


INTRODUCTION
Echocardiography (echo) is central to the assessment and management of all cardiac diseases. An echocardiogram is produced using ultrasound waves to create a moving picture of the heart. It is the innate advantages of this medium (sound waves are harmless and painless, and portable systems allow convenience with instant, reproducible results) that allows its use to continue to flourish widely beyond traditional hospital settings. Increasing patient multimorbidity resulting from an ageing population is driving an increase in demand for echo. In the UK for the last decade there has been approximately a 3% annual growth in the number of echocardiograms performed.1 This necessitates an expansion and diversification of echo services, and this has been recognised in the NHS Long Term Plan, which has identified primary care as an area to try to meet this demand and improve diagnosis of heart failure and heart valve disease (HVD).2 Here we discuss how echo is currently used in primary care, training pathways for GPs, and how developments in the field can lead to innovative and cost-effective echo services to benefit our patients.
THE DIFFERENT DELIVERY MODELS
The portability of echo machines had resulted in many community echo clinics across the UK where patients attend a community centre for a full echo study, just as they would have in hospital departments. There are several different models of delivery. One is via an independent third-party provider who may be able to provide appropriately trained individuals to deliver the service. In other models, the local hospital department delivers clinics within the community setting. This has the added advantage of offering educational opportunities to GPs with an interest in echo, but more importantly provides clinical governance via the hospital department delivering the service and the potential to reduce the repeat diagnostic testing of patients who are referred into secondary/tertiary hospitals.
Other community services utilise appropriately trained GPs with a specialist interest in cardiology to perform the scans as part of wider community cardiology services (with one general practice even employing its own physiologist). This brings echo directly to the point of care and allows echo to be integrated into the assessment of a broad range of patients presenting with complaints such as non-specific breathlessness, including in the patient’s own home (Figure 1). In the right hands, echo in this setting can be used to rule out significant left ventricular (LV) dysfunction, pericardial effusion, and pleural effusion, among other serious pathology. However, there are significant financial issues, with appropriately sophisticated portable machines costing somewhere in the region of £40 000 before consideration of maintenance costs. Therefore a process for financial reimbursement through local commissioning channels is mandatory for individual GP practices to consider investment. With the increase in GP clusters and collaborations, point-of-care echo could be provided by a small number of GPs in close conjunction with the local cardiology departments within each locality.
{kind=link}
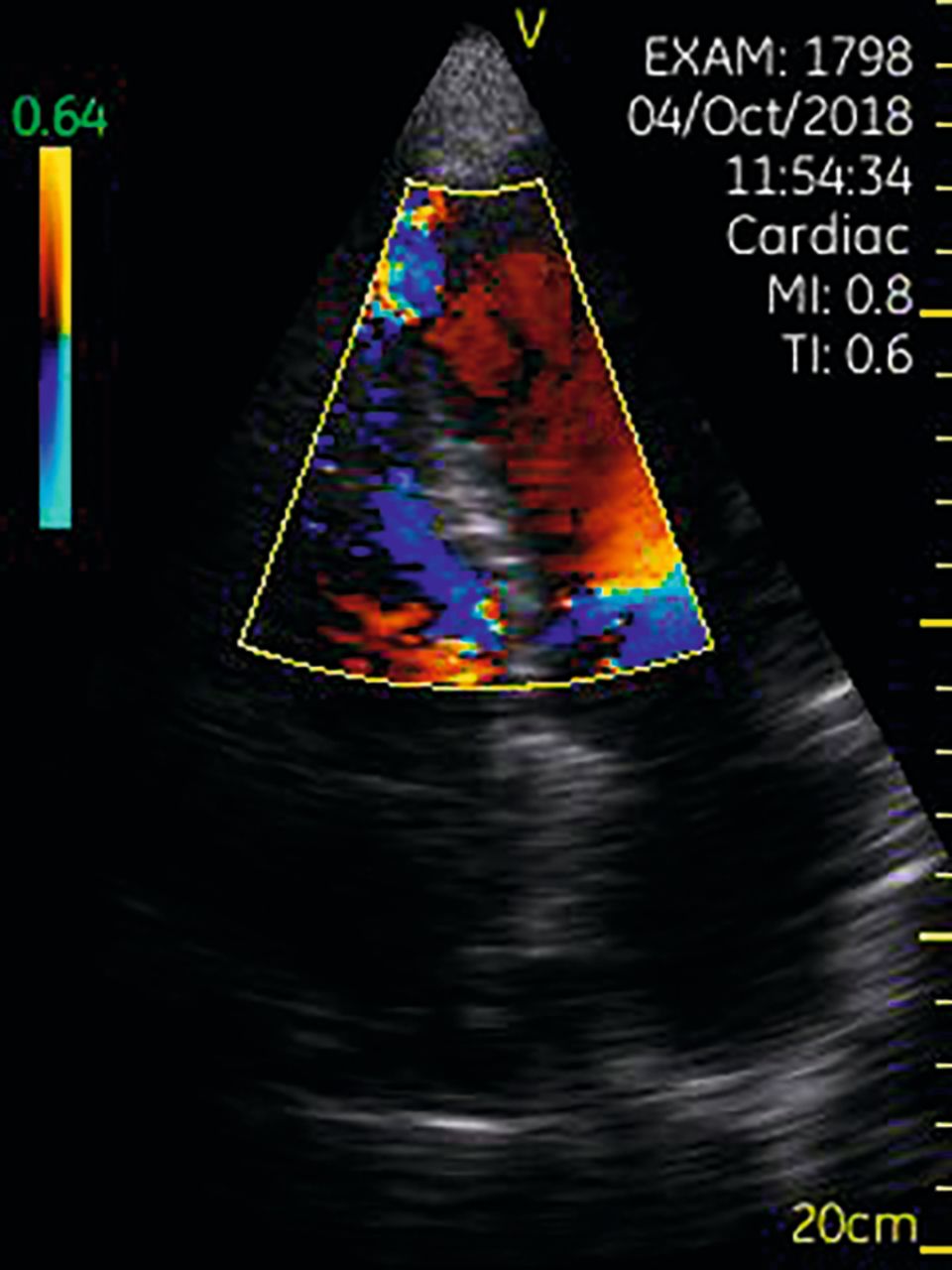
A ventricular septal defect due to a recent myocardial infarction. The patient presented with breathlessness and the echo was performed on a portable device in the patient’s home. It allowed direct referral to the appropriate secondary care team.
INTEGRATION INTO CLINICAL ASSESSMENT
Heart failure prevalence continues to increase and diagnosis can be challenging. This potentially leads to long delays between presentation and specialist assessment.3 Broadening the access to natriuretic peptide testing and echo in primary care could potentially improve the accessibility to specialist input and in turn expedite decisions for implementing disease-modifying therapy. To achieve this, there has been some interest and research in training non-specialists to capture focused images and using visual assessment to identify LV systolic dysfunction above and beyond usual clinical assessment.4 This is not without caution given that assessment of LV function is the most difficult assessment made by specialists who are experts in this field. The attractiveness of small hand-held devices costing less than £5000 is that they have the capability to capture satisfactory images for visual assessment of LV function, which may have the advantage of being easy to implement at scale, through a network of interested GPs covering a large population. We must, however, ensure a quality service is deliverable and not just a quantity service plan.
Although studies have been small, it does seem feasible to train GPs to assess for particular pathology and this can be supported with ‘tele-echocardiography’. This has been shown to improve diagnostic accuracy after images are acquired by a non-specialist with limited training5 and remotely reviewed by an expert. However, the main limitation of this approach is that hand-held devices are currently only able to confidently detect or rule out significant LV systolic, and not diastolic, dysfunction. This is important as diastolic heart failure is a common cause of breathlessness in older hypertensive populations.
Aortic stenosis (AS) is the most common valve pathology requiring surgery but patients are frequently diagnosed far too late, with a poor prognosis following the onset of symptoms. Auscultation of the heart has poor sensitivity and specificity for diagnosis of valvular heart disease.6 The ability to use a hand-held device to detect significant abnormalities of the aortic valve can be taught to GPs. A specific patient group with risk of AS (ageing, hypertension) could then be screened by GPs either systematically or opportunistically. Again, this assessment pathway could be performed by non-specialists at a broad scale using a ‘hub and spoke’ model through each integrated care system. Artificial intelligence (AI) may have a future role to play in further improving accuracy here and has shown promising results.7 As these AI programmes improve, it could further reduce the concern about training non-specialists in echo.
ACCREDITATION AND TRAINING
Despite potential advantages, training and continued professional development in echocardiography are crucial to its safe use in any healthcare setting. Without a robust process for certification, accreditation, and revalidation, the potential for risks to patients by inexperienced staff using poor equipment are high and must be minimised. It would rely on national consensus on the safe use of echo in primary care to protect patients and clinicians. Currently, the British Society of Echocardiography (BSE) promotes quality echo systems in primary and secondary care, and provides accreditation pathways for GPs to gain formal accreditation and demonstrate ongoing exposure to maintain proficiency. This necessitates the GP to perform a large volume of scans to reach an agreed accreditation standard and show continued development to re-accredit every 5 years. Obtaining accreditation can be a challenge for any busy clinician and starting the accreditation pathway during a GP specialty training is helpful. Indeed, the new GP training contract allows ample time for self-directed training, and hospital departments are often willing to mentor GPs during their echo development.
CONCLUSION
Echocardiography is an extremely powerful diagnostic instrument. When used carefully by the appropriate clinician and on the right patient, it can have immense benefits to patients presenting with cardiovascular symptoms in primary care. Indeed, as discussed above it could one day become integrated into the clinical assessment of patients presenting with breathlessness or optimising assessment of a murmur at an affordable cost. It can also be used for patients describing acute symptoms of potentially serious cardiac disease, even in the patient’s own home, allowing direct referral to the most appropriate secondary care team. Yet the risks of its indiscriminate use must be mitigated through careful training and demonstration of continued practice. If training and safety aspects are satisfactorily allayed, echocardiography can be successfully and widely used in primary care to the benefits of our patients.
Notes
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
- © British Journal of General Practice 2019
In this issue









Jump to section

