


INTRODUCTION
The potential benefit of any quality improvement scheme can be increased manifold if it is consistently and systematically applied across organisations and systems. However, this is not easily achieved. Across the UK, a third of healthcare improvement projects never spread beyond their particular unit, a further third are embedded within their own unit and spread across an organisation, and only a third are spread across their own and other similar organisations.1,2
The Institute of Healthcare Improvement (IHI) has branded the ‘Seven Spreadly Sins’ as common slip-ups that organisations make that prevent the successful spread of quality.3
In 2016, Barking and Dagenham, Havering, and Redbridge Care Commissioning Groups (BHR CCGs) embarked upon a programme to improve the quality of care provided to diabetes patients. The three CCGs are challenged by escalating diabetes prevalence, poor uptake of the National Institute for Health and Care Excellence’s (NICE) recommended eight care processes,4 and an increasing rate of complications. Encouraged by the rapid improvement of quality in one area,5 we sought to apply a similar approach, at scale, across the three CCGs. Our objectives were to control the growing prevalence of diabetes (establish a pre-diabetes register) and improve the quality of care to our patients (close the prevalence gap, increase the uptake of NICE-recommended care processes, and treat more people to target for blood pressure, cholesterol, and glycaemic control).
Although BHR CCGs had some common workstreams, we had mostly worked as independent organisations until recent times. Therefore, a quality improvement (QI) project of this scale (122 practices, 52 325 diabetes patients) was a daunting prospect. Here’s how we tackled the challenge successfully by avoiding the ‘Seven Spreadly Sins’:
SIN #1: DO NOT BOTHER TESTING — JUST DO A LARGE PILOT
True to the principles of QI, we did not always constrain ourselves with predetermined targets. For instance, we were not sure how to set the target for our pre-diabetes register. We waited for patterns to emerge, and we allowed these to guide our expectations.
SIN #2: GIVE ONE PERSON THE RESPONSIBILITY TO DO IT ALL
We devolved the leadership and generated a team spirit. Clinical leads and CCGs developed the overarching plan; clinical facilitators engaged with the frontline clinicians; local networks reviewed the results and shared learning; and practice managers and lead GPs championed and adjusted work plans as needed.
SIN #3: EXPECT HEROICS TO OVERCOME POOR PROCESSES
We worked on improving clinical and administrative procedures at practice level. Our urine albumin to creatinine ratio (ACR), smoking, and BMI record was particularly low; therefore, we trained our healthcare assistants and nurses to ensure that the patients are counselled about the importance of urine tests, and encourage patients to provide the urine sample together with all of the blood tests. We ensured that smoking status and BMI was correctly coded.
SIN #4: EXPECT HUGE IMPROVEMENTS QUICKLY
Instead, we set achievable targets based on the current baselines, for example, 2% increase from baseline on the three treatment targets.
SIN #5: SPREAD THE SUCCESS UNCHANGED
There was no prescribed blueprint for implementation. Engagement with the QI process helped practices to innovate and evolve the project to best suit their needs. For example, some practices chose to link diabetes checks with flu jabs, whereas others developed dedicated diabetes teams responsible for call–recall and clinical management of the blood results.
SIN #6: CHECK HUGE MOUNTAINS OF DATA JUST ONCE EVERY QUARTER
Instead, practices were able to access and update their data as frequently as needed. Data were provided in practical formats, for example, a spreadsheet to illustrate which of the care processes were missing for individual patients.
SIN #7: RELY ON VIGILANCE AND HARD WORK
We were not only vigilant and worked hard, but we also realised that we needed to work differently. We commissioned partners for QI who helped us recruit and train local clinicians to become QI leads for networks of practices. Their training and local knowledge placed them in a unique position to offer hands-on support to the practices.
RESULTS
All 122 BHR practices participated in the QI project. We identified 30 490 patients with pre-diabetes and referred them to local and national prevention pathways. Because of increased screening our expected versus actual prevalence gap reduced from 18 925 to 10 460 patients. The uptake of eight care processes improved significantly from 26.4% to 66.7%. In total, 22 967 more patients are now receiving all eight care processes as compared with 2015–2016 baselines (Figure 1). The increase in the uptake of urine ACR was particularly significant (from 37.9% to 72.6%, or 21 330 additional patients).

Improvement in eight care process uptake. 8CP = eight care processes.
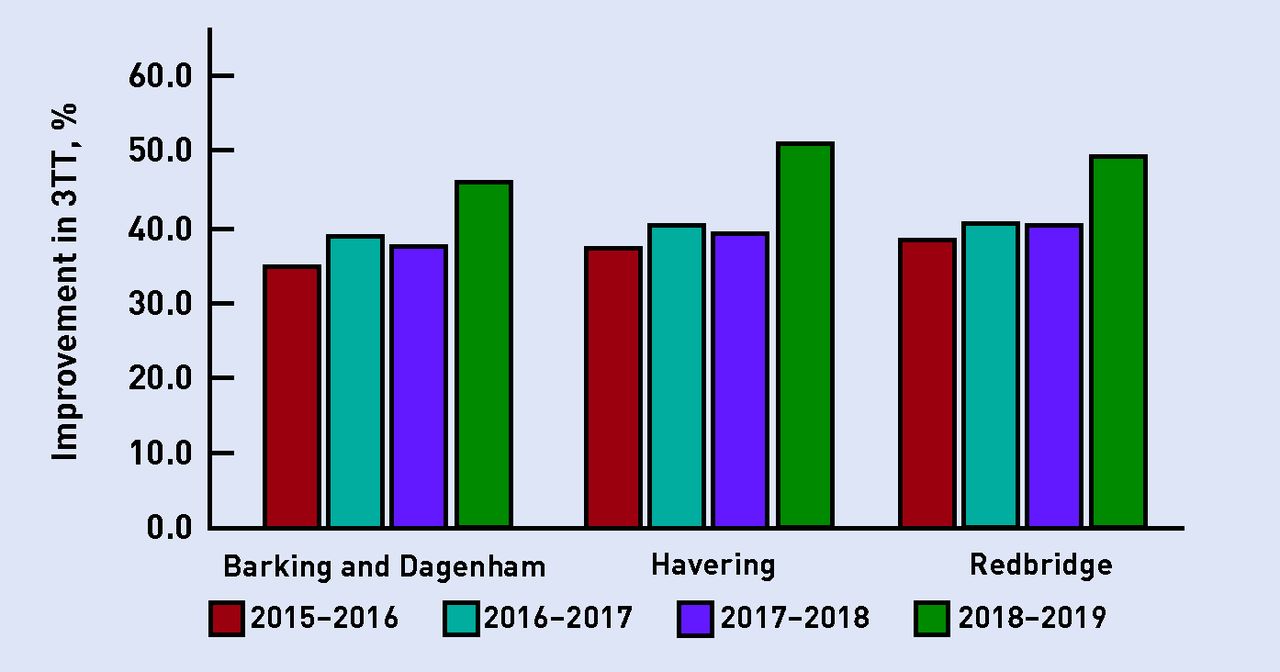
Patients achieving an HbA1c of 58 increased from 51.9% to 60.4% (10 055 additional patients). Patients achieving control for all three treatments (Hba1c, cholesterol, and blood pressure) increased from 36.9% to 48.6% (9834 patients) (Figure 2).
{kind=link}
{kind=link}
Improvement in treating to target. 3TT = three treatment targets.
The improvements in patient care are even more noteworthy, as the number of patients with diabetes increased from 37 755 to 49 040 between 2016 and 2019.
CONCLUSION
As the working at scale movement is gathering momentum in primary care, the time is ripe to identify and consolidate strategies that will deliver quality at scale. Our work illustrates that widespread improvement in quality is possible and within reach for most NHS organisations — as long as we remember to avoid the pitfalls.
Acknowledgments
The authors wish to thank BHR practices, the Clinical Effectiveness Group, and UCL Partners.
Notes
Provenance
Freely submitted; externally peer reviewed.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received June 24, 2019.
- Revision requested July 16, 2019.
- Accepted August 20, 2019.
- © British Journal of General Practice 2020
In this issue









Jump to section
- Top
- Article
- INTRODUCTION
- SIN #1: DO NOT BOTHER TESTING — JUST DO A LARGE PILOT
- SIN #2: GIVE ONE PERSON THE RESPONSIBILITY TO DO IT ALL
- SIN #3: EXPECT HEROICS TO OVERCOME POOR PROCESSES
- SIN #4: EXPECT HUGE IMPROVEMENTS QUICKLY
- SIN #5: SPREAD THE SUCCESS UNCHANGED
- SIN #6: CHECK HUGE MOUNTAINS OF DATA JUST ONCE EVERY QUARTER
- SIN #7: RELY ON VIGILANCE AND HARD WORK
- RESULTS
- CONCLUSION
- Acknowledgments
- Notes
- REFERENCES
- Figures & Data
- Info
- eLetters
More in this TOC Section
Related Articles
Cited By...

