


Abstract
Background Clinical judgement is intrinsic to diagnostic strategies in general practice; however, empirical evidence for its validity is sparse.
Aim To ascertain whether a GP’s global clinical judgement of future cognitive status has an added value for predicting a patient’s likelihood of experiencing dementia.
Design and setting Multicentre prospective cohort study among patients in German general practice that took place from January 2003 to October 2016.
Method Patients without baseline dementia were assessed with neuropsychological interviews over 12 years; 138 GPs rated the future cognitive decline of their participating patients. Associations of baseline predictors with follow-up incident dementia were analysed with mixed-effects logistic and Cox regression.
Results A total of 3201 patients were analysed over the study period (mean age = 79.6 years, 65.3% females, 6.7% incident dementia in 3 years, 22.1% incident dementia in 12 years). Descriptive analyses and comparison with other cohorts identified the participants as having frequent and long-lasting doctor–patient relationships and being well known to their GPs. The GP baseline rating of future cognitive decline had significant value for 3-year dementia prediction, independent of cognitive test scores and patient’s memory complaints (GP ratings of very mild (odds ratio [OR] 1.97, 95% confidence intervals [95% CI] = 1.28 to 3.04); mild (OR 3.00, 95% CI = 1.90 to 4.76); and moderate/severe decline (OR 5.66, 95% CI = 3.29 to 9.73)). GPs’ baseline judgements were significantly associated with patients’ 12-year dementia-free survival rates (Mantel–Cox log rank test P<0.001).
Conclusion In this sample of patients in familiar doctor–patient relationships, the GP’s clinical judgement holds additional value for predicting dementia, complementing test performance and patients’ self-reports. Existing and emerging primary care-based dementia risk models should consider the GP’s judgement as one predictor. Results underline the importance of the GP-patient relationship.
INTRODUCTION
Health policy and research have provided increased awareness about identifying individuals at risk of dementia in primary care.1 This is justified by strategies for risk reduction,2 and the opportunity for patient-centred management3 in case of cognitive deterioration, for example, home visits, adjusted communication, family involvement, checking medication, and alertness for risks such as social isolation. For older people with memory concerns, the GP is a significant contact.4 A patient’s predicted cognitive status can add to the GP’s holistic view of the patient and provide relevant information for ongoing patient management. Parameters discussed for identifying dementia risk include biomarkers,5 neuropsychological constructs such as mild cognitive impairment,6 short tests like the Mini-Mental State Examination (MMSE),7 and patient self-reports of subjective cognitive decline (SCD).8 Several dementia risk scores for use in general practice have been published recently,9–12 but none of these considers the GP’s judgement as an important source of prognostic power, therefore neglecting the expertise and relevance of GPs as experts on their patients. Ford et al suggested that easily available predictive information from primary care should also be explored in future studies because it ‘… might increase the predictive validity of a model’.13
Particularly in the absence of general screening activity,14 clinical judgement is an essential part of early diagnostic strategies used in primary care, arising from a hermeneutic approach to individual symptoms, changes, complaints, and patterns.15 Continuous and familiar doctor–patient relationships in primary care foster the integration of longitudinal clinical, biographical, and psychosocial information for clinical judgement.16 As Thornton emphasised, ‘… at the heart of evidence based medicine is good judgement’.17 In other medical settings, expert judgement (alone or combined with objective measures) has shown several advantages and good validity, for example, in the emergency department18 and in medical education.19 With regard to early dementia recognition and prediction, the GP’s judgement and the patient’s subjective cognitive decline are the most important parameters in the initial diagnostic trigger stage, whereas cognitive tests and laboratory parameters become relevant in the subsequent disease-oriented diagnostic stage.20 According to the stimulating and substantiating factors of intuitive clinical judgement,21 dementia prediction is a prime example of intuition as an appropriate initial diagnostic strategy in primary care.
| Several dementia risk scores have been constructed recently that do not include the GP’s expertise. This study found that a GP’s global clinical judgement of future cognitive status has an independent value for predicting a patient’s dementia, yielding additional information beyond test scores and patient reports. This finding supports the potential of intuitive and heuristic clinical judgement as a diagnostic strategy. |
How this fits in
The aim of this study was to address the research question: does the GP’s clinical judgement contribute additional information for the prediction of dementia within 3 years and time of dementia onset over 12 years, beyond the patient’s self-report and test performance?
METHOD
The German Study on Ageing, Cognition, and Dementia (AgeCoDe) is a multicentre prospective cohort study of German patients in primary care.22 Demographic, clinical, and neuropsychological data were collected from patients during home visits by interviewers at intervals of 18 months (at baseline and in eight follow-up assessments I to VIII). Interviewers were researchers, trained and supervised in the use of the assessment procedures. Independent from these patient interviews, GPs gave information about their participating patients. The analyses presented in this article consist of data from baseline and two follow-ups (with regard to dementia prediction over 3 years) and eight follow-ups (with regard to prediction of time to dementia onset over 12 years), respectively.
GPs were recruited by local researchers at six metropolitan study centres. Patients were recruited from the 138 participating GP practices between 1 January 2003 and 30 November 2004. Inclusion criteria for patients were age ≥75 years, absence of dementia in the GP’s view, and at least one contact with the GP within the previous 12 months. Exclusion criteria were consultations only by home visits, residence in a nursing home, severe illness the GP would deem fatal within 3 months, insufficient German language skills, deafness, blindness, lacking the ability to consent, and not being a regular patient of the participating GP practice. Researchers and GPs together compiled the lists of eligible patients from all practice patients; researchers then randomly chose up to 60 eligible patients per practice using random number tables.
Outcome variable: incident dementia
Interviewers conducted a SIDAM interview (structured interview for the diagnosis of dementia of the Alzheimer type, multi-infarct dementia, and dementias of other aetiology),23 including a neuropsychological test battery (the SIDAM-Score or SISCO), at baseline and all follow-ups. DSM-IV dementia criteria24 were included in a diagnostic algorithm in the SIDAM by assessing cognitive performance and activities of daily living, including an informant interview in cases with suspected dementia. Dementia status in patients without personal interview at follow-up (for example, because of refusal or death) was based on additional informant interviews with relatives, professional carers, and GPs, using the Global Deterioration Scale (GDS)25 and Blessed Dementia Scale.26 All diagnoses were discussed in consensus conferences with the interviewers and experienced geriatric psychiatrists or geriatricians. Dementia diagnoses could be verified by follow-up results.
Predictor variables
Education
The level of education received by the patients was assessed in at-home interviews and categorised as low (elementary education), intermediate (intermediate vocational/general qualification), or high (tertiary education) using an international educational classification.27
GPs’ clinical judgement
At baseline and without information about the results of the research interviews, GPs rated their patients’ future cognitive status using the seven-point ordinal GDS (1 = no subjective or objective impairment to 7 = severe dementia)25 and answering the question ‘Which GDS stage do you expect the patient will have in 3 years?’ This GP rating was analysed as a global clinical judgement of future cognitive status.
The MMSE (score 0–30)7 was used as a short test of the patient’s global cognition. A patient’s SCD8 was assessed with the questions: ‘Do you feel like your memory is becoming worse?’ (yes/no); in case of response ‘yes’: ‘Does this worry you?’ (yes/no).28
Characteristics of patients, doctor–patient relationship, and GPs’ decision making
Beside the SISCO, subtests of the CERAD-NP (neuropsychological assessment of the Consortium to Establish a Registry for Alzheimer’s Disease)29 were used to measure memory performance. All drugs a patient was currently taking were documented in the interviews. GPs gave information about patients’ comorbidities and were asked to describe their doctor–patient relationship in terms of familiarity with the patient (from 1 = very poor to 4 = very high) and years of doctor–patient contact.
To evaluate the relevance of cognitive tests in GPs’ diagnostic repertoire, all GPs in the follow-up phases III–VI reported on whether they conducted or requested any cognitive testing for each patient.
Statistical analysis
Predictor variables were checked for multicollinearity in terms of bivariate correlations and all coefficients were found to be negligible and well below 0.50 (see Supplementary Table 1 for details).
To evaluate the independent effects of predictors on the development of incident dementia within 3 years, multivariable mixed-effects logistic regression was applied, considering the cluster effect of GP practices. Odds ratios (OR) were calculated with 95% confidence intervals (CI).
Multivariable mixed-effects Cox regression (again including the cluster effect of GP practices) was used to analyse the independent effects of predictors on time of dementia onset over 12 years. Hazard ratios (HR) were calculated with 95% CI.
For all models, the Bayesian information criterion was chosen as a robust and conservative indicator of model fit, with lower values indicating better fit.
Differences in dementia-free survival times between participants with different GP-predicted GDS stages were illustrated by Kaplan–Meier survival curves and tested for significance using the log rank test.
Analyses were performed with SPSS (version 24) and SAS (version 9.3).
RESULTS
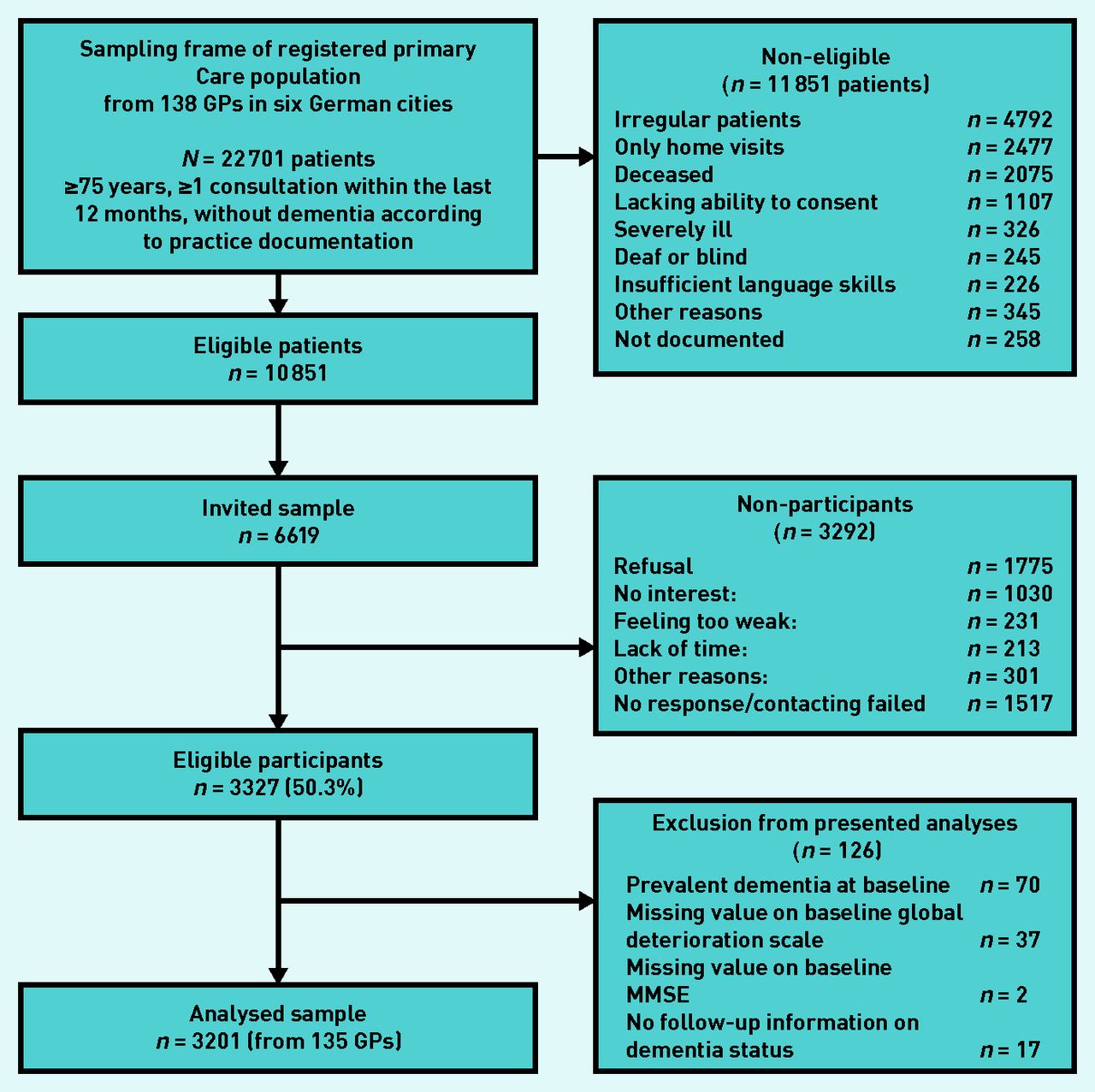
At baseline, 138 GPs (19–29 per study centre) recruited a total of 3327 participants (mean number = 24.1, SD = 11.7). Most of the recruiting GPs were male (74.5%), their mean age was 50.9 years (SD = 6.5), and the mean of their years in practice was 14.9 (SD = 6.7). Figure 1 gives details of the patient recruitment process. Consenting patients (n = 3327) were slightly younger (mean = 80.1 years [SD = 3.8] versus 80.7 years [SD = 3.8]) and more often male (34.5% versus 31.1%) than refusing or non-responding patients (n = 3292). The analysed sample for all regression models consists of n = 3201 participants with complete baseline information (face-to-face patient interview and GP questionnaire) and at least one valid item of follow-up information on dementia status (based on face-to-face or informant interviews), from 135 GPs (for three GPs no patient was eligible for the analysis).
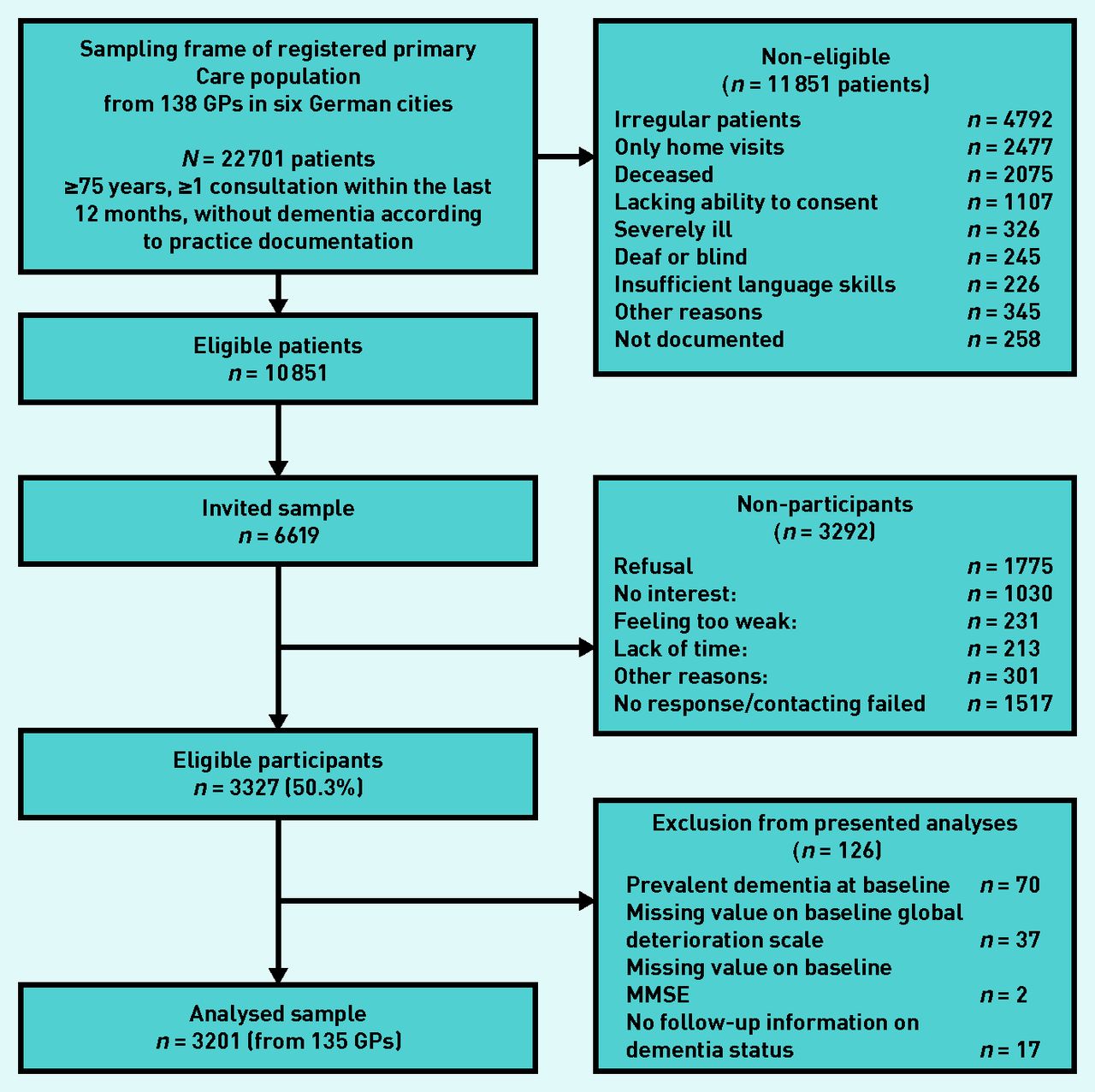
Patient recruitment flow chart.
MMSE = Mini-Mental State Examination.
The proportion of participants with personal versus informant follow-up interview is more than 80% versus <20% for each follow-up assessment, and personally interviewed patients slightly differ from non-interviewed patients (see Supplementary Tables 2 and 3 for details). The main reasons for missing personal follow-up interviews were death and refusal.
Characteristics of patients and doctor–patient relationships
Table 1 gives baseline characteristics for the participants. A high generalisability is supported by the low prevalence setting with realistic incidence rates of dementia. However, compared with other, younger cohorts,30 CERAD memory performance on verbal fluency and immediate word list recall in the AgeCoDe baseline sample was considerably better. GPs report excellent patient knowledge, and the mean consultation rate is higher than in representative German cohorts.31 The number of drugs taken and the proportion of patients taking five or more drugs is comparable, but slightly smaller than in an unselected German primary care sample of community-dwelling older adults.32 Except for the high rate of coronary heart disease, prevalence rates for chronic conditions in the AgeCoDe cohort very closely correspond to the rates described in representative German cohorts.33,34
Baseline characteristics of the patients in the study (n = 3201, all without dementia at baseline according to both reference standard and GP judgement)
Prediction of incident dementia within 3 years
In all models, the GP’s judgement yielded additional and significant information for the 3-year prediction of dementia, independent of the patient’s sex, age, education, SCD, and MMSE scores (Table 2).
Independent effects of baseline predictors for the 3-year prediction of dementia (multivariable mixed-effects logistic regression, n = 3201)
The regression model with GP/SCD/MMSE shows a better model fit than all other models based on the Bayesian information criterion (lowest BIC).
Prediction of time of dementia onset over 12 years
In all models, the GP’s judgement added specific information for the prediction of time to dementia onset in a 12-year period, independent of the patient’s sex, age, education, SCD, and MMSE scores (Table 3). The regression model with GP/SCD/MMSE outperformed all other models in terms of model fit based on the Bayesian information criterion (lowest BIC).
Independent effects of baseline predictors for the prediction of time of dementia onset over 12 years (multivariable mixed-effects Cox regression, n = 3201)
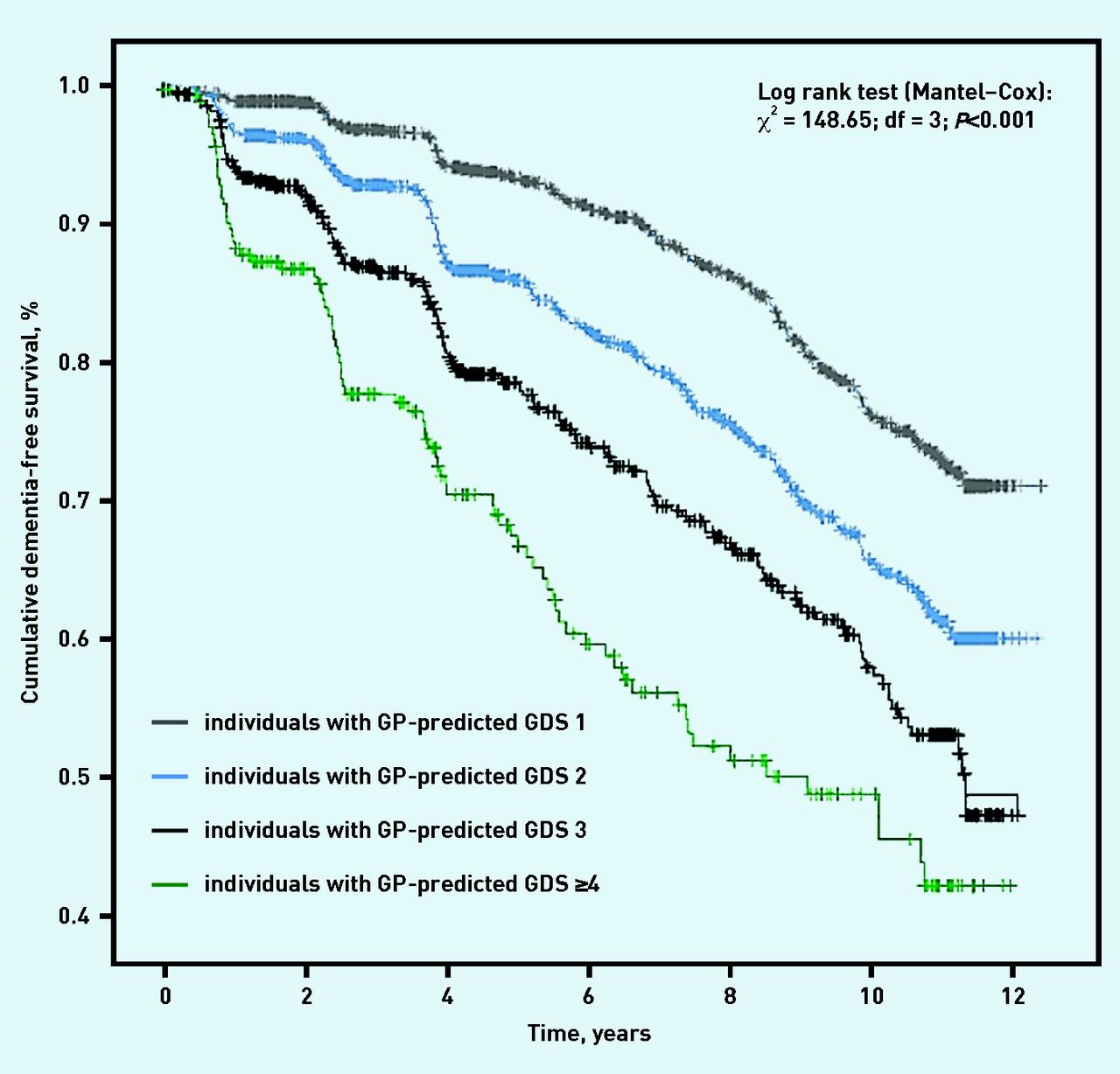
Multivariable mixed-effects Cox regression found that dementia-free survival significantly varied as a function of the GP’s rating of a patient’s future cognitive status (Figure 2).

{kind=link}
{kind=link}
Kaplan–Meier curves of dementia-free survival in patients with different GP ratings on future cognitive status (GDS stage). GDS = Global Deterioration Scale.
DISCUSSION
Summary
In the study sample of patients with a close doctor–patient relationship, the GP’s clinical judgement holds an added value for the prediction of dementia, apparently by providing information beyond cognitive test performance and patient’s self-report. This applies to both short-term prediction of incident dementia within 3 years and long-term prediction of dementia onset over 12 years. The results underline the importance of the GP–patient relationship.
Strengths and limitations
The presented analyses and conclusions are restricted to the applied parameters; there are many alternative measures of SCD, test performance, and clinical dementia rating.
The strong effect of the MMSE may be partly explained by a bias in terms of methodological proximity of predictor MMSE and gold standard. The MMSE, as the only one of the examined parameters, is an explicit part of the diagnostic SIDAM algorithm for the gold standard of clinical dementia diagnosis.
Compared with other cohorts, participants show better cognitive and verbal abilities (CERAD) and a closer doctor–patient relationship in terms of GP familiarity, duration of doctor–patient contact, and number of consultations. These biases may be the result of the study’s inclusion and exclusion criteria, as well as GPs’ involvement in the initial patient recruitment process. The effect of the GP’s judgement may have benefited from this biased selection of participants with a more involved kind of doctor–patient contact. In other aspects, such as somatic comorbidities, drug intake, and dementia incidence, the analysed sample seems not to be biased.
The independent association of the GP’s judgement was analysed and model fit indices of several prediction models were compared. These analyses can be interpreted as an indication of content validity, that is, the fundamental insight that a GP’s judgement on patient cognition is independently associated with dementia risk. For analyses of predictive validity, studies following STARDdem criteria35 are needed, incorporating the GP’s judgement and other predictors for generating practically relevant parameters such as positive and negative predictive values.
The main strength of the presented study is its prospective design. Especially in cross-sectional diagnostic studies on cognitive impairment, the risk of incorporation bias is high.35 A prospective design implies decoupling the reference standard from the index tests, thus reducing the risk of incorporation bias as well as diagnostic review bias. With regard to epidemiological studies, an elaborate diagnostic reference standard was used, mainly (the interview) being applied to most participants and thus minimising verification bias. The validity of the reference standard was further facilitated by re-evaluating a dementia diagnosis in follow-up visits (in cases with personal interviews), thereby reducing the risk of misclassification. However, dementia status in non-participants was derived from informant interviews, also including information from the GP. Apart from the validity aspects of informant reports, this could have introduced a bias to the benefit of the GP’s judgement.
Another advantage of the study is a valid GP judgement in terms of explicit questions about cognitive status; the study did not rely on GPs’ documentation of cognitive status in medical records.
Comparison with existing literature
To the authors’ knowledge, this is the first analysis of the validity of GPs’ clinical judgement regarding a patient’s likelihood of future dementia. Two previous studies report relevant validity of an expert clinical rating for future dementia,36,37 but ratings were based on singular lengthy interviews (90–120 minutes) by ‘dementia experts’ and not GPs. Primary care decision making with its specific diagnostic concepts, strategies, and holistic perspective has been described in theory as carrying diagnostic and prognostic potential.15,16 However, empirical evidence is sparse. The results of the current study underline the value of clinical judgement as a central parameter in the trigger stage: asking and testing patients is in contrast to what GPs normally do in the initial diagnostic phase.38 As a first step, they usually evaluate complex constructs, such as the risk of dementia, in a more intuitive way, based on a close, trusting, and continuous doctor–patient relationship.
Throughout the literature, there exists a strong belief in the superiority of questionnaires and performance-based tests over global, intuitive clinical judgement. As generalist concepts may be distinct from specialist classifications (reported not only for dementia,39 but also for depression40 and headache),41 there is some questionable justification for assuming superiority of one over the other. Innovative study designs42 and elaborate methods are needed to compare different approaches in a valid manner, to reveal the diagnostic yield of GPs’ clinical judgement, and to disentangle the cognitive mechanisms behind it.
Implications for research
The presented analyses provide a first indication for the value of the GP’s judgement and may stimulate rigorous studies on GPs’ dementia recognition and prediction. From the results of this study and the subsequent discussion, it seems justified to consider the GP’s judgement in prediction models as one parameter for the identification of individuals at risk of dementia, at least in familiar doctor–patient relationships.
As one of the central parameters in the diagnostic trigger stage, the GP’s judgement should be further investigated beyond dementia. Addressing attitudinal and cognitive biases of the GP’s judgement43 may help to improve its validity.
Acknowledgments
The authors thank all participants and GPs for their collaboration.
Notes
Funding
This study is part of the German Research Network on Dementia (KND), the German Research Network on Degenerative Dementia (KNDD), and the Health Service Research Initiative, and was funded by the German Federal Ministry of Education and Research (grant numbers: grants KND: 01GI0102, 01GI0420, 01GI0422, 01GI0423, 01GI0429, 01GI0431, 01GI0433, 01GI0434; grants KNDD: 01GI0710, 01GI0711, 01GI0712, 01GI0713, 01GI0714, 01GI0715, 01GI0716; grants Health Service Research Initiative: 01GY1322A, 01GY1322B, 01GY1322C, 01GY1322D, 01GY1322E, 01GY1322F, 01GY1322G). The funder had no influence on study design, collection, analysis, and interpretation of data, or the writing of the article and the decision to submit it for publication. Researchers are independent from funders.
Ethical approval
Approval was obtained from each study centre: Ethics Commission of the Medical Association Hamburg (OB/08 /022817/2007); Ethics Commission of the University of Bonn (050/02 258/07); Medical Ethics Commission II, University of Heidelberg at the University Medical Center of Mannheim (0226.4/2002 2007-253E-MA); Ethics Commission at the Medical Center of the University of Leipzig (143/2002 309/2007); Ethics Commission of the Medical Faculty of the Heinrich Heine University Düsseldorf (2079/2002 2999/2008); and Ethics Committee of the TUM School of Medicine, Munich (713/02 713/02 E).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Contributors
Further co-authors involved in the study were Jürgen in der Schmitten, Dagmar Weeg, Silke Mamone, Tobias Luck, Jochen Werle, Dagmar Lühmann, Christian Brettschneider, and Luca Kleineidam. Members of the AgeCoDe Study Group: Wolfgang Maier and Martin Scherer (principal investigators), Hendrik van den Bussche (principal investigator 2002–2011), Heinz-Harald Abholz, Christian Brettschneider, Cadja Bachmann, Horst Bickel, Wolfgang Blank, Hendrik van den Bussche, Sandra Eifflaender-Gorfer, Marion Eisele, Annette Ernst, Angela Fuchs, Kathrin Heser, Frank Jessen, Hanna Kaduszkiewicz, Teresa Kaufeler, Mirjam Köhler, Hans-Helmut König, Alexander Koppara, Carolin Lange, Diana Lubisch, Tobias Luck, Dagmar Lühmann, Melanie Luppa, Manfred Mayer, Edelgard Mösch, Michael Pentzek, Tina Posselt, Jana Prokein, Steffi Riedel-Heller, Susanne Röhr, Anna Schumacher, Janine Stein, Susanne Steinmann, Franziska Tebarth, Michael Wagner, Klaus Weckbecker, Dagmar Weeg, Jochen Werle, Siegfried Weyerer, Birgitt Wiese, Steffen Wolfsgruber, and Thomas Zimmermann.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received February 2, 2019.
- Revision requested March 11, 2019.
- Accepted May 8, 2019.
- © British Journal of General Practice 2019
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

