


This article argues that, rather than aiming for a psychiatric diagnosis, generalist professionals such as those working in primary care, as well as in other hospital and community settings, should use a non-diagnostic framework when encountering distress. The conceptual and empirical limitations of the psychiatric diagnostic system and evidence that psychological phenomena are dimensional suggest the need for an alternative approach; one that might also address problems of overdiagnosis and overmedication.1
There are three key problems with the current Diagnostic Statistical Manual (DSM) and International Classification of Diseases (ICD) systems of psychiatric classification. The process can be stigmatising; diagnoses are not adequate representations of reality; and they are inadequate for informing an individualised management plan. The current categorical diagnostic system encourages the patient to understand their distress as a disease, rather than as an understandable response to current problems, genetic inheritance, and past experience of trauma, loss, and problematic attachments. Although some patients are comforted by labels, we propose that a more scientifically valid and individualised assessment can provide a deeper understanding, a sense of being understood, and access to specialised services and benefits if required.
During the 20th century, psychiatrists created a relatively unified practice through the closely related ICD and DSM systems. Despite notable exceptions, such as Balint2 and more recently Dowrick,3 GPs have generally advocated the psychiatric model that is enshrined in the RCGP’s curriculum and in NICE guidance. Attitudes of professionals, however, are more mixed. Studies of practice show how diagnoses are not always offered, and that GPs’ talk often follows the patient’s view that the emotional distress might be related to social problems.4
The poor performance of the psychiatric diagnostic system demonstrates how diagnoses are inadequate models of reality. Diverse phenomena, such as thinking patterns, emotions, physical symptoms, and behaviours, have been lumped together, and the same diagnosis of depression can be allocated to two individuals with no symptoms in common. Diagnoses are not stable over time or reproducible;5 they are not consistent across cultures.3 They overlap so that comorbidity is the ubiquitous making it meaningless.6 Although many physicians are carefully laying out complex evidence-based dimensional approaches that cut across traditional specialties (for example, cardiometabolic problems), most mental health experts within the establishment continue to endorse categorical systems despite the opposing evidence from genetics through to social epidemiology. Exceptions include the US National Institute of Mental Health, which has abandoned investment in diagnosis-based research in favour of investing in neuroscience and the collaboration developing the HiTOP dimensional approach.7
RATIONALE FOR AN ALTERNATIVE SYSTEM
What kind of system could replace this diagnostic model? It would need to be simple and understandable to both patients and practitioners. It should also form the basis for decisions about care and be intrinsically therapeutic. The system should provide an explanation of the links between different aspects of patients’ lives: emotions and feelings, perceptions, thinking patterns, physical illness/symptoms, behaviours, and social situations. Additional causal influences can be included where important: cultural context, losses, traumas, early attachments, and genetic heritage. These can be incorporated into a ‘shared understanding’ that is both technical and narrative. The approach draws on psychological theories and therapies, and is informed by evidence about the substantial links, which are often bidirectional, between: our social situation and our mental wellbeing;8 our body and mind;9 and genetics and neurodevelopment.10
A LOGICAL APPROACH TO DEVELOPING A SHARED UNDERSTANDING AND PLAN
An individualised causal model, created through empathic discussion, should bring new insights for both patient and practitioner. Diagnosis is likely to enter the discourse and can be explained as an additional way of understanding situations, as well as one around which much research for interventions has been based. However, it need not take primacy over ensuring that individuals’ concerns about real issues are prioritised.
Three linked, iterative (though not necessarily sequential) analytic steps are described below; these build on Sackett’s clinical epidemiology and are relevant to a range of complex clinical scenarios. 11
Step one: prioritising key issues facing the patient now. At the core will be the emotions, thinking patterns, behaviours, physical illnesses, and social situation of the present. Strengths and personal goals as well as the most important problems can be elicited. Suicidality will need to be assessed along with other self-harming impulses and behaviour, including the use of alcohol and other substances.
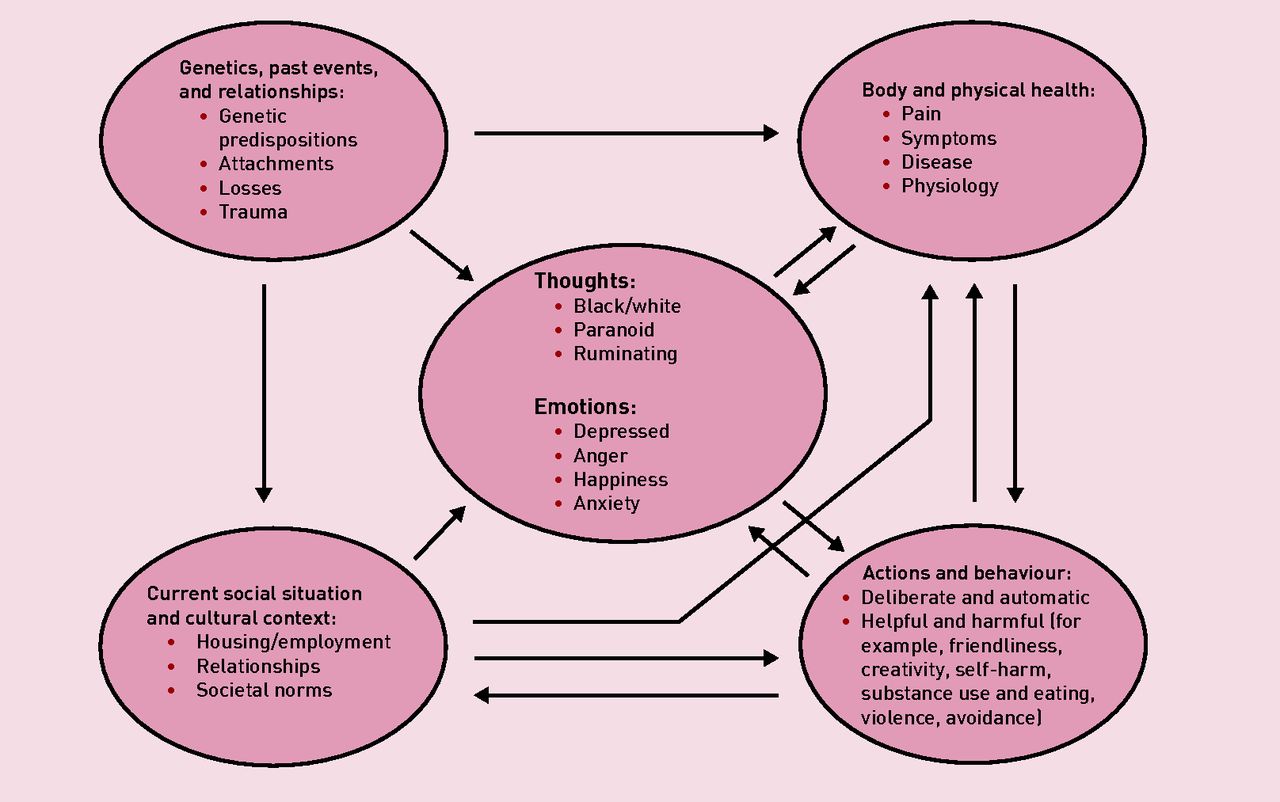
Step two: explicit causal linkage between the key issues. This step adds to Sackett’s principles.11 Figure 1 depicts the range of issues within the domains and links between them. Some links will have been revealed already: ‘I’m just too exhausted to go to work.’ ‘I’m just so fed up with the pain.’ Other links can be explored with open or direct questions: ‘I am wondering if you tend to drink when you are anxious about social situations.’
{kind=link}
Domains with examples and theoretical links.
Such a shared understanding will always be partial, a device to inform action, one that will change and can be reworked over time. Its historical depth can be defined by the patient’s willingness and felt need to delve into past traumas and relationships without necessarily exploring detail in order to avoid re-traumatising. It should be ‘owned’ primarily by the patient, and shared with practitioners, friends, and family when needed.
Step three: shared action plan based on identified priorities, goals, and available resources. The plan to address these goals can be constructed analytically from the range of available resources: the strengths of the individual; the skills of the practitioner; other community services and opportunities; and friends and family.
We propose two types of judgement made by patient and practitioner for this step. The first is based on quantitative evidence from the literature, regarding antidepressants, CBT, and other therapies, about what works for the average patient. The second relates to specific goals of the individual patient. Both require interpretation12 about the potential for a particular action or intervention to have an effect. However, given the low effect sizes of mental health interventions, an individual’s experience often becomes the best evidence about what might be effective.
Examples of interventions linked to a whole-person shared understanding for a young mother with low mood might include: choosing counselling over CBT to address continued rumination about a bereavement; agreeing to ask a friend to accompany her to the park with her children in order to improve her personal identity as a ‘good parent’; and supporting changes in shopping habits to reduce comfort eating leading to weight gain, which can add to low self-esteem.
IMPLICATIONS FOR PRACTICE
Although not a formal therapy, and based on humanistic impulses as well as good science, we suggest that this model will support consultations to be more intrinsically therapeutic2 by helping individuals see their problems as understandable and remediable. As a unifying way of seeing an individual using a biopsychosocial perspective, it is based on evidence from a wide range of disciplines, including how GPs often practise, and yet is a radical departure from guidelines as articulated by NICE and the RCGP curriculum. However, it also incorporates a different way of seeing the world, and as such can be taken on both in essence and in parts, to suit busy practitioners.
Such a step change will not be easy. In our time-pressured system, advice on what to do less of, such as completing diagnostic questionnaires or initiating antidepressants, may be needed alongside guidance on how to deliver the model in two to three consultations. Support for patients to use and understand the approach alongside potentially conflicting diagnostic approaches will be necessary. It will be important to evaluate feasibility, cost, relevance, and perceived benefit to patients and practitioners.
KEY MESSAGES
The current psychiatric diagnostic system on which we base treatment of mental health problems is conceptually and empirically flawed. An individual’s distress can be better understood through assessing the links between problematic thoughts, emotions, behaviours, social situation, and physical health. Decisions about how to address distress can best be made by estimating potential benefit for individualised interventions alongside use of traditional evidence-based interventions based on mean effects for populations.
Acknowledgments
This article arose from reflection on practice, ongoing conversations with colleagues, and an evaluation of the literature. The concept was first presented at a workshop at the 2016 WONCA Europe conference in Copenhagen and the authors are grateful for responses from attendees.
Notes
Funding
Richard Byng’s time was funded by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care South West Peninsula (NIHR CLAHRC South West Peninsula). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care.
Provenance
Freely submitted; externally peer reviewed.
- © British Journal of General Practice 2019
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

