


INTRODUCTION
Mental health difficulties are the norm in diabetes not the exception.1 They span from dementia and depression to anxiety and addictions, and of course diabetes distress and diabulimia. All mental illnesses can negatively affect a person’s ability to self-manage and self-management is the central tenet of diabetes care.
It is not surprising then, to learn that addressing mental health difficulties not only improves mental health outcomes but diabetes outcomes too.2
We need to embed and integrate mental health care into the entire diabetes care pathway. But in diabetes commissioning, mental health is usually an afterthought and often seen as a ‘nice to have’ part of the pathway rather than an integral component. Can we really afford to leave it there?
FROM THE HORSE’S MOUTH
The Too Often Missing report1 is an extensive survey of people with diabetes (PWD), GPs, and other professionals about mental health and wellbeing in diabetes. It found that 70% of PWD feel overwhelmed by the demands of their condition. Of these, three-quarters said that their self-management was affected by their emotional struggle and three-quarters felt that they could not access the specialist mental health support they needed.
The report also found that healthcare professionals often lack confidence in raising the issue of mental health and wellbeing with PWD and so they avoid it.1 In particular, they struggle to support people who are not engaged with their management plan (often referred to as ‘non-adherent’ or ‘non-compliant’) and they are concerned about the lack of diabetes specific mental health services for onward referral.
HOW THESE FINDINGS TRANSLATE TO THE FRONT LINE
The North West (NW) London map of mental health services for PWD showed that there were only 15 mental health professionals working in diabetes across the whole sector. This is a sector covering eight clinical commissioning groups (CCGs) and a diabetes population of >140 000 people (unpublished data; further information from authors on request). NW London is not unusual in this mismatch of available resources.
Extrapolating from prevalence estimates, in NW London, that would be 15 mental health professionals to support 50 000 people with diabetes distress (36% prevalence)3 or 98 000 people struggling to self-care because of feeling overwhelmed by diabetes (using the 70% prevalence described above).1 Put another way, 98 000 PWD is more people than you can fit into Wembley Stadium, being cared for by one football team and their substitutes.
It is understandable then, that primary care and diabetes professionals might be concerned that they will be left ‘holding the baby’ if they ask questions related to mental health.
IMPROVING ACCESS TO PSYCHOLOGICAL THERAPIES SERVICES: GREAT BUT NOT THE PANACEA
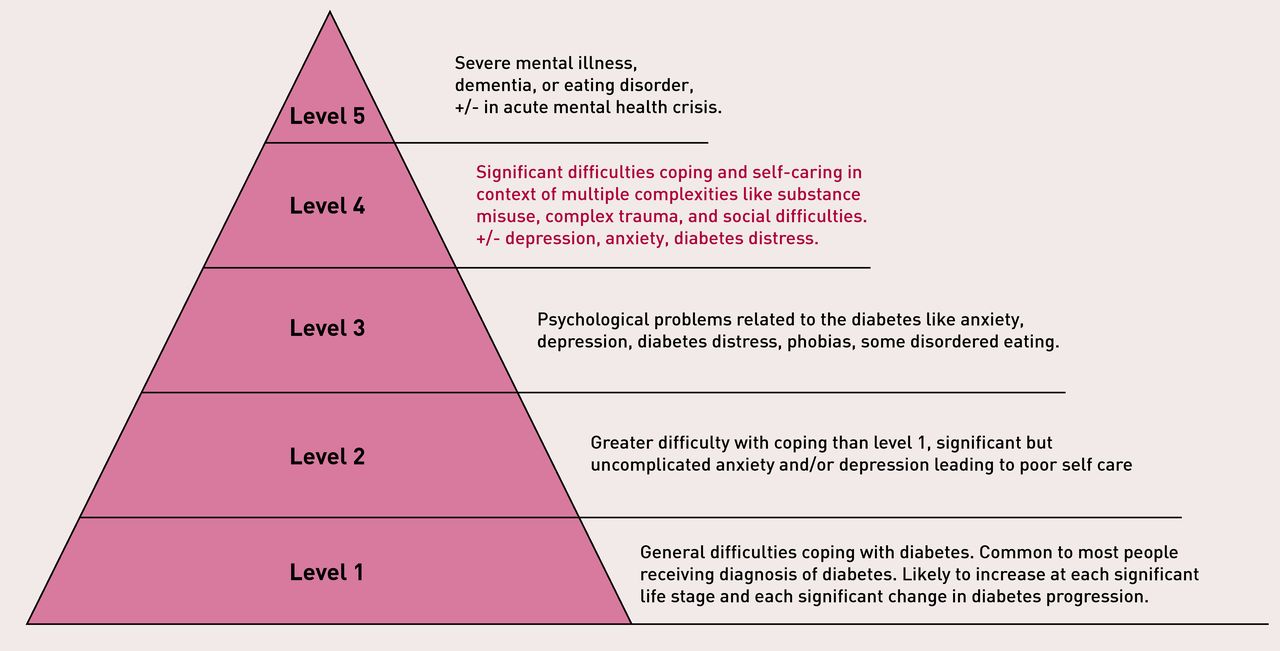
Improving Access to Psychological Therapies (IAPT) services were developed in 2008 and were always targeted at people with fairly uncomplicated depression and anxiety. This is what they are commissioned and trained to do at a national level. From 2016–2017, this has been extended to people with long-term conditions. Many of the services are trained to work specifically with diabetes but still mainly for uncomplicated depression and anxiety (Level 2 in the adapted pyramid of psychological need in people with diabetes;4,5 as described in Figure 1 and Box 1). They are very good at this,2 yet there is dissatisfaction with IAPT in some areas. Why? Because IAPT cannot address the entire pyramid of mental health need (Figure 1) that PWD can experience.

{kind=link}
| The pyramid of psychological need in people with diabetes was originally developed in the 2008 Diabetes UK document, Minding the Gap.4 It described three levels of need depending on the severity of symptoms and the kind of treatment options suitable for them. This was further developed in the 2010 Diabetes UK document,5 which described five levels of need and care, again with increasing severity of symptoms and complexity of treatment. Both distinguish between whether the issues need medication or not. We propose an adaptation of the five-level pyramid to highlight a difference at level 4. It isn’t just based on diagnosis and whether medication should be used but on complexity that includes a number of social as well as health factors. This level is important to highlight because it is underserved in current pathways. |
Pyramid of psychological need in people with diabetes: evolution of the model
In NW London, a stakeholder analysis revealed that the people whom primary care services most struggle to support are the ones that are most likely to be erroneously referred to IAPT, such as the 20-year-old male with type 1 diabetes, disengaged from services, or the single mother with type 2 diabetes and alcohol misuse. The list goes on.
Sadly, when there is no other mental health provision, primary care is left with no choice but to refer to IAPT. In turn, IAPT has no choice but to reject the referral because of their commissioning criteria. The entire system is inadvertently set up to fail everyone: the PWD, the referrer, and the IAPT service.
THE GAP IN THE MENTAL HEALTH PATHWAY: THE ELEPHANT IN THE ROOM
So what about the PWD who do not have straightforward depression or anxiety? If there is a crisis, suicide risk, or psychotic breakdown, a referral to secondary mental health services is suitable. This is Level 5 in the adapted pyramid of need.
If the person is under the care of the acute trust they may be lucky enough to have access to a clinical health psychologist if their mental health issue is related to their diabetes. This is Level 3 in the adapted pyramid of need, but primary care isn’t usually able to refer to them.
That leaves the people who have complex needs and/or are under community or primary care for their diabetes but are not mentally ill enough for secondary mental health services. They may be struggling with multiple, complex social stressors or a history of trauma. They are a small but significant cohort and have a bigger impact on services than their mere numbers would suggest. This is Level 4 in the adapted pyramid of need.
COMMON COMPLEX MENTAL HEALTH DISORDERS
The science of adverse childhood experiences (ACEs) has been growing for 20 years. It describes a dose-response curve between the number of ACEs a child was exposed to before the age of 18 (abuse, neglect, household mental illness, violence, or incarceration) and the number of mental and physical health conditions and health harming behaviours they develop in adult life, including an increased risk of developing diabetes.6
Traditionally, there hasn’t been much to offer this cohort of people. Repeatedly telling them to improve their diet or exercise and describing the severe complications of poorly controlled diabetes isn’t working. Referring them for the traditional IAPT approach isn’t working, as the referral is likely to be rejected because of complexity, as already described. So, what does work?
The NW London Integrated Care Programme set up a service that worked with this cohort, using a relational model of psychotherapy as well as psychiatry. It achieved average HbA1c improvements of 22 mmol/mol in 12 months. It paid for 70% of its costs within the first year and with adjustments to the model of care it became cheaper over the coming 3 years.
There are pockets of services like this dotted around the UK, but maintaining funding is challenging due to the cohort of people being relatively small.1
FINAL WORD
Improving Access to Psychological Therapies is not going to solve all mental health problems in diabetes care. It is not a panacea and it can only do its job well if the rest of the pathway works too.
Commissioners (for diabetes and for mental health) must decide if the service gap at Level 4 in the adapted pyramid of need is significant enough because of the complexity, multimorbidity, and wide ranging impact on the total health and social care economy, to warrant funding in a sustained way.
The same model works across all long-term conditions and this one investment could ‘kill several birds’, so to speak, making much more economic sense. Surely it is time to act.
Notes
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
- ©The Authors
This article is Open Access: CC BY-NC 4.0 licence (http://creativecommons.org/licences/by-nc/4.0/).
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

