


Abstract
Background Comorbidity is a major public health issue, which challenges health care configured around single diseases.
Aim To provide an overview of frequent disease combinations of one and two additional chronic diseases and groups among patients with cardiovascular disease (CVD) in general practice.
Design and setting Medical record data from the Julius General Practitioners’ Network of 226 670 patients registered in 2015–2016 in Utrecht, the Netherlands, were collected and examined.
Method Prevalences and combinations of one and two comorbid conditions were determined, by age and sex, in four populations of patients with CVD: heart failure, peripheral arterial disease (PAD), coronary heart disease (CHD), or stroke. Using logistic regression analyses, the authors examined whether comorbid conditions were significantly more prevalent in patients with a specific cardiovascular condition compared with those without.
Results Low vision, diabetes mellitus, back/neck problems, osteoarthritis, chronic obstructive pulmonary disease (COPD), and cancer were the most prevalent non-cardiovascular conditions and ranked in the top five of non-cardiovascular comorbid conditions in the different CVDs studied, irrespective of patient age and sex. Of these, diabetes, COPD, and low vision were statistically significantly more prevalent in all four cardiovascular conditions when compared with patients without the respective disease. Over the life span, the majority of the comorbid conditions were most prevalent in patients with heart failure, directly followed by those with PAD; they were less prevalent in patients with CHD and stroke.
Conclusion Comorbid conditions are very common in patients with CVD, even in younger age groups. To ensure efficient and effective treatment, organisational adaptations may be required in the healthcare system to accommodate comorbid conditions in patients with CVD.
INTRODUCTION
Cardiovascular disease (CVD) remains the largest cause of mortality worldwide, despite a spectacular decline in age-specific cardiovascular mortality in Western societies over the last few decades.1 Improved primary prevention and pharmacological treatment of cardiovascular risk factors have resulted in a lower risk of cardiovascular events and a decrease in case fatalities.1,2 As a result, the age at which people have their first cardiovascular event has shifted to older age and patients live longer after the onset of CVD.3 Consequently, more patients with CVD have a higher life expectancy and are increasingly confronted with comorbid conditions — this makes this population of particular interest when studying comorbidity.
The presence of one or more co-occurring chronic diseases next to an index disease is defined as comorbidity.4 Comorbidity could potentially lead to poorer functional status, lower quality of life, and even increased mortality.5,6 Alongside the effects on patients, having multiple chronic diseases is also challenging for healthcare systems such as primary care because, traditionally, these are configured around single diseases. This fragmented point of view can potentially lead to conflicting medical advice and interacting medications.7
Nowadays comorbidity tends to be considered the rule rather than the exception, so increasing awareness and improving guidance for patients with comorbid conditions is crucial in order to prevent adverse health outcomes, increase efficiency, and reduce costs. One of the first steps in this process is to assess the prevalence of comorbidity in CVD and to provide a context for future research. Despite the large numbers of people with complex needs and the effect this has on health care being acknowledged, current evidence about whether the prevalence of different combinations of comorbid conditions differs between the sexes, and how the prevalence of comorbid conditions changes over the life span is lacking. In addition, most studies have investigated disease pairs,5,8 whereas patients with CVD often have more than two comorbid conditions.9,10
The objectives of the present study were, therefore, to describe the prevalence and associations of comorbid conditions in patients with CVD, by age and sex. The aim was that results from this and other studies could then be used to identify and prioritise combinations of diseases that would benefit most from further research. Insight into these phenomena can help improve healthcare management for patients with multiple diseases and target healthcare resources.
METHOD
Study design and data source
Data from the Julius General Practitioners’ Network (JGPN) database was used. The database contains anonymously extracted electronic medical records (EMRs) from all patients registered in 53 general practices in the Utrecht area of the Netherlands. In the Netherlands, all inhabitants (except older people in nursing homes) are obliged to be registered with a general practice and the GP acts as gatekeeper to hospital and specialised care. As such, Dutch general practice data are likely to be a reliable reflection of the health status of most of the population. The JGPN population is considered representative of the Dutch population with regards to sex and age.11
How this fits in
Nowadays, comorbidity is considered the rule rather than the exception. As well as the effects on individual patients, comorbidity presents added challenges for healthcare systems, such as primary care, as these are traditionally configured around single diseases. Despite large numbers of patients with, for example, cardiovascular disease and comorbidity, and the acknowledgement of its effect on health care, current evidence is lacking on whether prevalence of different combinations of comorbid conditions varies between males and females, and how prevalence of comorbid conditions changes over life span. The study findings may help guideline developers to identify relevant subgroups, to inform researchers and research funders which comorbid conditions are most prevalent and may require prioritisation, and may target healthcare resources for patients with multiple conditions.
This study was conducted in accordance with the privacy legislation in the Netherlands and the regulations of the Dutch Data Protection Authority.
Study population
The present study used data from 226 670 persons of ≥18 years, who were registered for at least 1 year after 1 January 2015. Diagnoses were coded by the GP according to the International Classification of Primary Care (ICPC). The EMR data of the patients were screened for the presence of different diagnostic codes from 1 January 2008 onwards, or from the date the patient was registered with the GP practice if they were enrolled after 1 January 2008. It was established whether the patients had any of the following cardiovascular conditions:
heart failure (ICPC: K77);
peripheral arterial disease (PAD) (ICPC: K92, K99.01–K99.03);
coronary heart disease (CHD) (ICPC: K74–K76); or
cerebrovascular accident (stroke) (ICPC: K90).
The specific cardiovascular condition for which the patient was included in the study sample will be referred to as the ‘index disease’. A distinction was made between cardiovascular comorbidity and non-cardiovascular comorbidity. Cardiovascular comorbid conditions included the same cardiovascular conditions as the index diseases. Non-cardiovascular comorbid conditions were selected based on a standard list of chronic diseases for primary care;12 it was established whether patients had any of these, which comprised asthma (ICPC: R96), back/neck problems (including hernia, spondylarthritis and scoliosis — ICPC: L83–L86), cancer (ICPC: A29, B72, B73, D74, D75, D77, L71, N74, R84, R85, S77, T71, U75–U77, W72, X75–X77, Y77), chronic obstructive pulmonary disease (COPD) (ICPC: R91, R95), colitis (ICPC: D94), congenital abnormalities of the central nervous system (ICPC: N85), dementia (ICPC: P70), depression (ICPC: P76), diabetes mellitus (ICPC: T90), epilepsy (ICPC N88), hearing impairment (ICPC: H84, H54), HIV/AIDS (ICPC: B90), intellectual impairment (ICPC: P85), low vision (retinopathy, macular degeneration, glaucoma, cataract, blindness — ICPC: F83, F84, F92, F93, F94), multiple sclerosis (ICPC: N86), osteoarthritis (ICPC: L89–L91), osteoporosis (ICPC: L95), Parkinson’s disease (ICPC: N87), rheumatoid arthritis (ICPC: L88), schizophrenia (ICPC: P72), and tuberculosis (ICPC: A70).
Analyses
The characteristics of the total study population and of those with at least one of the index diseases were described. The prevalence of the different comorbid cardiovascular and non-cardiovascular chronic diseases among the four patient groups with an index disease was examined. To investigate whether these comorbid conditions were more prevalent among patients with a specific index disease compared with those without it, odds ratios with corresponding 95% confidence intervals (95% CIs) were calculated using logistic regression analyses adjusted for age and sex. The comparison groups involved the total study population minus the patients with the respective index disease. If a patient had more than one index disease, for example, heart failure and CHD, they were included in both index disease groups. In addition, the prevalence of having cardiovascular and non-cardiovascular comorbid conditions was examined among the four index disease groups by age and sex. Age groups were 18–54 years, 55–74 years, 75–84 years, and ≥85 years. All analyses were performed using SPSS (version 22.0).
RESULTS
In the total cohort of 226 670 patients, 15 787 patients with CVD were identified. This comprised 9487 patients with CHD, 3290 patients with heart failure, 3261 patients with stroke, and 2846 patients with PAD (Table 1). The mean age was 68 years (standard deviation [SD] 13 years) for males with CVD and 71 years (SD 15 years) for females with CVD; the mean age was much lower in the total population (mean: 46 years (SD 18)). CHD was the most common cardiovascular condition, with a prevalence of 4% in the total population, but 66% and 53% of males and females respectively had CVD. The median follow-up time was similar for all groups (Table 1).
Participants’ characteristics
Non-cardiovascular comorbidity
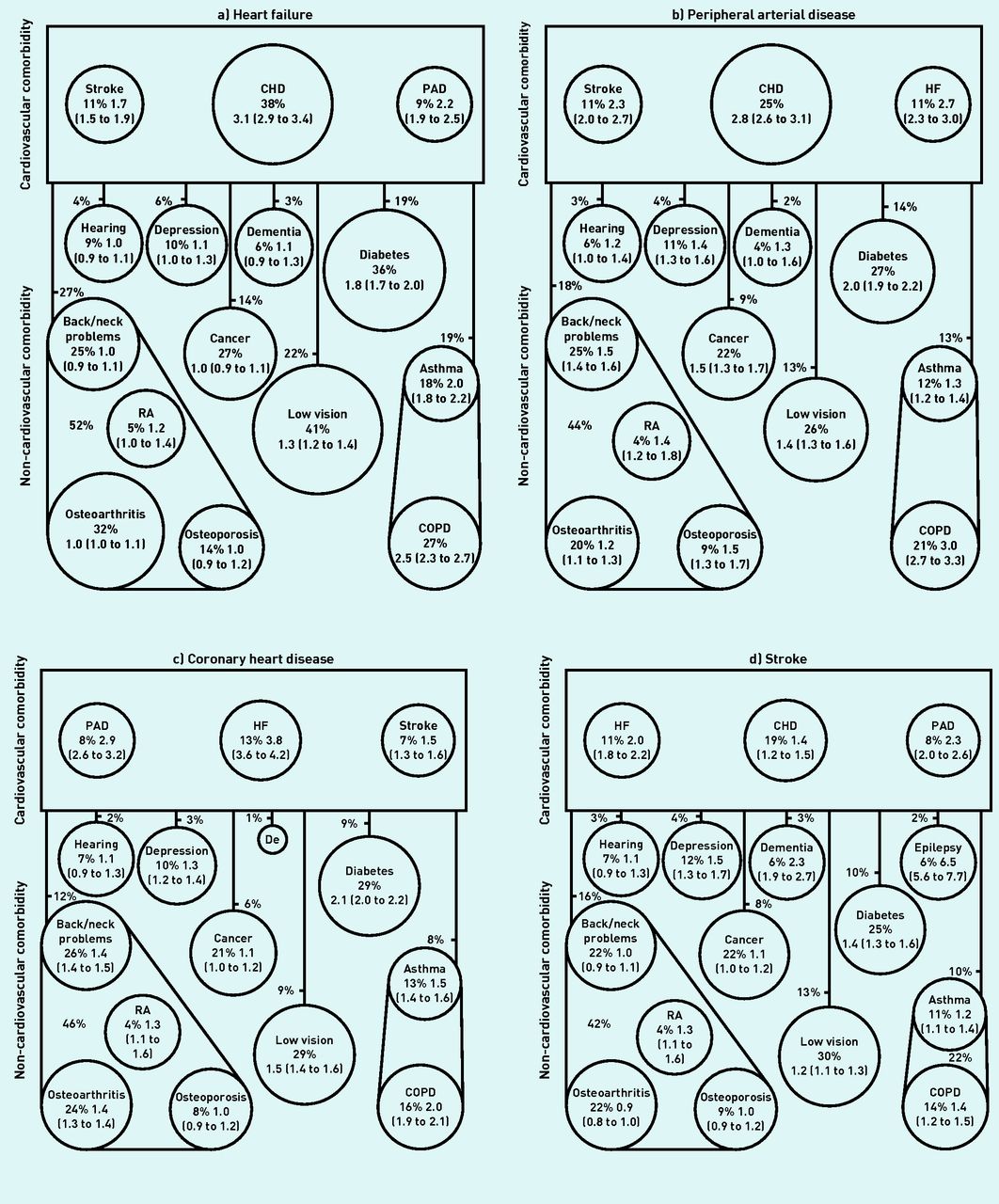
Low vision, diabetes, back/neck problems, osteoarthritis, COPD, and cancer were the most common non-cardiovascular conditions and were among the top five non-cardiovascular comorbid conditions in all groups of patients with CVD (Figure 1). Of these, in age- and sex-adjusted analyses, diabetes, low vision, and COPD were statistically significantly more prevalent in patients with any of the cardiovascular index diseases when compared with patients without those cardiovascular conditions. In addition, asthma was also statistically significantly more common in those with CVD than those without (data not shown).

{kind=link}
Cluster diagram of the most common comorbid conditions in patients with a) heart failure, b) peripheral arterial disease, c) coronary heart disease, and d) stroke. Each circle gives the crude prevalence, followed by the odds ratio and 95% CI, adjusted for age and sex. Percentages next to lines that connect the cardiovascular comorbid disease group with other diseases or disease groups represent the prevalence of having both a cardiovascular comorbid condition as well as the non-cardiovascular condition. Percentages not connected to a line or circle indicate the prevalence of the muscular diseases grouped. As an example, 19% of the patients with heart failure have both an additional cardiovascular disease as well as diabetes mellitus. Only prevalences >2.5% are shown. Circle size is proportional to the prevalence. CHD = coronary heart disease. COPD = chronic obstructive pulmonary disease. De = dementia. HF = heart failure. PAD = peripheral arterial disease. RA = rheumatoid arthritis.
In patients with stroke, the prevalence of most comorbid conditions appeared to be somewhat lower than in patients with other index diseases (Table 1). Epilepsy, however, was more prevalent in patients with stroke (6%) than the other index diseases (<2.5%, Figure 1). Osteoarthritis was a highly prevalent comorbid condition, with a prevalence of 32% among patients with heart failure (Figure 1); when all musculoskeletal diseases (back/neck problems, osteoarthritis, osteoporosis, and rheumatoid arthritis) were grouped, this percentage increased to 52%. The prevalence of a number of non-cardiovascular comorbid conditions appeared to be highest for patients with heart failure compared with other cardiovascular conditions (Figure 1).
Cardiovascular comorbidity
CHD was the most common cardiovascular comorbid condition in patients with heart failure (38%), PAD (25%), and stroke (19%); in patients with CHD, heart failure was the most common cardiovascular comorbid condition (13%) (Figure 1). In age- and sex-adjusted analyses, all cardiovascular comorbid conditions were more prevalent in those with a cardiovascular index disease compared with patients without the respective cardiovascular condition (Figure 1). Patients with heart failure had the highest prevalence of cardiovascular comorbid conditions, followed by those with PAD (Figure 1). In total, 27% of the patients with heart failure had both a cardiovascular comorbid condition and a musculoskeletal disease, compared with 18%, 16%, and 12% in patients with PAD, stroke, and CHD, respectively (Figure 1).
Comorbid diseases over the life course in males and females
Aside from asthma and depression being included in the top five comorbid diseases in the youngest age group (18–54 years), low vision, diabetes, back/neck problems, osteoarthritis, COPD, and cancer were also the most common non-cardiovascular comorbid conditions when data were stratified by age and sex (Table 2). This also applied to epilepsy in patients aged 18–54 years who had previously had a stroke. Although less prevalent compared with the older age groups, relatively high prevalences — for example, for diabetes and COPD — were observed in the youngest age group. Depression was, in general, more prevalent in younger age groups compared with older age groups. Osteoarthritis, low vision, and cancer became more prevalent with increasing age. The most notable difference between males and females was that musculoskeletal diseases were more prevalent in females (Table 2).
Prevalence of cardiovascular comorbid conditions and top 10 most common non-cardiovascular comorbid conditions in patients with heart failure, peripheral arterial disease, coronary heart disease, and stroke (stratified by age and sex)
DISCUSSION
Summary
In this study it was observed that low vision, diabetes mellitus, back/neck problems, osteoarthritis, COPD, and cancer were the most common non-cardiovascular comorbid conditions among patients with heart failure, PAD, CHD, and stroke, irrespective of age and sex. Comorbid conditions were most prevalent in patients with heart failure, and appeared to be lower in patients with stroke.
Strengths and limitations
The strengths of this study include the large sample size, which enabled comorbidity to be examined in strata of age and sex. With the exception of some older people who live in nursing homes, all Dutch inhabitants are obliged to be registered with a general practice; as such, the data used in this study are likely to be a good reflection of the health status of the population. However, it should be noted that a disease is only regarded as present when the patient actually visits the GP and the GP diagnoses the patient with the respective disease. This may have led to the prevalence of conditions for which patients may not consult their GP — for example, depression — being underestimated. Furthermore, because older people in nursing homes are usually not registered with a general practice, it is to be expected that a disease such as dementia may be underrepresented. As people residing in nursing homes have high levels of frailty and comorbid conditions, the results of this study are not generalisable to them; this group comprises 0.7% of the total Dutch population.13 In addition, as socioeconomic deprivation is an important risk factor for comorbidity,5 it may be expected that the prevalence of comorbid conditions is higher in patients with CVD who have a lower socioeconomic status. Unfortunately, this study did not include information about socioeconomic status and so this could not be taken into account.
Comparison with existing literature
Previous studies confirm the finding that comorbid conditions are particularly prevalent in patients with heart failure.10,14–16 Another study in the general Dutch population observed that patients with heart failure had the highest prevalence of comorbidity (92%) compared with those with other cardiovascular conditions such as stroke (81%) and CHD (80%).14 In addition, patients with heart failure more often also have both a cardiovascular comorbid condition and a non-cardiovascular comorbid condition simultaneously. In the current study, there was a high prevalence of heart failure combined with both a cardiovascular comorbid condition and a musculoskeletal disorder, and heart failure combined with both a cardiovascular comorbid condition and asthma, and/or COPD.
Studies investigating disease triplets are more scarce than studies investigating disease pairs. However, a study by Sinnige et al showed results in the same vein, with high prevalences for heart failure–coronary artery disease–COPD and heart failure–coronary artery disease–osteoarthritis.15
The study presented here confirms findings of previous studies that low vision, diabetes, back/neck problems, osteoarthritis, COPD, and cancer are very common non-cardiovascular conditions among patients with heart failure, CVD, and stroke.14,15 Those results were extended in this study and it was shown that these diseases were also the most common conditions in patients with PAD; in addition, these diseases also appeared to be the most common non-cardiovascular comorbid conditions in different age groups and affected males and females similarly. Musculoskeletal diseases were, however, more prevalent in females compared with males — this is also supported by previous literature.16–18
Low vision, diabetes, COPD, and asthma were statistically significantly more prevalent in all cardiovascular conditions when compared with patients without that respective cardiovascular condition in age- and sex-adjusted analyses. This may be explained by the fact that these diseases all share risk factors similar to those for CVD. Patients with type 2 diabetes have a higher prevalence of ‘traditional’ risk factors for CVD, such as dyslipidaemia, abdominal obesity, smoking, and physical inactivity — next to these, diabetes is possibly further associated with CVD through a mechanism that includes long-term hypertension, chronic hyperglycaemia, microvascular disease, glycosylation of myocardial proteins, diabetic nephropathy, and autonomic neuropathy.19 Similarly, COPD and CVD also share risk factors such as smoking. It is suggested that COPD is also linked to heart failure due to low-grade systemic inflammation,20 which may explain the high prevalence of COPD in patients with heart failure in the study presented here.
The finding that low vision is statistically significantly associated with CVD is in accordance with previous studies.21,22 Again, a suggested hypothesis for this association is that the conditions share risk factors, such as smoking.21 On the other hand, a previous study showed a strong association between visual impairment and the 10-year risk for a first atherosclerotic disease event, even after adjustments for traditional risk factors.22 It could be that an as-yet-unknown pathological pathway between visual impairment and CVD exists.
In the current study, a strong relation between stroke and epilepsy was also observed. This finding is in accordance with previous literature which showed that patients with an intracerebral haemorrhage in particular have a high risk of developing epilepsy.23
Implications for research and practice
The results of this study underline the high prevalence of comorbid conditions in patients with CVD. These results can act as a starting point in the revision of medical guidelines to ensure they are more suitable for patients with CVD and comorbid conditions. At present, guidelines are predominantly based on trial populations that differ from the primary care population in terms of comorbidity prevalence and age.24,25 This study’s results may shape the development of prescribing policy for highly prevalent disease combinations. Additionally, it may inform researchers of those comorbid conditions that are most prevalent and may require prioritisation, in terms of studying how they affect the management of the respective cardiovascular index condition. The current study showed that patients with heart failure are most often burdened by comorbid conditions, irrespective of age and sex; this area could perhaps be prioritised for future investigations, such as developing interventions that aim to align health care to the needs of the growing number of patients with heart failure and comorbid conditions.
There is a great need for studies investigating how to organise care and manage patients with comorbidity; although such studies are becoming increasingly more prevalent, evidence on the effectiveness of the interventions remains inconclusive due to the relatively small numbers of randomised controlled trials and the mixed overall results.26 The results of a systematic review by Smith et al showed that interventions in primary care targeted at comorbid depression may be effective.26 Although many of the included studies were restricted to patients in older age groups, the study presented here revealed that depression is particularly prevalent in younger patients.
The National Institute for Health and Care Excellence created a guideline on clinical assessment and management of patients with multimorbidity;27 this offers GPs guidance on how to prioritise treatment and may help to establish which non-pharmacological treatments could best be initiated, reduced, or stopped.28 In line with this, principles to guide decision making when dealing with comorbidity during primary care consultations have been developed.29 These principles describe how a patient’s conditions and treatments, and prioritising health problems that take into account their preferences, may determine realistic treatment goals that are shared by the patient and the GP.29 However, a 10–15 minute consultation may be too short to provide such care to patients who have many comorbid conditions.30 It seems plausible that a longer consultation could result in more preventive health advice and increased patient satisfaction. However, a review from 2016 investigating this subject only included five trials and all studies had methodological weaknesses,31 hence, further research is still needed.
The results presented here showed that the top five most prevalent comorbid diseases next to CVD did not change much over the life span and between sexes. GPs should be aware that diseases such as diabetes and COPD, however, are not limited to older patients with CVD, but are already prevalent in their younger counterparts. Additionally, disease management programmes are implemented for an increasing number of chronic diseases including CVD; GPs should consider including patients with comorbidity in these. Given the largely single-disease focus of these programmes, they may be less useful for patients with comorbid conditions that interact in the treatment and management of the disease of main interest.
Notes
Funding
This work was supported by a grant from the Dutch Heart Foundation (grant DHF project ‘Facts and Figures’).
Ethical approval
Not applicable. Anonymised data; no ethical approval necessary. This study was conducted in accordance with the privacy legislation in the Netherlands and the regulations of the Dutch Data Protection Authority.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received February 23, 2018.
- Revision requested April 19, 2018.
- Accepted June 15, 2018.
- © British Journal of General Practice 2019
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

