


INTRODUCTION
Chronic diarrhoea has an estimated prevalence of about 4–5% in Western populations and is one of the most common reasons for gastroenterology referral.1 There is a myriad of causes for chronic diarrhoea, which can make the investigation and diagnosis of the underlying cause difficult. In 2003, the British Society of Gastroenterology (BSG) released guidelines2 to aid in the investigation of chronic diarrhoea; however, these have since been updated, in April 2018. Below, we provide a brief and focused summary of the new 2018 guidelines1 for primary care, highlight the new changes compared with the 2003 edition, and discuss some limitations of the new guidance.
CLINICAL ASSESSMENT IN PRIMARY CARE
Initial investigations in primary care are aimed at differentiating organic gastrointestinal (GI) disease from functional disease. Routine, screening blood tests are recommended in all patients presenting with chronic diarrhoea, and these include full blood count, ferritin, c-reactive protein, coeliac serology, and thyroid function tests. Faecal calprotectin (FCP) is now recommended as a screening tool to detect inflammatory causes of chronic diarrhoea, and stool cultures remain useful in distinguishing infection from other inflammatory causes of chronic diarrhoea. Faecal immunochemical testing (FIT) is a new method of detecting the presence of blood in faeces and can be used instead of the traditional faecal occult blood test (FOBT) where available.
In general, for patients with typical symptoms of functional bowel disease, normal physical examination, and normal screening investigations, a diagnosis of IBS can be made. However, referral should be considered for those with abnormal screening investigations or persistent symptoms that impact the quality of life and do not respond to initial treatment.
The main new guideline changes impacting primary care physicians are as follows:
Change in definition: chronic diarrhoea is now defined as ‘the persistent alteration from the norm with stool consistency between types 5 and 7 on the Bristol stool chart and increased frequency greater than 4 weeks’ duration’. Stool weight and daily stool frequency have been abandoned due to limited clinical value.
The use of FCP to exclude inflammation within the gut: in chronic diarrhoea where cancer is not suspected, it is now recommended that FCP should be tested in adults <40 years of age. Further guidance on interpreting abnormal FCP results and their management can be found in a recently published NHS England document, which has been endorsed by the National Institute for Health and Care Excellence (NICE).3
The use of FIT to detect colonic cancer: in patients with chronic diarrhoea suspicious of colonic cancer and without rectal bleeding, FIT is now recommended as a rule-out test to guide further investigations. There will be a move away from the older FOBT because FIT has a better diagnostic performance.
Dual-method testing for Clostridium difficile (C. diff): glutamate dehydrogenase enzyme immunoassay (EIA) or polymerase chain reaction, in combination with toxin assays, is now recommended for the diagnosis of C. diff. The combination provides higher negative and positive predictive values.
Recommendations for immunocompromised patients: consideration should be given to the possibility of immunodeficiency states presenting as chronic diarrhoea. If immunodeficiency is suspected, testing for human immunodeficiency virus (HIV) is recommended. If immunodeficiency is already established, norovirus or cryptosporidia should be excluded through stool testing.
Recommendations on anorectal disease: physicians are reminded to be vigilant for faecal impaction with overflow diarrhoea, especially in older people. In cases of faecal incontinence where conservative measures fail, it is recommended that patients be offered anorectal manometry and endoanal ultrasonography. Cross-sectional imaging with contrast is recommended if a fistula is suspected.
NEW CHANGES IN SECONDARY CARE INVESTIGATIONS THAT COULD AFFECT PRIMARY CARE
Younger age limits for lower GI endoscopy: If endoscopy is indicated, colonoscopy with ileoscopy and biopsy is now the preferred investigation without limitations in patient age; this was previously reserved for patients aged >45 years. However, in patients aged <40 years with functional symptoms, normal FCP, and in whom functional bowel disease is suspected, flexible sigmoidoscopy with biopsy is now recommended (previously for <45 years in age with atypical symptoms).
SeHCAT (tauroselcholic [75 selenium] acid) or fasting serum C4 (7α hydroxy-4-cholesten-3-one) testing are now recommended in patients with suspected functional diarrhoea: one in three patients with diarrhoea-predominant irritable bowel syndrome (IBS-D) has bile salt malabsorption. It is recommended that patients with SeHCAT value <15% or elevated C4 levels be trialled on a course of bile salt sequestrants. Empirical therapy may be trialled if both tests are unavailable.
Hydrogen breath testing or withdrawal of dietary lactose are now recommended if lactose maldigestion is suspected: no recommendations were made in the previous version.
Magnetic resonance imaging (MRI) enterography/enteroclysis or video capsule endoscopy are now the preferred imaging modalities to investigate small bowel disease: if both are unavailable, computed tomography (CT) may be used. Small bowel barium follow through and barium enteroclysis are no longer recommended due to poor sensitivity and specificity.
Glucose and lactulose breath tests are no longer indicated for the investigation of small bowel bacterial overgrowth (SBBO): this is due to the low sensitivity and specificity of these tests. Small bowel aspirates are recommended as the gold standard of diagnosis of SBBO. However, if this is not possible, empirical antibiotic therapy is recommended.
Faecal elastase is recommended to diagnose pancreatic insufficiency, and MRI (with magnetic resonance cholangio-pancreatography [MRCP] protocol) is recommended to diagnose chronic pancreatitis: CT is an alternative if MRI is not possible. If these investigations are normal, but the clinical suspicion remains high, endoscopic ultrasound (EUS) or MRCP with secretin is recommended.
Biopsies from the left and right colon should be taken to exclude microscopic colitis: microscopic colitis, a common cause of chronic diarrhoea in patients aged >50 years, often has a patchy distribution. Therefore one-sided colonic biopsies are no longer recommended.
LIMITATIONS
The main limitation of the new guidelines that is most relevant and impactful to primary care is the ambiguity surrounding recommendations for endoscopy. The new guidelines recommend:
‘In patients with typical symptoms of functional bowel disease, normal physical examination and normal screening blood and faecal tests (calprotectin), a positive diagnosis of IBS can be made.’
However, within the same set of recommendations it states:
‘In younger patients (<40 years) with a normal faecal calprotectin and in whom functional bowel disease is suspected, we recommend a flexible sigmoidoscopy.’
This was subsequently clarified with the authors,4 and in the latter group of younger patients (<40 years) they have recommended secondary care evaluation for patients with atypical, persisting, or severe symptoms of functional bowel disease5 even if the FCP is normal. Therefore, primary care physicians need not refer such patients for lower GI investigations directly but should refer these patients for specialist review in secondary care.
SUMMARY
Significant changes have been made to the previous guidelines that will undoubtedly improve the investigation of chronic diarrhoea in the community. A summarised flow diagram (Figure 1) has been created for physicians at the point of care for ease of use.
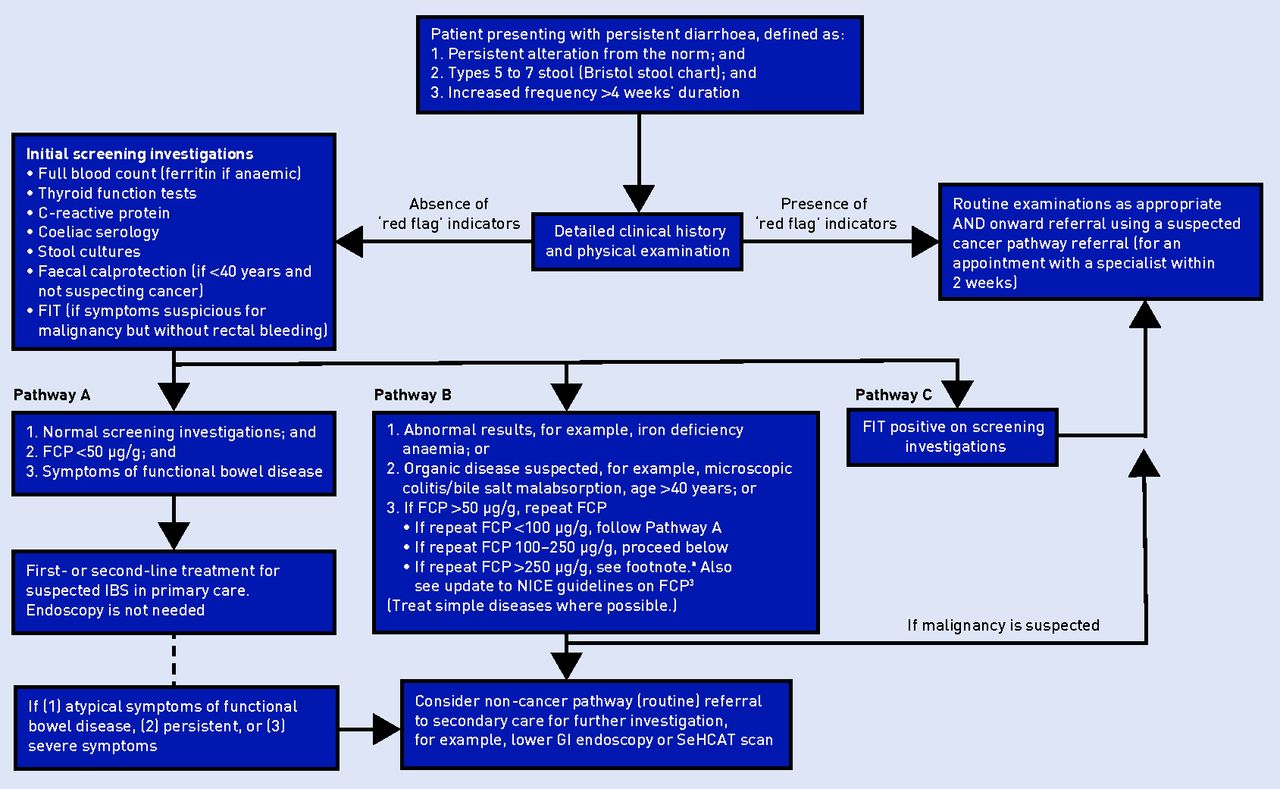
{kind=link}
Flow diagram for the investigation of chronic diarrhoea in primary care based on the 2018 BSG guidelines1and NICE recommendations.3aUrgent clinical review and referral to gastroenterology if FCP >250 μg/g on repeat sample or if acute severe IBD is suspected. BSG = British Society of Gastroenterology. FCP = faecal calprotectin. FIT = faecal immunochemical testing. GI = gastrointestinal IBD = inflammatory bowel disease. IBS = irritable bowel syndrome. NICE = National Institute for Health and Care Excellence. SeHCAT = tauroselcholic [75 selenium]acid
Acknowledgments
John Ong was supported by the WD Armstrong Doctoral Fellowship from the University of Cambridge. Communications and access to literature were supported by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust, King’s College London, and the University of Cambridge. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health.
Notes
Funding
None.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: www.bjgp.org/letters
- Received December 10, 2018.
- Revision requested December 14, 2018.
- Accepted December 20, 2018.
- © British Journal of General Practice 2019
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

