


Early-onset emphysema may have genetic and environmental causes. This case study reports on two cases that draw attention to the importance of taking a careful occupational history.
CASE HISTORIES
Patient 1
A 51-year old male presented with a 10-year history of progressive breathlessness on exertion, noticed initially while training a youth football team. By the time of assessment in 2003 he was unable to run and had stopped work as a window fitter due to breathlessness. He had an intermittent cough and wheeze with daily clear sputum production. There was no diurnal variation in breathlessness, nocturnal cough, or history of asthma and atopy. He took no regular medication, and had never smoked, though both parents smoked at home when he was a child. His father died of ischaemic heart disease and emphysema at the age of 67 years. Computerised tomography (CT) scan of the lungs showed severe emphysema (Figure 1). Lung function was typical of centriacinar emphysema with mild airway obstruction (FEV1/FVC = 53%; FEV1 = 2.77 L, 73% predicted; FVC = 5.19 L, 109% predicted), significant air trapping (residual volume = 3.02 L, 135% predicted) and severely reduced gas transfer (DLCO = 3.96 mmol/min/kPa, 37% predicted). Liver function tests and alpha-1 antitrypsin phenotype (MM) and level (1.93 g/L) were normal. He was treated with inhaled beta-agonist, corticosteroid, and antimuscarinic drugs, and attended pulmonary rehabilitation. There was a steady decline in his lung function over 13 years and lung transplantation was precluded due to significant coronary artery stenosis.

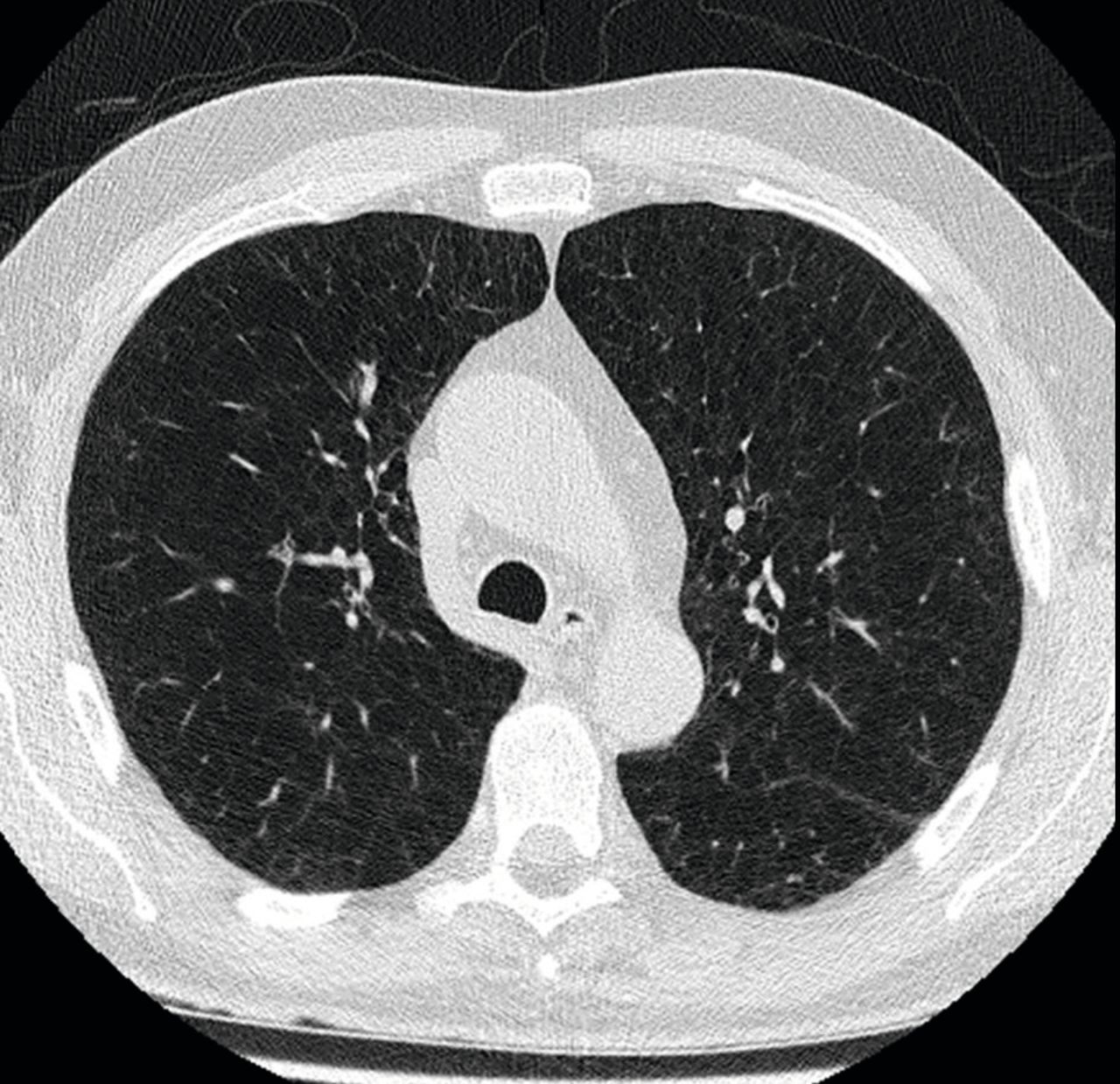
High-resolution computerised tomography (CT) image at the level of the aortic arch from patient 1, showing severe centriacinar emphysema of both upper lobes.
Patient 2
A 50-year old man, the brother of patient 1, presented with a 15-year history of progressive breathlessness that necessitated stopping work at his brother’s window-fitting business. There were no diurnal features, no weight loss, cough, sputum production, or wheeze, and he too was a lifelong non-smoker. Lung function testing and CT appearance were almost identical to that of his brother. Liver function tests and alpha-1 antitrypsin phenotype (MM) and level (1.22 g/L) were all normal. At 6 years following diagnosis there had been a steady deterioration, leading to exercise limitation of 20 yards, with FEV1 = 0.91 L (25% predicted) and DLCO = 3.41 mmol/min/kPa (32% predicted). Thus he underwent bilateral sequential lung transplant in August 2016 (Figure 2) with good physiological recovery.
{kind=link}
{kind=link}
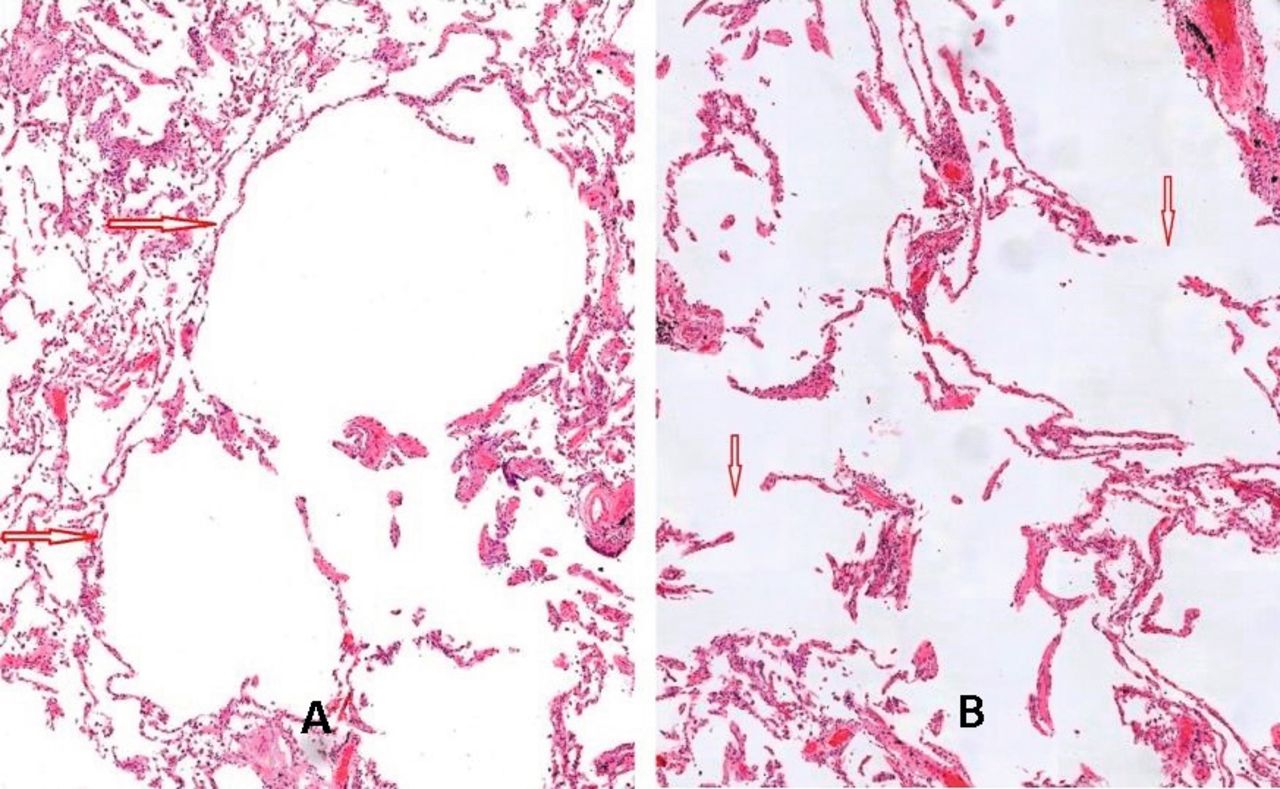
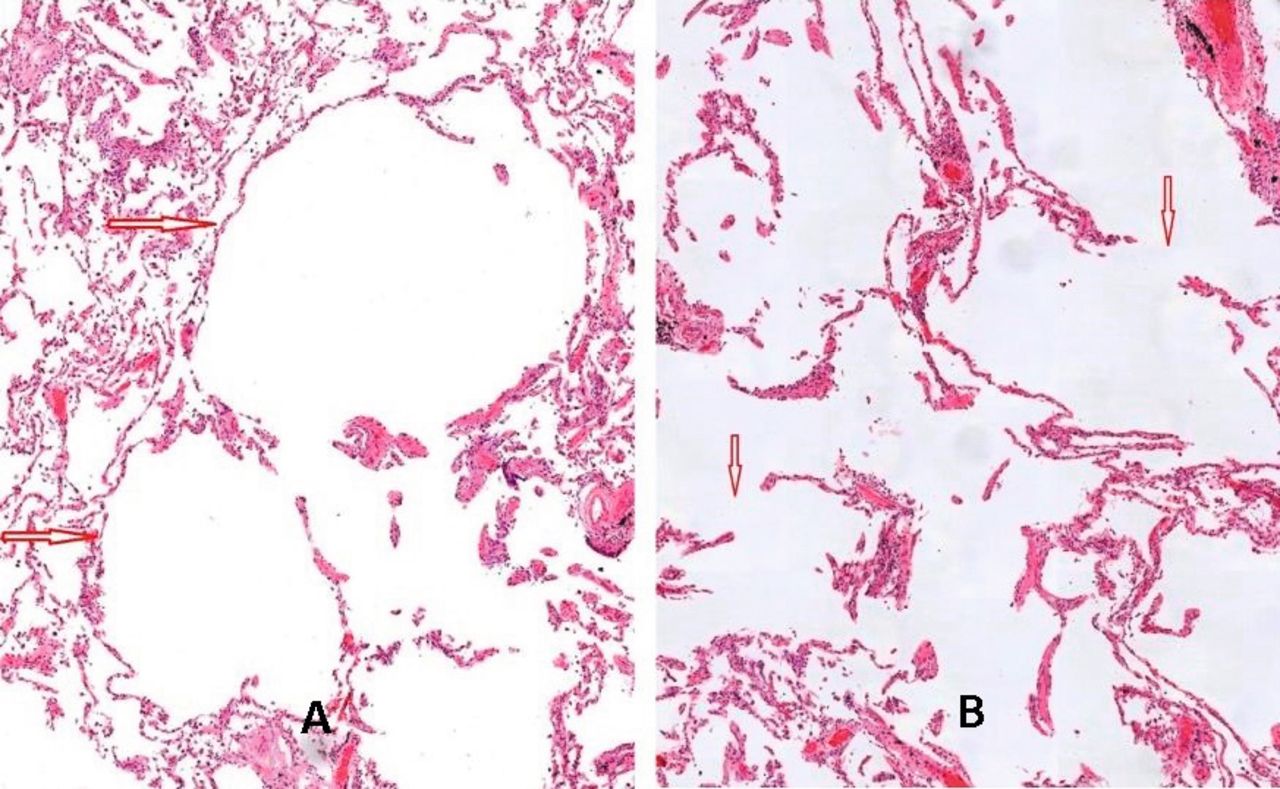
Histology from explanted lung from patient 2 at 20× magnification showing centriacinar alveolar dilation (A: arrows) and pronounced fragmentation of alveolar walls (B: arrows) in keeping with severe emphysema.
DISCUSSION
Emphysema with disabling breathlessness can present with normal or near-normal spirometry. However, significant air trapping and poor gas exchange are only revealed physiologically on full lung function testing; significant air trapping can usually be seen on plain chest radiograph. Severe emphysema under the age of 50 years is unusual and its occurrence in two brothers and their father suggests a genetic cause. Alpha-1 antitrypsin deficiency is the underlying cause in most with this family history; however, it was excluded both by the normal levels and phenotype, which can be obtained routinely from hospital laboratories. Family studies of emphysema have shown familial aggregation independent of alpha-1 antitrypsin deficiency, so an undefined genetic cause was still possible.1 Not all smokers can be relied on to tell the truth, particularly about marijuana smoking, which can cause severe and premature upper lobe emphysema; both denied ever smoking any recreational materials.
Emphysema can be caused through occupational exposure, so a lifelong occupational history is required. Patient 1 left school aged 15 years and became a furnace man in drop forges for 8 years, using cast iron and mild steel. Subsequently he was employed for 7 years as a caster at a manufacturer of zinc alloy products. He drew molten zinc alloy from the furnace and melted two cadmium sticks into each casting bucket, which then gave off an orange fume. He processed 24 buckets in each 8-hour shift and wore no respiratory protection; then followed 16 years as a window fitter. Patient 2 joined the same zinc alloy manufacturing company as his brother at age 18 years and worked there for 9 years in an identical role. At age 27 years he changed role within the company to drive forklift trucks, until leaving to start a window-fitting company with his brother. Their father also worked at the same casting company.
Cadmium is used as an electrode for rechargeable nickel-cadmium batteries, as steel plating, electric cabling, solder, and in pigments for plastic and ceramics. Inhalational exposures occur when cadmium is heated above 320°C, where it produces the orange-brown fume cadmium oxide; the highest exposures occur with processes that heat cadmium, such as foundry work, soldering, brazing, and electroplating. Once absorbed, cadmium binds to the protein metallothionen. If binding capacity is saturated, excess cadmium accumulates in the kidney with a long but variable elimination half-life (10–40 years). By the time that our two brothers presented, both of their urinary cadmium levels were normal (<0.3 mcg/g creatinine). Acute pulmonary presentations following inhalational exposure to high concentrations of cadmium oxide fume have been described and include fatal acute pneumonitis, pulmonary oedema, and a syndrome not unlike metal fume fever with transient headache, chills, chest pain, and breathlessness.2
The seminal case-control study of emphysema in 101 copper-cadmium alloy workers showed a linear dose-related lung function decline, and presence of emphysema independent of cigarette consumption.3 Owing to the quality of evidence for causation, British cadmium-exposed workers with emphysema are now entitled to state benefit through the industrial injuries scheme,4 provided they have an aggregate exposure of 20 years; neither patient was awarded benefit having had <20 years’ exposure. Affected workers may also make a claim for compensation under civil law, though this requires proof of negligence on the part of the employer.
The attributable risk for occupation and chronic obstructive pulmonary disease (COPD) is estimated to be 15% within the general population.5 Workplace exposures to other dusts (grains, wood dust, coal dust, silica), chemicals (isocyanates, polycyclic aromatic hydrocarbons), and fumes (welding fume) all contribute. The strength of evidence for causal relationships is stronger for some agents than others, and currently only COPD/emphysema caused by cadmium fume or coal dust is eligible for UK industrial injuries benefit. However, other jobs independently associated with COPD identified from epidemiological studies include farmers, welders, wood and metal workers, and construction and cement factory workers.6 As smoking becomes less common the importance of other risk factors will increase. Because the prevalence of COPD in working populations can be up to 30%,6 careful occupational histories are required.
Notes
Provenance
Freely submitted; externally peer reviewed.
Patient consent
The patients gave consent for publication of this case report and images.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received August 10, 2018.
- Accepted August 28, 2018.
- © British Journal of General Practice 2019
In this issue









More in this TOC Section
Related Articles
Cited By...

