


Abstract
Background Current funding arrangements for undergraduate medical student placements in general practice are widely regarded as outdated, inequitable, and in need of urgent review.
Aim To undertake a detailed costing exercise to inform the setting of a national English tariff for undergraduate medical student placements in general practice.
Design and setting A cost-collection survey in teaching practices across all regions of England between January 2017 and February 2017.
Method A cost-collection template was sent to 50 selected teaching practices across all 25 medical schools in England following the development of a cost-collection tool and an initial pilot study. Detailed guidance on completion was provided for practices. Data were analysed by the Department of Health and Social Care.
Results A total of 49 practices submitted data. The mean cost per half-day student placement in general practice was 111 GBP, 95% confidence interval = 100 to 121 (146 USD), with small differences between students in different years of study. Based on 10 sessions per student per week this equated to around 1100 GBP (1460 USD) per student placement week.
Conclusion The costs of undergraduate placements in general practice are considerably greater than funding available at time of writing, and broadly comparable with secondary care funding in the same period. The actual cost of placing a medical student full time in general practice for a 37-week academic year is 40 700 GBP (53 640 USD) compared with the average payment rate of only 22 000 GBP (28 990 USD) per year at the time this study was undertaken.
INTRODUCTION
The funding of medical student placements in general practice in England is currently agreed locally between Health Education England (HEE) and individual medical schools. HEE is the body with responsibility for managing undergraduate (pre-registration) education and postgraduate (post-registration) training for all health professionals in England. Undergraduate medical education funding is based on a historical NHS payment system originally known as SIFT (Service Increment for Teaching).1 This system is widely regarded as outdated, inequitable, and in need of urgent review.2,3.
SIFT was first introduced in 1976 in order to cover the additional service costs incurred by the NHS in providing facilities for the clinical teaching of medical students.1 Initially, SIFT was paid only to teaching hospitals and was not available to the small number of GPs who at that time taught medical students. The Winyard Report published in 1995 made SIFT available to general practices for the first time, initially at 12.00 GBP (14.80 USD) per half-day session.4–6 No further national guidance on funding of GP teaching has been issued since Winyard. The 2012 consultation report, Liberating the NHS: Developing the Healthcare Workforce, from Design to Delivery, set out the government’s commitment to a new system based on ‘tariffs’ for education and training as the foundation of a transparent funding regime that provides genuine incentives within the health sector.7
In 2013, following an impact assessment8 and a detailed cost collection in secondary care, HEE introduced the new tariff-based system for education and training. SIFT was replaced by a national tariff paid to teaching hospitals in proportion to the number of students taught each year. The undergraduate tariff was initially set at 34 623 GBP (approximately 45 600 USD) per full-time student per year, adjusted for each hospital by the NHS Market Forces Factor (MFF). The MFF is an estimate of unavoidable cost differences between healthcare providers based on their location, which can increase the total tariff by as much as 25%.9
The 2013 HEE costing exercise did not include teaching in general practice, and the tariff system subsequently introduced does not apply to primary care. Student placements in general practice in England therefore continue to be funded based on historical SIFT and variable local arrangements, at a rate on average of two-thirds of the new secondary care tariff.9 Recognising the need to address this disparity, a reference group was set up in 2013 by the Department of Health and Social Care (DHSC) to take forward the development of primary care tariffs. The Primary Care Education Working Group (PCEWG) included representatives from HEE, the Society for Academic Primary Care (SAPC), the Royal College of General Practitioners (RCGP), the Medical Schools Council (MSC), the British Medical Association (BMA), and the Committee of General Practice Education Directors (COGPED).
| A standard national tariff for the funding of medical student placements in secondary care was introduced in England in April 2013 based on detailed costing data from teaching hospitals. In spite of original intentions there is currently no national tariff for undergraduate student placements in primary care, nor any data on the real costs of teaching in general practice. Currently, payments to teaching practices are locally agreed, vary widely, and are consistently lower than those made to secondary care placement providers. For the first time, this study provides evidence that the real cost of teaching undergraduate medical students in general practice is similar to that in secondary care and will inform a realistic and fair primary care education tariff. |
How this fits in
There has been one previous attempt to estimate the cost of teaching in general practice that was based on an audit of overall placement spend by 15 medical schools, but did not examine actual costs at individual-practice level.10 The aim of the present study, commissioned by the PCEWG, was to develop a practice-level costing methodology and to undertake a national costing exercise in order to establish the real cost of teaching undergraduate medical students in general practice. It is intended that the results should inform the development of a new tariff for undergraduate primary care education in England.
METHOD
Data collection and sampling
A detailed cost-collection survey tool was developed in Microsoft Excel by DHSC statisticians following consultation with a range of stakeholders and extensive discussion at the PCEWG. Questions focused on the following components of practice-borne costs:
tutorials — the cost of teaching when no patient care is being provided;
observation — the productivity loss caused by teaching while patient care is being provided, calculated from the difference in the number of consultations offered while teaching and not teaching students;
administration — the costs of managing teaching in the practice; and
other — overheads and staff training.
Practices also provided data on practice list size, staff complement, teaching experience, and the responders’ confidence in their data. Costs were itemised on a per-half-day-session basis and number of students taught. To understand whether any variation in costs between practices may relate to the amount of teaching, the authors compared costs by the number of sessions delivered.
The tool was piloted in three teaching practices and revised in the light of feedback. Based on the pilot exercise it was estimated that one clinician and one manager would need a full day of protected time to collect the relevant data and complete the submission template. Heads of GP teaching at all 25 English medical schools were asked to identify two local teaching practices that met an agreed set of inclusion criteria, described below, and to support their local practices undertaking data collection by paying them 500 GBP on receipt of a completed template. All 25 schools agreed to this arrangement.
Practice inclusion criteria
A pragmatic approach was taken to recruiting practices, focusing particularly on those who demonstrated historical engagement and commitment to local undergraduate teaching programmes. The sample size of 50 practices was based on recruitment of two practices by every English medical school. This provided a good geographical spread (all English regions), a range of settings (rural, urban, inner city), and ensured practices taking part had experience of actively teaching undergraduates within the previous 2 years.
The template and a detailed guide to completion (available from the authors on request) were circulated to all medical school GP teaching leads at the beginning of January 2017, with a deadline for completion of the end of February 2017.
Data checking and analysis
The Workforce Information and Analysis team at the DHSC reviewed the cost metrics, total activity, and activity distribution to ‘sense-check’ each return. If anomalies were found, they were referred to the practice for further explanation. Results have not been harmonised using the MFF. MFF is an estimate of the unavoidable cost differences between different providers in different parts of the country. For example, providers in London and the South East of England might have higher costs of labour and land when compared with those in the North East of England. The MFF is used to ensure fairness in allocations and tariff. The analysis was descriptive with the cost per student session as primary unit of analysis to differentiate between single student placements and placements of a group of students simultaneously. The authors calculated means for each year of study and across all study years; and 95% confidence intervals (CI) weighted for the number of sessions each practice provided.
All data that were returned have been included in the analysis. Although the authors acknowledge that there are outlier values in the data, they have confidence in the overall quality of the data returned: the summary values were broadly in line with their expectations and practices were receptive to feedback from the study team.
RESULTS
A total of 49 practices, including at least one from each of the 25 medical schools in England, submitted data. Three schools made a single return but two completed three returns. Thus the authors obtained data from 49 practices against their target of 50, 98% of the intended sample size.
Practices
Practice list size ranged from 2750 to 45 000 (median 10 292 [standard deviation (SD) = 7.259]). This compares with the 2018 average UK general practice list size of 8279.11 A total of 39 (80%) practices were ‘confident’ or ‘very confident’ about the accuracy of their cost estimates (data and further details available from authors on request).
Summary statistics
In total, 11 061 sessions of placement activity were reported in the data collection, representing a total cost to these practices of 2.18 million GBP. Years 3–6 of study accounted for 88% of the teaching reported, and 80% of the overall cost of teaching. The number of students per session varied between 1 (all years of study) and 26 (years 1 and 2 of study). Groups tended to be larger in the study years 1 and 2, and smaller in years 3–6 of study (Table 1). More sessions were provided in the clinical years with year 5 having more than double the amount of sessions than other years. The mean number of sessions delivered by each practice was also higher in the later years. In year 1 the mean number of sessions delivered was 19.4 increasing to 76.3 and 73.4 for years 3 and 4, respectively, and 150.3 in year 5 (Table 2).
Practices, sessions, and cost per student teaching session at practice level
Average number of sessions split by practice and year
The costing template did not collect data at individual-student level, although anecdotal evidence suggests that the mean number of sessions in a practice will increase through the course of a student’s time in medical school. A year 1 or 2 placement may involve a short period as part of a relatively large group whereas a year 4 or 5 placement may involve a more intensive period within the practice.
Cost per session of student teaching
Table 1 shows the total activity and costs submitted split by the year of study. Median costs range from 89 GBP (interquartile per session in year 1 of study to 104 GBP for years 2 (interquartile range [IQR] 7–274) and 4 of study (IQR 3–331). The mean cost per student placement per session was 111 GBP (95% CI = 100 to 121), or, for a 10-session week, 1110 GBP.
The cost per session at practice level ranged from 39.60 GBP to 250.40 GBP with a median of 90.80 GBP (Figure 1). The authors did not find any evidence that larger practices had lower costs than smaller practices, nor that London practices had higher costs than those in other regions.

Aggregate cost per student session per practice.
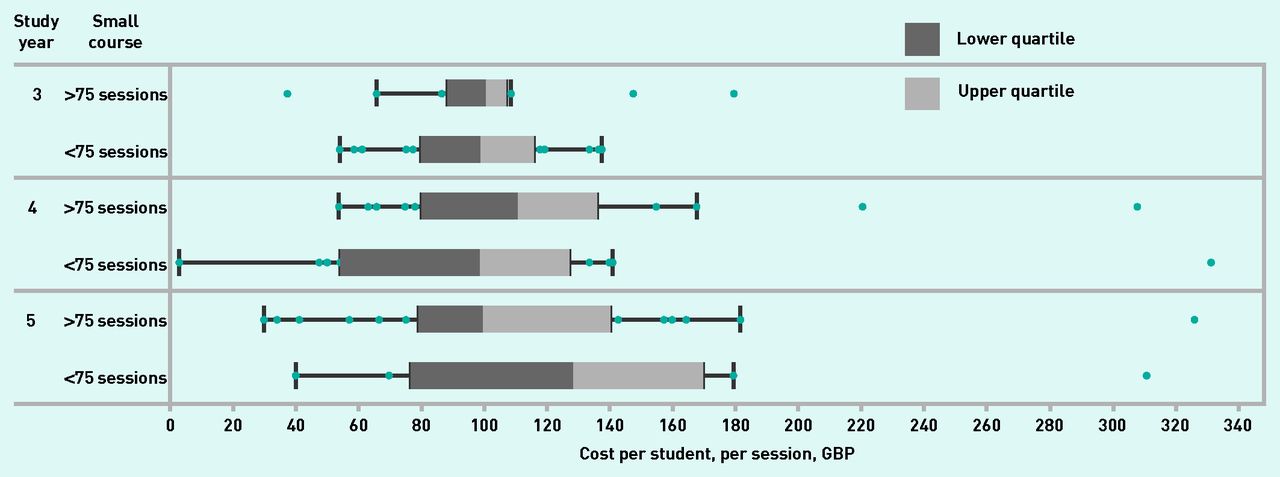
Variation in cost per year of study
There was variation in cost per student session between practices across all years of study with high and low outliers. For example, in year 4 of study the cost ranged from 3 GBP to 330 GBP per student session, though the authors suspect the extreme outlying figures may not be entirely reliable (Figure 2). Most teaching was delivered in years 3, 4, and 5 (year 6 is excluded because of small numbers). Figure 2 shows less variation in costs incurred by practices, with a trend to lower costs for practices that delivered greater volumes of teaching. For example, in year 4 the difference between the upper and lower quartiles (middle 50% of data) was around 55 GBP for practices delivering >75 sessions, chosen as being around the mean number of sessions delivered by practices during the clinical years, and 80 GBP for those delivering <75 sessions. However, the authors are unable to say if this was a real effect of economies of scale.

Cost distribution by amount of teaching.
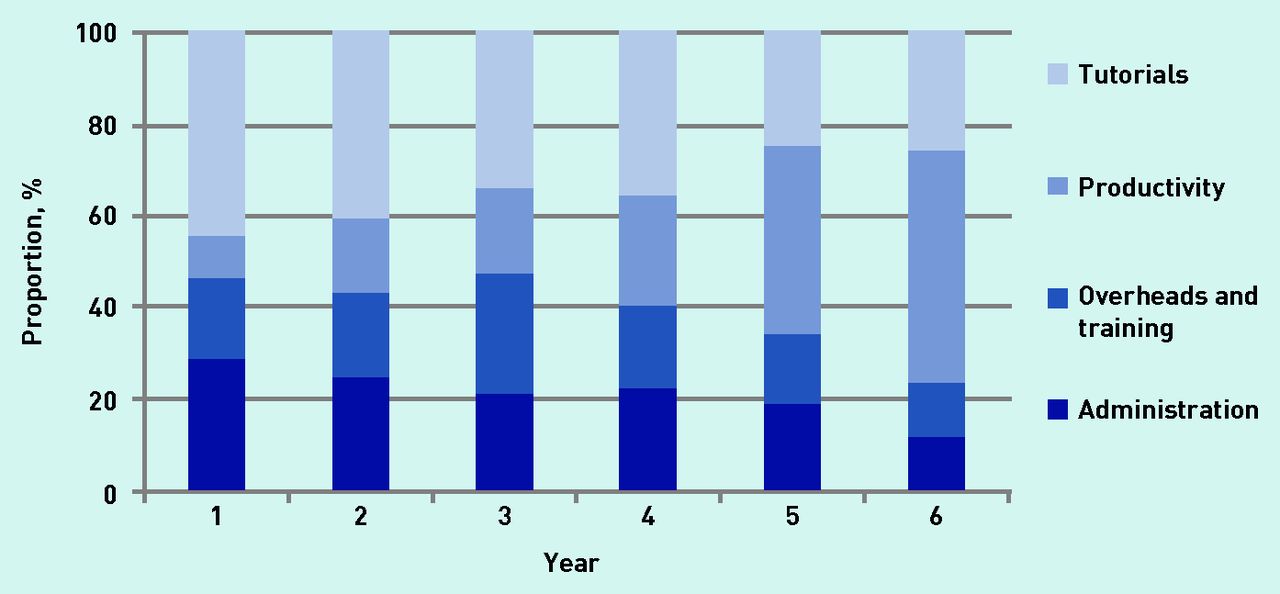
Cost components
Figure 3 shows how the relative contribution of different cost components varied by year of study. For first- and second-year placements a higher proportion of costs was for tutorials and administration of placements, whereas in later years of study the majority of costs were due to lost productivity for clinicians supervising students.
{kind=link}
{kind=link}
{kind=link}
Distribution of spending between cost components.
Based on these results the actual cost of placing a medical student full time in general practice for one academic year is in the region of 40 700 GBP (53 640 USD).
DISCUSSION
Summary
This study has provided the first detailed estimate of the costs of undergraduate education in general practice based on a sample of teaching practices representing all medical schools in England. Data from 11 061 teaching sessions involving a total cost to these 49 practices of 2.18 million GBP were identified. A mean cost to practices of 111 GBP (95% CI = 100 to 121) per student session of education provided was derived. There was substantial variation in costs between practices that could not be explained by practice size, location, or volume of teaching provided by the practice. There was little variation in cost of provision of placements by students’ year of study and no evidence of costs varying by geography.
Strengths and limitations
The strengths of this study are first that the methodology was agreed by a broad group of stakeholders representing those who pay for clinical education (DHSC and HEE), medical schools (MSC), academic general practice (SAPC, COGPED, and RCGP), and the medical trade union (BMA). The methodology was analogous to that used previously to cost medical undergraduate teaching in secondary care. Data management and analysis was carried out by the Workforce Information and Analysis team at the DHSC, who were independent of general practice. Data management included a rigorous data quality review. Although not designed to be a completely representative sample of all practices that provide teaching, the authors obtained data from at least one practice from every medical school in England and from at least two for 22 of the 25 schools, thus obtaining data from 94% of the initial sample. The authors obtained data from every English region and from a range of practices serving inner-city, suburban, and rural practices. Data were collected using a carefully designed and piloted template and with detailed guidance for completion. Practices’ confidence in the accuracy of their cost estimates was higher than that of teaching hospitals for the 2013 secondary care collection (personal communication, Workforce Information and Analysis team, 2019).
In terms of limitations, the authors acknowledge that there would have been differences in interpretation of some costing questions by practices that would have accounted for some of the variation. Also, significant known costs of teaching in general practice that are borne by students and by medical schools were not included. For example, the median distance between an English medical school and a teaching practice is 27 km, which results in significant travel and accommodation costs not included here.12 Neither are the substantial costs to medical schools of developing, managing, and quality assurance of the general practice programmes included here.13
Nonetheless, the overall results of this study provide, for the first time, strong evidence that the costs of providing undergraduate placements in general practice are considerably in excess of the funding made available for primary care undergraduate education at the time of writing. The actual costs are in fact broadly comparable with the significantly greater funding provided for placements in secondary care. Based on these results, the realistic cost of placing a medical student full time in general practice for one academic year is in the region of 40 700 GBP (53 640 USD). This is in stark contrast to the average payment rate for primary care of 22 000 GBP (28 990 USD) per year (unpublished data, HEE Finance, 2016; further details available from authors on request).
Comparison with existing literature
There has been only one previous attempt to estimate the cost of teaching in general practice.10 This previous study was based on an audit of overall placement spend by 15 medical schools and did not examine actual costs at individual practice level.
Despite using a different costing methodology, it produced a similar cost estimate to the present study.
Implications for research and practice
The need to increase recruitment of medical graduates to general practice is a matter of national concern, and promoting general practice as a positive career choice for graduating students is an NHS priority.2 The 2018 RCGP report, Destination GP, highlighted the critical role of GP teachers and high-quality clinical placements in developing the future GP workforce.14 Alberti et al, in 2017, demonstrated a significant association between the quantity of authentic clinical general practice teaching at each medical school and the percentage of its graduates who entered GP training after their foundation programme.15 Although most GPs do recognise the importance of medical students gaining experience in primary care, their willingness and ability to offer placements is already being squeezed by increasing service demands, staff shortages, and large increases in postgraduate teaching.16 If this evident under-resourcing of undergraduate placements in general practice is allowed to continue, it seems to the present authors inevitable that there will be further attrition in placement capacity, with serious consequences for the NHS workforce. Further mixed-methods research is required to explore this important issue and to describe the willingness and capacity of primary care to deliver high-quality educational experience for both the GPs and secondary care doctors of tomorrow.
Acknowledgments
The authors would like to thank all colleagues who have supported this study and in particular: the Workforce Information and Analysis team at the DHSC, all members of the DHSC/HEE Primary Care Education Working Group, all heads of GP teaching at English medical schools, Katie Petty-Saphon at Medical Schools Council, and all the teaching practices who provided data for analysis.
Notes
Funding
Each medical school in England agreed to support local costs of up to 500 GBP per practice to two practices to provide backfill time for one clinician and one manager to collect relevant data and complete the costing template.
Ethical approval
Research ethics approval was not required as no person-specific data were included.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors are employed by universities that deliver community-based medical education and did not receive any funding to conduct this study. The survey on which this study is based was commissioned by the DHSC/HEE Primary Care Education Working Group to fulfil its remit and the decision to publish negotiated by Joe Rosenthal, John L Campbell, and Robert K McKinley, who are members of the Working Group.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received April 24, 2019.
- Revision requested June 3, 2019.
- Accepted July 8, 2019.
- © British Journal of General Practice 2020
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

