


Article Figures & Data
Figures
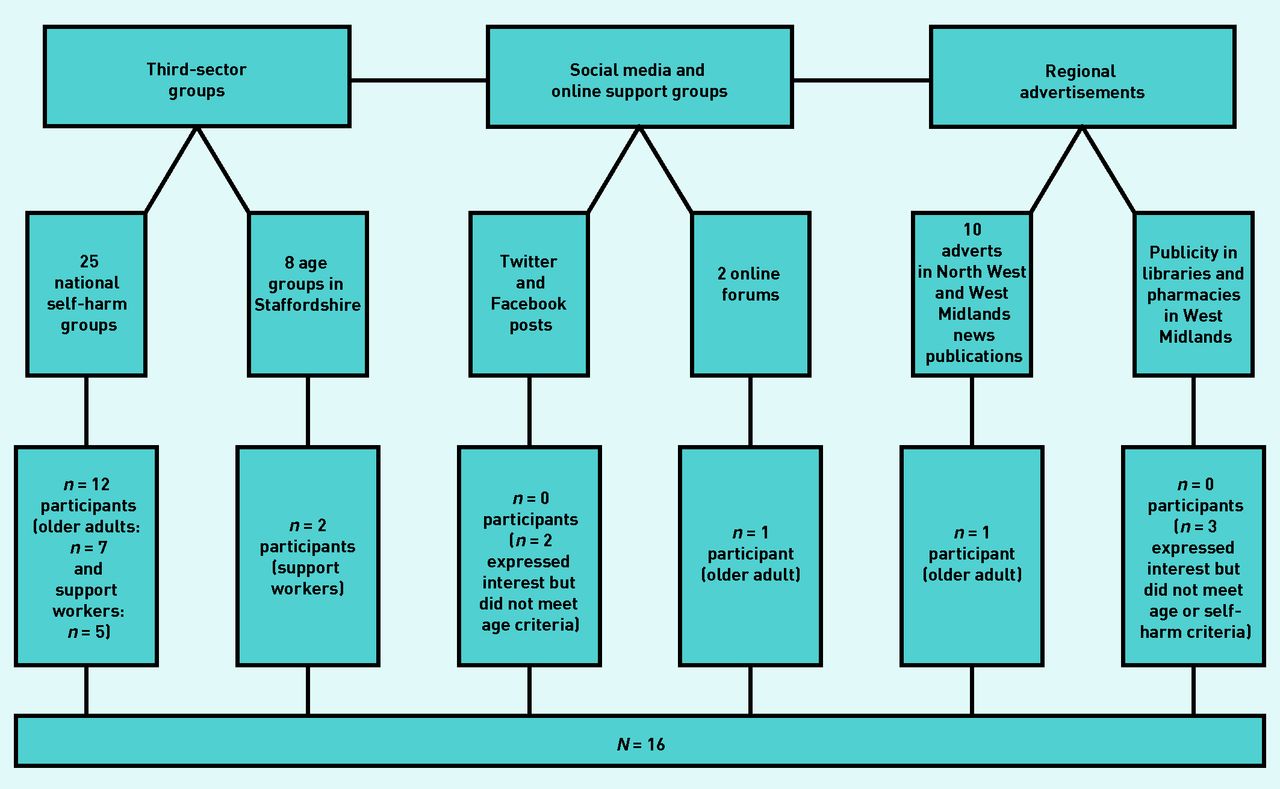
- Figure 1.
Flowchart of recruitment methods.
- Figure 2.
Summary of data analysis process.
aThe research team discussed interpretation if adjustment of analysis was needed when data were inconsistent with initial analysis. PPIE = patient and public involvement and engagement.
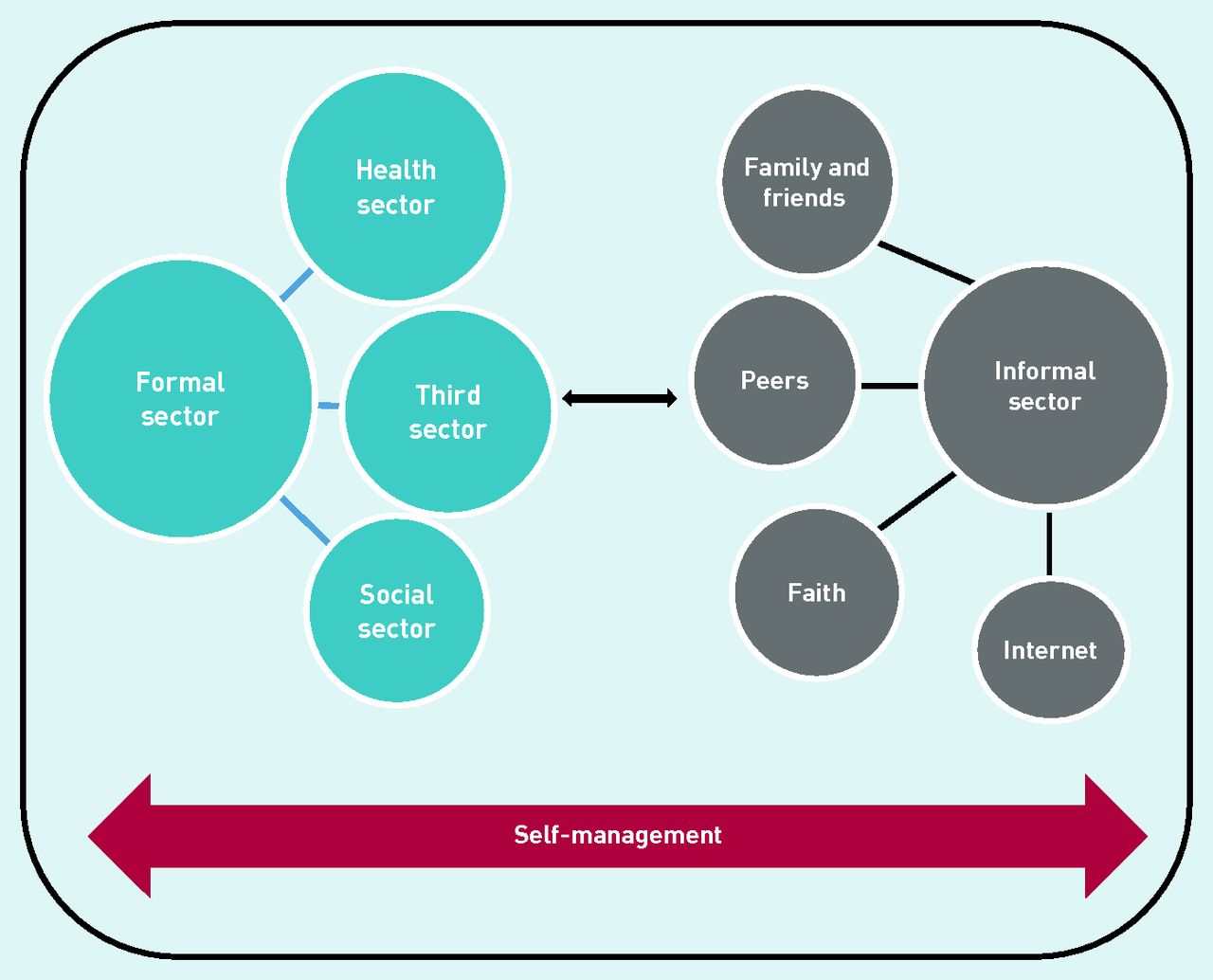
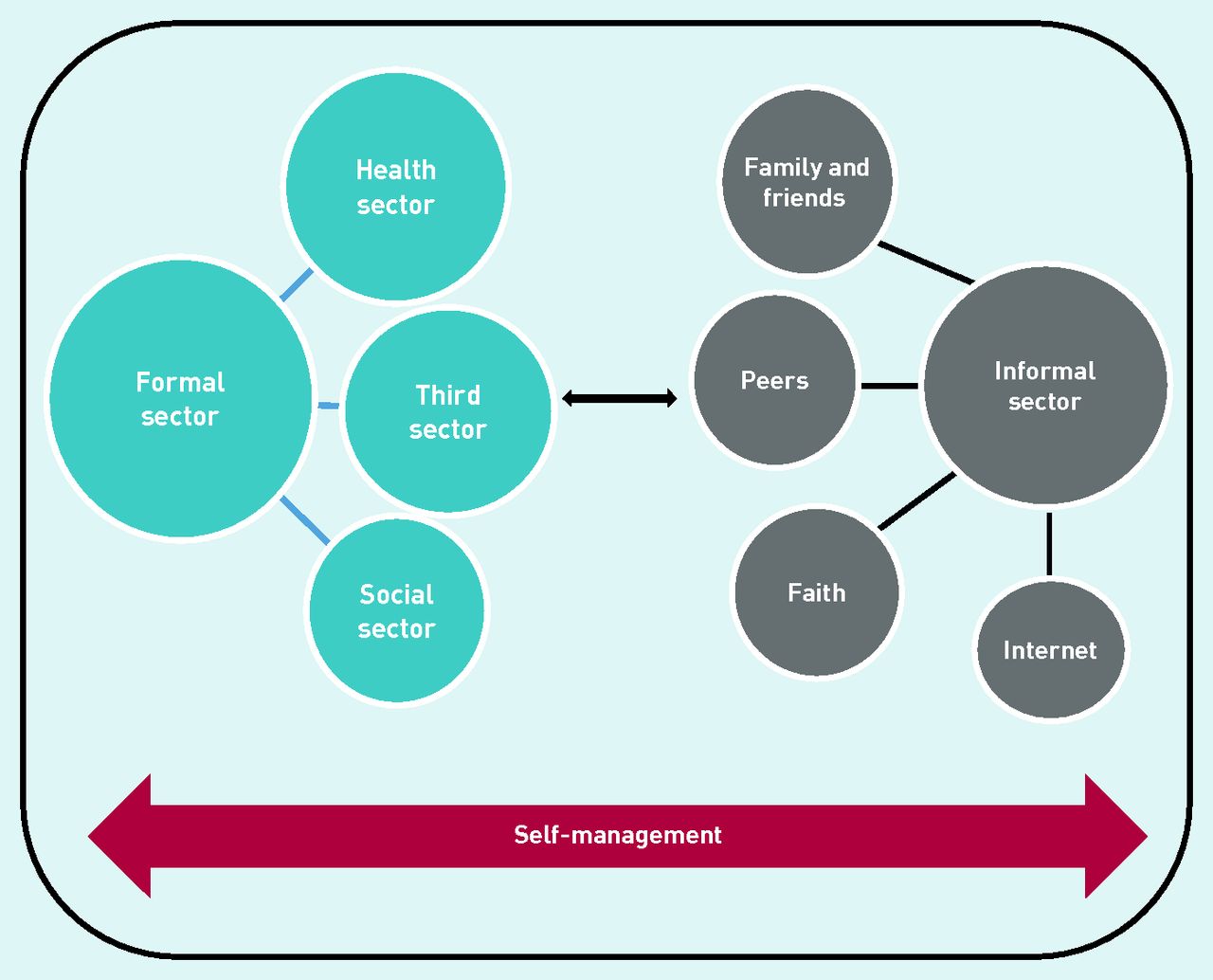
- Figure 3.
Support avenues for older adults with self-harm behaviour.


{kind=link}
{kind=link}
{kind=link}
Tables
How this fits in
Self-harm is the leading risk factor for suicide, with suicide being an increasing concern among older populations given the high suicide rates reported. Though research has shown that older adults who self-harm are in frequent contact with primary care owing to complex health conditions, to the authors’ knowledge, no research has explored the role of primary care in supporting this group. Using a qualitative approach, the presented study’s findings confirm that primary care is a potential avenue for effective self-harm management in older adults, and GPs are in a good position to manage and support older adults who self-harm. However, given the complex nature of self-harm, primary care may wish to work with other sectors (health, social, and third sectors) to comprehensively support older adults who self-harm, as recommended by the National Institute for Health and Care Excellence. Patient ID Sex Ethnicity Age, years Health conditionsa Psychosocial contexta Start of self-harm Supporta F1 F White British 62 Personality disorder
Fibromyalgia, diabetes, heart disease, scoliosis, arthritis
Early start of mental health difficulties with child sexual abuse
Living alone, experiencing loneliness
Family history of mental illness
Experienced loss of children in adulthood
Limited mobility due to health
Early teens Long history of overdose hospital admissions
Limited family support
No longer attending group for self-harm
Medication seen by GP
Infrequent contact with CPN
F2 F White British 72 Depression, alcohol misuse
Irritable bowel syndrome, arthritis, pancreatitis
Childhood sexual abuse and overall stressful upbringing
Interpersonal difficulties with family and family history of alcohol misuse
Early retirement due to mental health conditions
Early childhood Regularly attends sector group for self-harm
Previous contact with secondary care
Now overseen by GP
F3 F White British 60 Personality disorder
High blood pressure, hypothyroidism
Multiple childhood stressors including sexual abuse, bullying, neglect, encounters with judiciary system
Family history of mental illness
Partner bereavement leading to experience of loneliness
Early teens Regularly attends sector group for self-harm
Medication overseen by GP
Support received by CPN
Long history of contact with primary and secondary care services
M1 M White British 67 Depression
High blood pressure, heart disease
Early childhood experience of shame caused by secrecy of adoption
Experienced multiple losses of family members and friends
Health conditions disrupted life since early 40s leading to job loss
40s Multiple experiences with counsellors and contact with primary and secondary care
Regularly attends sector group for self-harm
Medication overseen by GP
F4 F White British 65 Personality disorder, eating disorder, post-traumatic stress disorder
Osteoporosis, high blood pressure
Early childhood experiences of sexual abuse, violence, and neglect
Family history of mental illness
40s Recently joined third-sector self-harm group
Support from primary and secondary care services
Receives family support
F5 F White British 62 Depression
Fibromyalgia, sciatica, ankylosing spondylosis, arthritis
Early childhood loss with death of mother, adopted by grandparents
Ongoing conflict with husband and interpersonal problems
Multiple bereavements
Health conditions affecting mobility and everyday life
60s Recently joined third-sector self-harm group
Previously received support from psychiatrist
Medication for depression overseen by GP
Receives family support
M2 M White British 61 Pica, anxiety, post-traumatic stress disorder
Dystonia, heart failure, diabetes, liver disease, ulcerative colitis
Limited mobility due to health conditions
Several negative experiences with healthcare facilities
Loss of family members
First time talking about self-harm
40s Previously supported by counsellors
Currently sees psychiatrist
Attends third-sector dystonia group
No support for self-harm
F6 F Ethnic minority British 62 Depression, eating disorder
Arthritis, walking disability
Ongoing experience of violence and abuse
Escaped violent and life-threatening marriage, forcing themto re-locate
Self-identified as ethnic minority, highlighting difficulty to access support
Early childhood Received limited support for self-harm
Attends third-sector self-harm group
Soon to start seeing a private counsellor
M3 M White American 60 Eating disorder, obsessive compulsive disorder, personality disorder
Anaemia
Divorce of parents experienced in childhood
Self-identified as homosexual, highlighting difficulty to access support
Highly educated and with previous experience in research
High levels of insight and self-awareness
Early childhood Talking therapy received for over a decade but stopped once moving to England
Attends service user group and is on the waiting list for a self-harm hospital programme
No family support
↵a As reported by participants. CPN = community psychiatric nurse. F = female. ID = identifier. M = male.
Participant ID Sex Age, years Rolea Personal background F7 F 46 Volunteer lead at self-harm charity Previous self-harm history
Started the only self-harm group in [city in North West England] because she saw the lack of support for people who self-harm
Has only recently started the group and supported people who self-harm
Looking for funding in order to make group a third-sector organisation for people who self-harm
F8 F 36 Support worker at self-harm third-sector group No mention of self-harm or mental health history
Has worked with vulnerable populations, such as providing support for abused females in the past
Majority of experience supporting people who self-harm through observation of previous groups’ support worker
F9 F 52 Support worker at self-harm third-sector group Previous self-harm history
Working as a support worker for many years but only recently with people who self-harm
Looking to receive further training for supporting people who self-harm
F10 F 49 Main facilitator at self-harm third-sector group Traumatic experience in teens (rape) that led to self-harm
Received support from family and local third-sector group for self-harm in the last decade
Took over support worker/facilitator role in the group 11 years ago, while still in recovery for self-harm
Has completely stopped self-harming for 8 years
Multiple experiences with research projects as well as being a lay board member for various local suicide prevention boards
F11 F 40 Support worker at older adults’ third-sector group No mention of self-harm or mental health history
Support offered to older adults focused on social services benefits and overall wellbeing
Has not received training on how to manage and deal with people who self-harm
Has trouble relating and understanding self-harm in members
M4 M 42 Support worker at older adults third-sector group Previous counselling/psychology background
Previous experience in research with older adults’ population and mental health
M5 M 50 Main facilitator at self-harm third-sector group Previous history of self-harm and suicidal attempts from early adolescence due to childhood sexual abuse
Only received support for their mental health when diagnosed with cancer in their adult years
Started facilitating group after volunteering at service user-led group
Participated in other research projects and actively involved in public speaking, and raising mental health and self-harm awareness
↵a As identified by participants. ID = identifier. F = female. M = male.
External factors Healthcare professionals’ attitudes and preconceptions
Structure of healthcare system
Disparity of care
Fragmented care delivery: mind–body dualism and priority to physical health care
Practical barriers Mobility restrictions
Transportation difficulties
Bureaucratic delays in healthcare delivery
Limited resources/staff
Internal factors Older adults’ attitudes and preconceptions of healthcare professionals
Reluctance to seek help
Health status of older adults
External factors Healthcare professionals’ attitudes and empathy
Staff with previous lived experience
Structural factors Accessible facilities
Provision of ongoing and regular support
Internal factors Previous positive treatment experiences influencing older adults’ attitudes towards staff
Health status of older adults
Be aware that self-harm can occur in older adults, and though suicidal intent is not always present, it is important to consider patients’ suicidality
Consider the stigma attached to self-harm, and ensure an empathic approach so that the patient feels listened to
Be responsive to the distress associated with self-harm; do not focus exclusively on the physical sequelaeof self-harm
Consider offering longer appointments to provide comprehensive assessment and support to the patient for physical and mental health needs
Consider arranging a follow-up as part of ongoing assessment and management
Review current medication to assess whether these may act potentially as a method of self-harm, for example, overdose
Assess patient safety throughout the consultation and advise on access to means of potential self-harm
Liaise with the third sector and social care sector, or refer to specialist care where indicated
View the consultation as an opportunity to provide self-harm management and avoid repeat self-harm and suicide
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

