


Substantial evidence has now accrued to robustly support systematic case finding using pulse regularity checks in general practice to detect atrial fibrillation (AF) in people aged ≥65 years. Fay et al have summarised this evidence to make the case to detect an additional 10–15 cases of AF per 1000 people screened.1 Cole et al have shown that such ascertainment in people aged ≥65 years by GPs is feasible in entire local CCG populations, with increases in AF register size of 5–10%.2
However, the National Screening Committee has so far remained doubtful about supporting a national screening programme for AF, and the US Preventive Services Task Force recently recommended against electrocardiographic screening for AF.3 An increasing number of methods to detect irregularity of heart beat — ranging from simple pulse checks every 5 years in primary care to continuous electronic monitoring detecting short-duration irregularities with less certain treatment benefits — have complicated the picture.4 Case finding in general practice using episodic pulse regularity checks is supported by a UK Health Technology Report concluding that: ‘Systematic opportunistic screening is more likely to be cost-effective than systematic population screening. Nurse pulse palpation or modified blood pressure monitors would be appropriate screening tests, with confirmation by diagnostic 12-lead electrocardiography.’ 5
Current NICE guidance on the measurement of blood pressure also recommends pulse palpation to detect irregularity. However, despite the positive and cost-effective results of case finding shown in the randomised SAFE trial and observational studies in UK general practice,2,6 some GPs and other commentators have remained doubtful about such simple methods for the systematic detection of AF.7 Large randomised controlled trials are the desirable gold standard for new cost-effective interventions for ascertainment of AF to reduce stroke, but they are not the only sources of relevant information. A single large trial is unlikely to be able to cover all diverse populations, in all diverse settings, and for all treatments. As the ascertainment and treatment of hypertension has shown, case finding has an illustrious history in general practice. Blood pressure ascertainment has evolved with evidence, practice, and policy. Trials, diverse studies, and real-world observational data have all provided important evidence. However, after almost 40 years including large-scale trials of blood pressure screening and treatment, there is still no recommended national screening programme for hypertension, with policymakers opting instead for NICE guidance and a heterogeneous mixture of vascular risk management programmes including general practice ascertainment and NHS Health Checks. General practice has successfully improved ascertainment and management of hypertension, but few would disagree that progress has been inordinately slow and there is still much to do. We are still waiting for better funding, and further studies on AF are desirable, but neither are excuses for inaction. Such studies might include other outstanding questions such as the optimal intervals for ascertainment — 5 yearly or annually, the cost-effectiveness of ascertainment in high-risk groups at younger ages, and the further benefit of repeated or various electronic measurements. But these further questions are also not an excuse for inaction. Importantly, the existing evidence shows that case finding is feasible in routine general practice with entire older CCG populations receiving pulse regularity checks, yielding important numbers of new treatable AF cases. Treatment of AF whether screen detected, incidentally and asymptomatically detected, or symptomatically detected is effective in reducing stroke.2,6
For GPs, there are two important questions frequently asked about systematic AF case finding. Does asymptomatic AF, or AF detected by screening, carry the same risk as symptomatically presenting AF? Second, does anticoagulation of such new cases reduce their stroke risk?
There is currently no randomised trial of anticoagulation specifically in asymptomatic AF or screen-detected AF (the latter are ongoing). However, there is good existing evidence from non-randomised and observational comparative studies, which confirm that:
at the time of detection around a third of current AF cases are asymptomatic;
asymptomatic AF is associated with a greater risk of stroke than symptomatic AF;
that treatment of asymptomatic AF is associated with reduced stroke risk; and
that anticoagulation of screen-detected AF in whole populations at older age is associated with reduced stroke risk.
ASYMPTOMATIC PRESENTATION OF AF
AF may present in three main ways: most typically with palpitations, or with other non-palpitation symptoms, or asymptomatically. Asymptomatic AF carries a higher risk of stroke or mortality than typical presentations with palpitations. In a study of 476 randomly selected patients known to have AF, 40% presented ‘typically’ with palpitations, 26% had other non-palpitation symptoms, and 34% had asymptomatic AF presentation.9 Patients presenting with palpitations had significantly lower CHA2DS2-VASc scores compared with non-palpitation symptoms and asymptomatic presentation. Asymptomatic AF was associated with a greater risk of cardiovascular events (adjusted hazard ratio [HR] 3.12, 95% confidence interval [CI] = 1.50 to 6.45) and all-cause mortality (HR 2.96, 95% CI = 1.89 to 4.64) compared with palpitation-associated AF after adjustment for CHA2DS2-VASc score and age.
Further studies have confirmed the adverse risk profile of asymptomatic compared with symptomatic AF. In a study of 3119 patients in a European registry, 40% were asymptomatic, and they were three times more likely to have permanent AF but less likely to receive oral anticoagulants than symptomatic patients. Mortality at 1 year was more than two-fold higher in asymptomatic patients compared with symptomatic patients (9.4% versus 4.2%, P<0.0001).10 In a ‘real world’ setting a 10-year follow-up of 1100 asymptomatic and symptomatic people with AF confirmed higher stroke risk in asymptomatic patients.11
ROUTINE PULSE CHECKS CASE FINDING AND/OR SCREENING FOR AF
At older ages, opportunistic pulse checks using episodic manual pulse checks or simple electronic devices are effective in detecting new cases of AF in older people, increasing AF prevalence by 5–10%.6 Electronic methods are also effective at detecting new cases, with repetitive testing associated with higher rates of detection than methods using a single point in time.12 The natural history of AF shows that it is often an intermittent condition tending, over time, to progress to more permanent states. The studies described above rely on episodic ascertainment at a point in time and may miss intermittent AF. Opportunistic testing using cheap mobile ECG devices or enhanced blood pressure monitors, such as AliveCor, Omron, and WatchBP, is becoming widespread. In addition, more continuous electronic monitoring has been employed to identify a variety of cardiac arrhythmias including brief episodes of atrial tachyarrhythmia unlikely to be identified by episodic ascertainment. The role of anticoagulation for such brief arrhythmias has yet to be established.4
ANTICOAGULATION OF ASYMPTOMATIC AF AND STROKE RISK
An observational study in UK primary care of 5555 patients with incidentally detected AF over 3 years showed that incidentally detected asymptomatic AF treated with oral anticoagulants was associated with a reduction in stroke risk. Among incidentally detected AF in UK primary care, anticoagulant therapy was prescribed to 51% and was associated with HR of 0.35 (0.17–0.71) for stroke, and 0.56 (0.36–0.85) for death, compared with no therapy.13
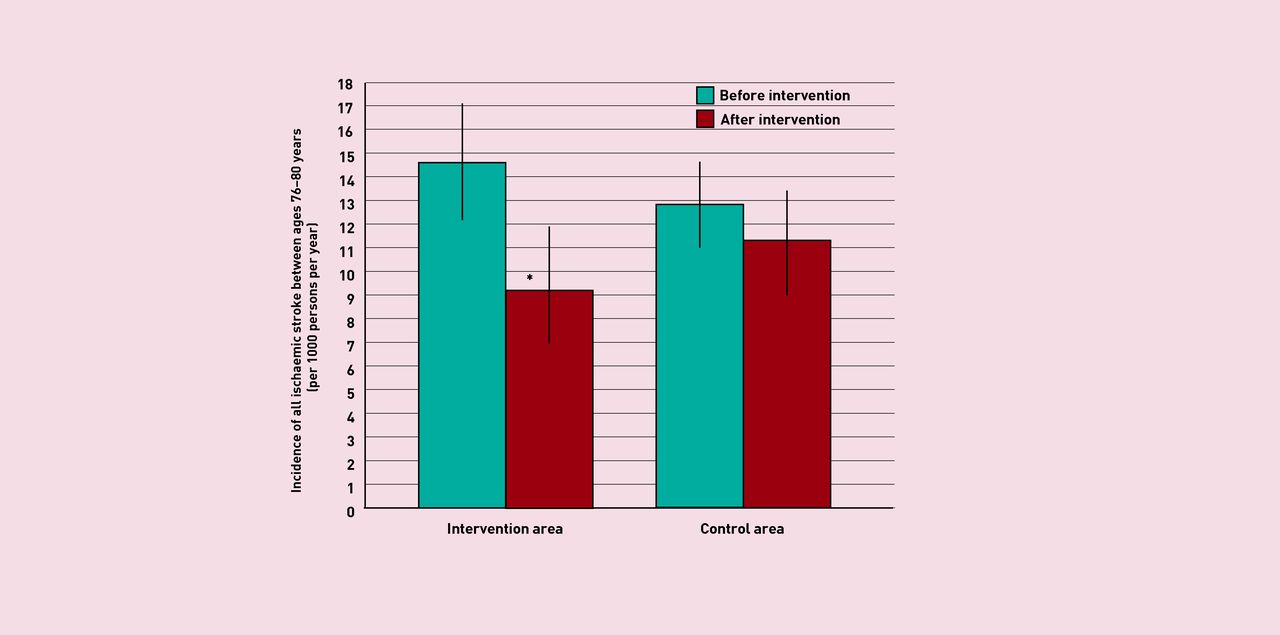
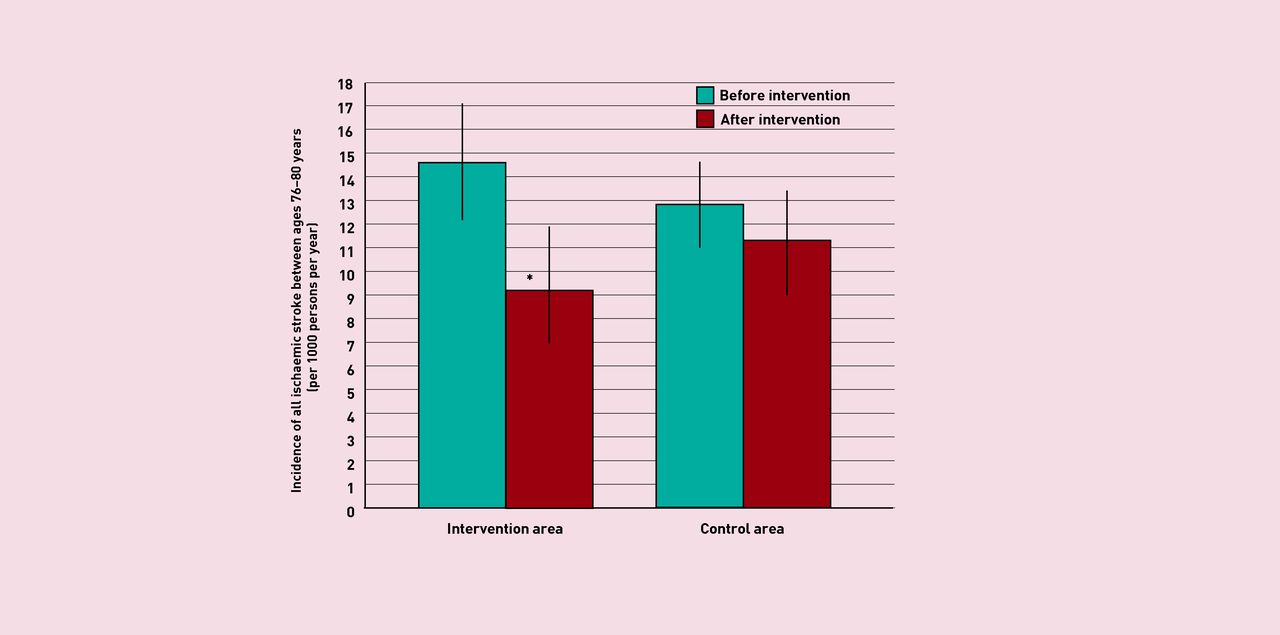
In a programme in two Swedish municipalities, repeated ECG screening for AF in people aged 75–76 years found more cases of AF during 5 years of follow-up than in a control municipality. The incidence of all ischaemic stroke declined from 14.5 to 9.1 per 1000 persons per year in the intervention (P = 0.003), but not in the control area where the incidence changed from 12.7 to 11.2 per 1000 persons per year (P = 0.31) (Figure 1).8 Further randomised controlled trials of systematic screening to detect AF are underway, both in the UK and elsewhere.14
{kind=link}
Ischaemic stroke before and after intervention to detect AF in control and intervention localities in Sweden. From Engdahl J, Holmén A, Rosenqvist M, Strömberg U. A prospective 5-year follow-up after population-based systematic screening for atrial fibrillation. EP Europace 2018.8 Reproduced by permission of Oxford University Press.
CONCLUSION
In summary, there is now good evidence that systematic detection of AF using episodic manual or electronic pulse regularity checks is associated with increased detection of AF. Asymptomatic cases are associated with higher risks of stroke than people with symptomatic AF, and may be less likely to be anticoagulated. In people with asymptomatic AF treated with anticoagulants there is a reduction in strokes, and community screen detection leads to lower levels of stroke. In short, pulse regularity checks are an effective way to detect new cases of AF that will benefit from anticoagulation. Further evidence and trials are desirable, but opportunistic case finding for AF is simple and feasible in general practice for whole populations at older ages, and anticoagulation is an effective treatment to reduce stroke.
Notes
Provenance
Freely submitted; externally peer reviewed.
- © British Journal of General Practice 2019
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

