behaviour symptoms/complaints, memory disturbance, and hyperkinetic disorder (attention deficit hyperactivity disorder, ADHD) — constituted 45% of the diagnoses. Nearly half of the adolescents had at least one new consultation related to psychological problems in the subsequent year, one-third were referred to secondary care, and GPs collaborated with other primary care services for approximately 20% of adolescents. The GP’s role in following up adolescents with psychological problems, and the follow-up consultations in particular, should be studied further, and discussions regarding clarifying and improving the role of GPs in adolescent mental health are needed.
The magnitude of the challenge and process that leads to a GP recording a psychological diagnosis for adolescents aged 15–16 years is discussed in a previous paper by the authors.20
METHOD
A population-based study among Norwegian adolescents and all GPs in the national list patient system was conducted based on three nationwide registers:
the GP claims register (Control and Payment of Health Reimbursement database);
the Regular GP database; and
the population register.
These registers have been comprehensively described elsewhere.5
The target population comprised all persons born in 1993 and 1994, living in Norway, and recorded on a GP’s list in 2011 (n = 129 499). The study sample comprised all patients who had had a psychological diagnosis (P-diagnosis) from the International Classification of Primary Care (ICPC-2) recorded for the first time at age 15–16 years (index patients) by a GP.21 Patients for whom a P-diagnosis had been recorded by a GP at age 13–14 years were excluded.
Variables
Outcome variables
The main outcomes were:
follow-up consultations with adolescents with a P-diagnosis during the year after the first P-consultation (index consultation);
referrals to secondary mental health services for children and adolescents; and
multidisciplinary collaboration in primary care, including short communications between the GP and other municipal health and social services, or participation in multidisciplinary meetings regarding an index patient.
Explanatory variables
Patient variables were the:
total number of GP consultations — classified as 0, 1–2, and ≥3 — during the year before the index consultation;
mothers’ and fathers’ time in education, classified as ≤10 years, 11–13 years, and ≥13 years; and
P-diagnosis (separate or grouped) used in the index consultation.
GP characteristics used were GP age, sex, list size, and whether they were a specialist in general practice (a GP in Norway can become an approved specialist in general practice, which is not mandatory and requires a 5-year educational programme parallel with working as a GP). In addition, characteristics of the GP’s practice (based on contacts with the total GP patient population) were taken into consideration. These included the proportion of long (lasting >20 minutes) consultations being used as a continuous variable and the proportion of consultations with a P-diagnosis (grouped in quartiles) being used as explanatory variables.
Table 1 shows the distribution of the explanatory variables.
First psychological diagnosis in a GP consultation at age 15–16 years by number of prior GP consultations, length of parental education, and GP characteristics, N = 6809
In addition, the authors used the code for long consultations (>20 minutes) and code for talking therapy from the consultations with adolescents to describe the time spent in consultations. Because these codes are not allowed to be combined, the therapy code was assumed to also indicate a long consultation as it requires a more formal therapeutic approach.
Statistical analyses and missing data
Groups were compared using Pearson’s χ2 test and one-way analyses of variance. Negative binominal regression analysis was used to evaluate associations between the number of follow-up consultations and predictor variables. Logistic regression analysis was used to analyse predictors for referrals and collaborative contacts.
Multilevel models were used to take into account clustering with several adolescents on the same GP lists. The sample in the regression analyses was 6017 (88.4% of study sample) because 642 of adolescents had missing data on education for one or both parents and additionally 150 adolescents had missing data on GP characteristics (19 adolescents had missing data on both GP characteristics and parental education). Stata (version 15) was used for the statistical analyses.
RESULTS
Study sample and diagnoses
In total, 7148 adolescents out of those born in 1993 and 1994 received a first P-diagnosis in a GP consultation at age 15–16 years. Of these, 67 were diagnosed as having a stammer (P10), 46 with enuresis (P12), 168 with learning problems/dyslexia (P24), and 58 persons with ICPC codes related to function or procedures performed, without indication of type of psychological problem. These patients were excluded from the sample, leaving a final sample of 6809 adolescents (58.5% females), representing 5.3% of the study cohort
Internalising problems — depression, anxiety, and stress and the rest listed below heading ‘internalising problems’ — accounted for 50.5% of index cases among females, with depressive disorder being the most frequent diagnosis (15.4%) (Table 2).
Distribution of diagnoses used in index consultation in 15–16 year-old female (n = 3980) and male (n = 2829) patients born in 1993 and 1994, N = 6809
Among males externalising problems — drug abuse, child/adolescent behaviour symptom or complaint — constituted 18.0%, of index cases and memory disturbance or hyperkinetic disorder (ADHD) constituted 27.0%, compared with 10.7% and 10.6% among females, respectively (Table 2).
Among females, long consultation was used in 59.4% of index consultations compared with 50.7% among males (data not shown).
Follow-up GP consultations
Within 1 year after the index consultation, 46.6% of females and 39.9% of males had ≥1 follow-up consultations.
Approximately one-third of the patients had 1 or 2 follow-up consultations with a P-diagnosis (Table 3). With internalising problem as index episode, 13.5% of females and 13.4% of males had ≥3 follow-up consultations, and with less specific problems (P29 — Psychological symptoms complaint, other), 19.1% of females had ≥3 follow-up consultations, compared with 8.4% of males.
Number of GP follow-up consultations in the year after index consultation, and the proportion of long consultationsa
This diagnosis (P29) resulted in the highest percentage of long consultations among males (63.2%). Among females the highest percentages of long consultations was found for internalising problems (65.9%) and for P29 (65.8%).
Referral to secondary care
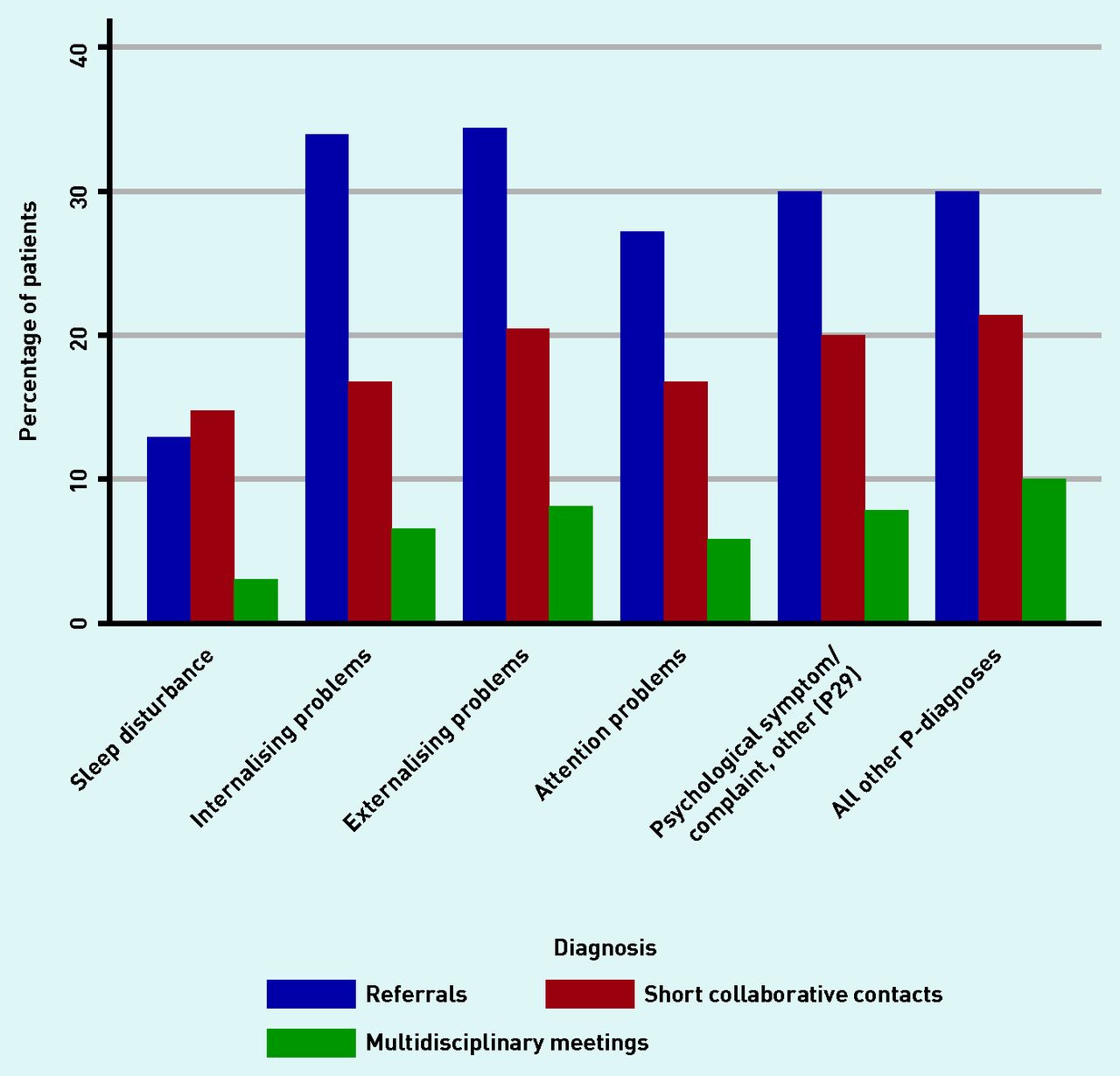
Overall, 20.4% of females and 17.9% of males were referred to specialist services during the week after their index consultation. Of these, 41.7% had no further P-consultation with the GP during the following year. Additionally, 12.4% of females and 9.1% of males were referred within a year, with substantial variation depending on the index diagnosis (Figure 1). The proportion of referrals varied from approximately 13% for sleep problems to approximately 34% for internalising and externalising problems.

{kind=link}
Percentage of patients where the GP report referrals or collaborative contacts within 1 year after an index P-consultation, by diagnosis.
Multidisciplinary collaboration
During 1 year, GPs took part in ≥1 multidisciplinary meetings concerning 7.4% of females and 5.8% of males. Other contacts with municipal services were reported for 18.7% of females and 16.6% of males. Both meetings and other contacts were reported for 4.0% of females and 3.1% of males. Overall, collaborative activity was reported for 22.1% of females and 19.1% of males (data not shown). Figure 1 shows the GPs’ collaborative activities for different groups of diagnoses.
No follow-up
For 34.5% of females and 40.9% of males, there were no other consultations coded with a P-diagnosis, no reported referrals, or no collaborative contacts in the 1 year after the index consultation.
Predictors of follow-up GP consultations
Compared with sleep disturbance as the reference category, an index diagnosis of an internalising problem increased the frequency of follow-up for both sexes (Table 4). For females, this was also the case for other psychological symptoms/complaints (P29). Having ≥3 GP consultations 1 year before the index consultation increased the number of follow-up consultations for both sexes (Table 4).
Negative binomial regression indicating associations between number of GP follow-up consultations after a GP index consultation and initial diagnosis, number of prior consultations, parental education, and GP characteristics
Males with a male GP had more follow-up consultations than males with a female GP, whereas GP sex had no impact among females. Having a GP with a high proportion of P-consultations overall in their practice statistically significantly increased the number of follow-up consultations among participants. Parents’ educational background was not statistically significantly associated with the number of follow-up consultations.
Predictors of referrals to secondary care and multidisciplinary collaboration
With sleep disturbance as the reference, all other diagnoses had three- to fourfold higher odds of referrals, and females had higher odds of being referred than males (Table 5).
Logistic regression showing associations between GP referral to secondary care (model 1) and GP cooperating with another municipal social or care service (model 2) in the year after index consultation, and the initial diagnosis, parental education, and GP characteristics
GPs collaborated more often with other municipal health or social services for female patients, compared to male patients. An index diagnosis of an internalising problem was comparable with sleep disturbance (reference) in terms of frequency of collaborative contacts; this was contrary to all other diagnoses, which had higher odds of GP collaboration (Table 5). Many prior GP consultations increased the odds of GPs engaging in collaborative contacts, but had no impact on referral rates. Having a GP with many patients increased the risk for referrals but decreased collaboration activity, while GPs who were specialists engaged in fewer multidisciplinary collaborative contacts than non-specialists.
Parental education had no effect on referral rates, but patients whose fathers had little education had markedly higher odds of their GP collaborating with other municipal services than those whose fathers had spent ≥11 years in education (Table 5).
DISCUSSION
Summary
This nationwide study presents a representative overview of how GPs provide care for adolescents they first diagnose with a psychological problem at age 15–16 years. The sample included 6908 patients, and represented 5.3% of the Norwegian population in this age group. Internalising problems were diagnosed at nearly half of these consultations among females and one-third among males, with depressive disorder being the most frequent diagnosis.
In the year after diagnosis, 46.6% of females and 39.9% of males had at least 1 follow-up consultation for a psychological problem. Referrals were made for 20.4% of females and 17.9% of males related to index consultation, and another 12.4% of females and 9.1% of males were referred to secondary care within 1 year. GPs collaborated with other primary care professionals and municipal services for 22.1% of females and 19.1% of males. For 7.4% of females and 5.8% of males (approximately 500 patients), GPs attended formal multidisciplinary meetings with other services
Index diagnosis of internalising problems, unspecified psychological symptoms (P29), number of prior GP consultations, and higher proportion of P-diagnoses in the adolescent’s practice had the greatest impact on follow-up.
There were some differences related to GP characteristics. Males had more follow-up consultations if their GP was male than their female counterparts, but GP age had no effect. If the GP had many patients on their list, referral rates were higher but there was less collaboration within primary care or with municipal services. GP specialists also engaged in less multidisciplinary work.
Parents’ educational background had no impact on the number of follow-up consultations or referrals, but GPs cooperated with other services more frequently when adolescents had fathers who had spent little time in education.
Strengths and limitations
The main strengths and limitations of studies based on Norwegian nationwide GP register data have been summarised in a previous paper by one of the authors.5
A main strength is that >99.5% of the population are part of the list patient system, which reduces selection bias and increases external validity of the findings regarding GP consultations. A specific strength of this study was the use of two complete age cohorts, which increased the validity and number of included patients. GPs usually report only one diagnosis for each consultation and this study, which was based on claims register diagnoses, may underestimate the amount of psychological problems GPs deal with in consultations with adolescents, because more than one problem may be discussed in a consultation.
An important weakness of the study is the uncertainty regarding the precision of GP diagnosis. For example, there may be variation between GPs in differentiating between feeling depressed (P03) and having a depressive disorder (P76), making comparisons between specific diagnoses difficult. Diagnoses were therefore grouped in the main analyses. A further limitation is including the code for talking therapy as an indicator of long consultations. However, this study’s estimates of long consultations after combining these codes seems reasonable when it comes to consultations for psychological problems because the average proportion of long consultations overall in GPs’ practices is around 30% (see GP characteristics, Table 1).
Comparison with existing literature
GPs concluded their involvement in 35% of the cases concerning females and 41% of males after the index consultation. Some of the diagnosed problems might have been ‘fixed’ or clarified as being sufficiently minor that the adolescents could manage the problem themselves; this approach has been shown to be valuable in a systematic use of short interventions.17,22 The relatively high proportion of long consultations indicates that GPs took time to adequately address problems in the index consultation, a theory supported by the study of Iliffe et al showing use of time in consultations with adolescents to be important when dealing with psychological problems.22 A higher proportion of P-diagnoses in a GP’s total practice (indicating the ‘mental health profile’) increased the rate of follow-up consultations for patients with P-diagnoses; this practice characteristic may mirror the ‘future planner’ archetype.14
This study also highlighted the GP’s role as referrer, as around 20% of patients were referred to secondary care immediately after their index consultation, which is consistent with Dutch findings.23 Many adolescents who were referred had no further consultation with their GP, indicating that the GP’s ‘fixer’ role had been fulfilled.14
Previous research indicates that collaboration substantially improves the quality of care, especially in this age group.24–25 When the GPs report contact with other primary care and municipal services for only one in five of these patients, an increase in collaboration with other services in municipalities regarding these patients might be an area for improvement of care.
Generally, females received more care in terms of the number of consultations, and had more long consultations, referrals, and collaborative contacts, which is consistent with the more frequent use of health care, in general, among females.26
Implications for research and practice
The usual treatment approach in mental health care of offering patients a series of consultations is seldom used by GPs. In this study, 7–19% of adolescents (depending on sex and diagnosis) had ≥3 follow-up consultations during 1 year after their psychological problem had been diagnosed for the first time. The majority of cases had no further contacts. The exact reasons for this are not known, but it may be that GPs do not generally define such treatment as part of their role or do not have the skills to enter deeper into psychological problems in this age group. The latter interpretation is supported by previous studies;13–15,18 Alternatively, adolescents who are offered another appointment may disagree with such an interpretation. How often adolescents themselves drop out of follow-up and their reasons for not wanting further contact should be studied more deeply.
The increasing proportion of males who are dropping out of school and work because of mental health issues is alarming, and may indicate that males should be better looked after, even though they may exhibit less active help-seeking behaviour.5,27
Referrals to secondary care were not infrequent and cooperation between GPs and secondary care is crucial for a high-quality mental health service for adolescents. For most patients in this study, GPs did not report any contact with other municipal services. This is inconsistent with the collaborative approach described in most recommendations for health services for young people10,16,24 and must be addressed. In addition, closer contact between GPs and other primary care services is needed when providing care for adolescents with psychological problems.
Although primary care may be a good starting point for managing adolescent psychological problems, this study highlights the need to strengthen Norwegian GPs’ knowledge and skills in this area through educational programmes that have been found to improve GP services elsewhere.22,23 Such programmes must be followed by research to evaluate their usefulness.
This study showed that one in 20 adolescents aged 15–16 years consult a GP for the first time with a psychological problem. The GP’s subsequent role in following up these problems appears to be somewhat limited, and further discussion about how to improve their future contribution in this field is warranted. Providing help and support to young people struggling with psychological difficulties may increase their quality of life, have important societal effects — such as helping adolescents complete their education28,29 — and may even save lives.
Acknowledgments
The authors thank Audrey Holmes, MA, from Edanz Group for editing a draft of this manuscript.
Notes
Funding
There was no funding for this study.
Ethical approval
The use and linkage of the registers are approved by the Norwegian Data Inspectorate (project 13646) and the register owners: the Norwegian Board of Health, Statistics Norway, and the Norwegian Directorate for Education and Training.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received January 29, 2018.
- Revision requested March 13, 2018.
- Accepted May 29, 2018.
- © British Journal of General Practice 2018
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

