


INTRODUCTION AND PREVALENCE
Thyroid nodules are very common in the adult population. In the Framingham study, clinically apparent thyroid nodules were present in 6.4% of females and 1.5% of males.1 There may be even more thyroid nodules that are undetected, and postmortem studies demonstrate thyroid nodules in half of all patients.2 Many nodules can be managed in primary care, but some patients will require referral to secondary care. The aim of this article is to arm a GP with the information required to confidently assess which patients require referral, and in what timeframe.
INCIDENTAL FINDING OF THYROID LUMPS
The gap between the 1.5–6.4% of palpable nodules found in the Framingham study and the 50% found at post-mortem implies that there is an enormous volume of nodules that are not clinically apparent. With the development of increasingly sophisticated imaging modalities there has been an epidemic of thyroid ‘incidentalomas’. These non-palpable nodules are seen in at least 20% of ultrasound scans, 25% of contrast-enhanced chest CTs, 15% of MRI neck scans, and 30% of PET-CT scans.3 Most patients with incidentally discovered thyroid nodules can be managed by the same principles of history and examination as those with palpable lumps. There are two exceptions to this rule, the first being incidental thyroid lumps on CT, MRI, or ultrasound scan (USS) that are <1 cm and have no associated lymphadenopathy. There is no need for further investigations or referral of these lesions unless there are specific adverse or concerning features.4 This is because, even in the minority of these nodules that represent a cancer, tumours <1 cm are typically indolent and are associated with a 10-year survival of greater than 99.99%.5 Failure to diagnose a thyroid cancer at this size is therefore not material to a patient’s long-term outcomes. The second exception is that any thyroid nodule which is reported to be an avid lesion on FDG–PET CT should always be referred urgently as a suspected cancer. Of these, 30–40% will represent a thyroid cancer and, as such, should be investigated in virtually all cases.6
HISTORY
GPs are well versed in eliciting a history of thyroid status, whether hypo- or hyper-, and this should be covered with the usual screening questions. The history of a thyroid lump should also cover both symptoms associated with the lump and previous personal and family history that may raise concern of thyroid cancer (see Box 1 for immediate red-flag symptoms). If there are no features in the history or examination that merit onwards referral as a possible cancer, it is also useful to ask specifically about the presence of compressive symptoms. This is because patients with benign nodules causing significant detriment to their quality of life may benefit from a routine referral to the local thyroid team.
|
Red flags that may prompt urgent referral
Thyroid status
Hyperthyroid — hot, anxious, tremulous, palpitations.
Hypothyroid — cold, low energy, depression, constipation.
History of the lump
Is this a new lump, or a change in a pre-existing lump? Sudden painful expansion of a pre-existing lump almost always represents haemorrhage into a colloid cyst and the patient should not be alarmed. By contrast, an older patient with a rapid expansion of a painless thyroid mass should raise alarm, particularly if associated with any red-flag symptoms.
Compressive symptoms associated with the lump; dry nocturnal cough, globus, or dysphagia. However, for the thyroid to cause dysphagia there must be a substantial goitre to effectively pincer the oesophagus between the two lobes.
Associated neck lumps noted by the patient.
Changes in voice.
Risk factors for thyroid cancer
Age <16 years: all children should be referred for investigation of thyroid lumps.
History of radiation to the neck.
Childhood spent in proximity to a nuclear fallout zone (for example, Chernobyl).
Family history of thyroid cancer: multiple endocrine neoplasia is an uncommon but important cause of thyroid cancer.
EXAMINATION
General: clinical assessment of thyroid status; stridor; hoarseness.
Lump: thyroid palpation; ideally comment on size, fixity to underlying structures, consistency (for example, rocky hard; fluctuant); palpation of central and lateral neck.
DIFFERENTIAL DIAGNOSES
Benign (80% of all thyroid lumps): colloid nodule; hyperplastic nodules; thyroid adenoma; dominant nodule within a multinodular goitre.
Malignant: primary thyroid malignancies — differentiated (papillary, follicular), medullary, and undifferentiated (anaplastic); lymphoma; metastatic deposits from sites such as the breast, kidney, or prostate.
INVESTIGATIONS
Thyroid function tests (TFTs) rarely yield useful information about the nature of a thyroid nodule. However, baseline TFTs are useful in managing a patient where there is clinical suspicion of hypo- or hyperthyroidism, and to aid further management for those who need onwards referral.
No further investigations are routinely required in primary care.
ONWARDS REFERRAL
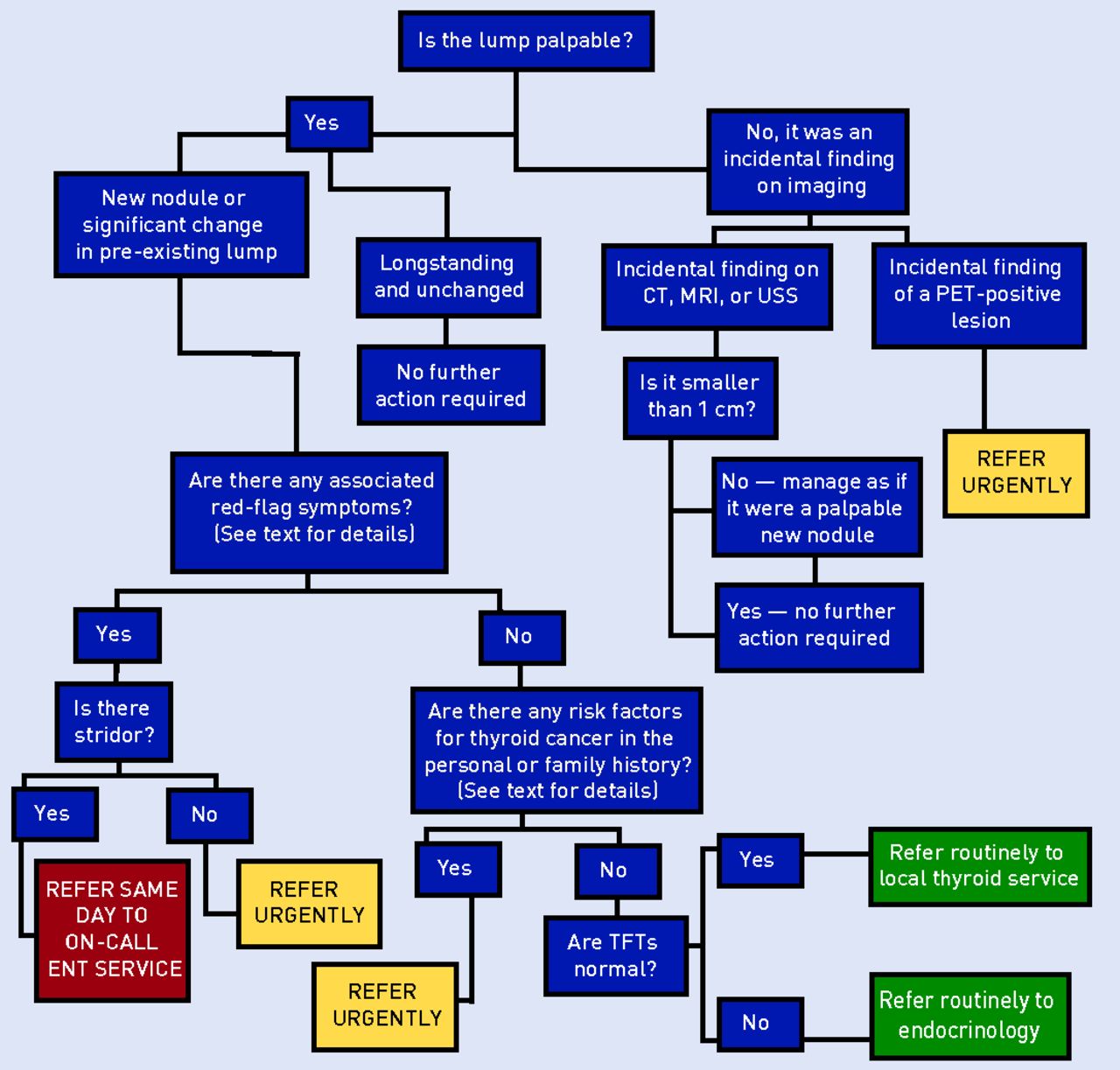
Figure 1 is a guide to patient referral based on guidance from the British Association of Endocrine and Thyroid Surgeons7 and the American College of Radiology.4 Clearly this is only a guide and discretion should be used if there appear to be sinister features that cannot adequately be explained, or if a patient has a very short predicted life expectancy.

{kind=link}
A guide to referral for patients with thyroid lumps. TFT = thyroid function test.
INFORMATION FOR THE PATIENT
Patients who do not meet the criteria for referral should be reassured that thyroid nodules are an incredibly common phenomenon in the population and should be considered a variant of normal.
Patients who are referred for suspected cancer will be understandably anxious, but should be reassured that only a minority of thyroid lumps are cancer. They should be informed that in secondary care they will be seen by a thyroid surgeon and will undergo further investigation by means of an ultrasound and possibly fine-needle aspirate cytology. The results are used to risk-stratify the lump and direct further treatment. For the minority of patients who do have a malignancy, the prognosis for differentiated thyroid cancer is generally excellent,7 and treatment is associated with lower morbidity than many other oncological protocols. Treatment is predominantly surgical, by hemi- or total thyroidectomy. Some patients may require extended surgery to include lymph nodes or radioiodine remnant ablation (RRA). RRA is a short course of treatment, usually taking less than a week to complete. It causes very few side effects. Pertinently, however, female patients wishing to start a family after radioiodine must wait 12 months and males must wait 6 months.
For patients who wish to read more about their condition, the British Thyroid Foundation (http://www.btf-thyroid.org/) has an excellent range of resources available online. Additionally, for patients with thyroid cancer the Butterfly Thyroid Cancer Foundation (http://www.butterfly.org.uk/) has specific information about the diagnostic and treatment journey.
Notes
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received February 8, 2019.
- Revision requested February 26, 2019.
- Accepted March 25, 2018.
- © British Journal of General Practice 2019
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

