


Abstract
Background Implementation science experts recommend that theory-based strategies, developed in collaboration with healthcare professionals, have greater chance of success.
Aim This study evaluated the impact of a theory-based strategy for optimising the use of serum immunoglobulin testing in primary care.
Design and setting An interrupted time series with segmented regression analysis in the Cork–Kerry region, Ireland. An intervention was devised comprising a guideline and educational messages-based strategy targeting previously identified GP concerns relevant to testing for serum immunoglobulins.
Method Interrupted time series with segmented regression analysis was conducted to evaluate the intervention, using routine laboratory data from January 2012 to October 2016. Data were organised into fortnightly segments (96 time points pre-intervention and 26 post-intervention) and analysed using incidence rate ratios with their corresponding 95% confidence intervals.
Results In the most parsimonious model, the change in trend before and after the introduction of the intervention was statistically significant. In the 1-year period following the implementation of the strategy, test orders were falling at a rate of 0.42% per fortnight (P<0.001), with an absolute reduction of 0.59% per fortnight, corresponding to a reduction of 14.5% over the 12-month study period.
Conclusion The authors’ tailored guideline combined with educational messages reduced serum immunoglobulin test ordering in primary care over a 1-year period. Given the rarity of the conditions for which the test is utilised and the fact that the researchers had only population-level data, further investigation is required to examine the clinical implications of this change in test-ordering patterns.
- diagnostic tests
- health services overuse
- immunoglobulins
- implementation
- interrupted time series analysis
- primary health care
INTRODUCTION
Healthcare budgets worldwide face increasing pressure to reduce costs and remove inefficiencies, while maintaining quality and safety. Laboratory testing is a major component of healthcare budgets, and demand for laboratory testing is increasing faster than other medical activity.1,2 There are many reasons for this rise, including the availability of new tests2,3 and clinical practice guidelines advising earlier screening to detect occult disease.4,5 Given the increasing financial pressure on health systems, judicious laboratory testing is imperative. However, evidence suggests that many laboratory tests are ordered unnecessarily.4,6,7 As well as the cost implications, this can lead to harmful downstream effects, such as further follow-up testing, specialist referrals, and invasive diagnostic procedures.8,9
Serum immunoglobulins are a group of tests that pose particular challenges for primary care physicians. The test is primarily used to help with the diagnosis of haematological disorders such as myeloma and lymphoma. These disorders are rare, and their symptoms can be vague, non-specific, and overlap with a wide range of other conditions.10 Thus, immunoglobulin testing is probably best undertaken as a second-line investigation where there are other tests, such as a full blood count or radiological abnormalities, which indicate the possibility of a haematological disorder. Deciding when to request immunoglobulins can be challenging for primary care physicians and requires clinical judgement in the context of non-specific clinical features.11 In the UK, one of the largest increases in primary care test use between 2005 and 2009 was for serum immunoglobulins with a relative increase of 73.4%, from 61 to 106 tests per physician per year.12 There has been no contemporaneous increase in the incidence of blood dyscrasias that might explain this rise. Serum immunoglobulin levels are often difficult for GPs to interpret.11 The practical implication of this is that results which show the very common finding of a polyclonal gammopathy (benign reactive finding) are sometimes interpreted as myeloma or pre-myeloma and generate unnecessary referrals to secondary care, which can lead to patient anxiety.
Using serum immunoglobulins as a ‘screening’ tool may result in overdiagnosis of monoclonal gammopathies of undetermined significance (MGUS), requiring annual life-long monitoring.10 As a result, MGUS can have a huge burden on a healthcare system; the estimated annual cost for MGUS monitoring in the US is at least 109 million USD.13 The risk of progression to symptomatic myeloma requiring treatment is <1%.14 Hence, overdiagnosis may increase anxiety among patients, reducing quality of life.15 However, reaching a diagnosis of myeloma is often very difficult, with a long diagnostic period compared with other cancers.16,17 In particular, identifying myeloma in primary care is very difficult owing to the complexity of presenting. As a result, recent research has focused on identifying the best inflammatory markers for the initial investigation of possible myeloma in primary care,17 to guide GP decision making on test ordering. Hence, there is the potential to improve the use of serum immunoglobulin tests in primary care.
| Ideally laboratory tests must be appropriately ordered, reported promptly, correctly interpreted, and inform future diagnosis and treatment of the patient. Serum immunoglobulin tests should be ordered as part of the primary screen for suspected plasma cell dyscrasias or periodically to monitor disease progression for already diagnosed conditions, such as myeloma. However, interpretation of abnormal results can be difficult. Abnormal findings can also lead to increased uncertainty and a cascade of further tests. Further research in primary care is needed to improve test ordering practices and to guide GPs on when to use, and how to interpret, these and other tests. This quasi experimental study evaluates a laboratory based intervention specifically targeting serum immunoglobulin tests, which may be applicable to many other tests. |
How this fits in
The authors’ previous systematic review found that educational strategies, feedback, and changing test order forms may improve the efficient use of laboratory tests in primary care.18 In a related study, the authors used interviews with primary care physicians to explore different options for improving the use of serum immunoglobulins.11 The interviewees expressed a lack of confidence in their ability to use the tests and were concerned about factors that could lead them to overuse the test in some circumstances (for example, for fear of litigation) and underuse them in others (such as where there may be an apprehension of generating the extra workload associated with liaising with haematology specialists). The study found that interventions focused on education (increasing knowledge or understanding: what to do and why), enablement (increasing means and/or reducing barriers to increase capability or opportunity), persuasion (using communication to induce positive or negative feelings or stimulate action), and environmental restructuring (changing the physical or social context) were most likely to help the GPs successfully change their ordering behaviours.11
Theory-based interventions utilise a combination of behaviour change models to select and design an intervention strategy.19 The mechanisms for changing test ordering (barriers and enablers) for this study were identified using the theoretical domains framework (TDF) and corresponding capability, opportunity, and motivation conditions of the ‘behaviour change wheel’ known as the COM-B model,20 which has been explained elsewhere.11 Intervention content was then specified in terms of component behaviour change techniques (BCTs)21 and were based on the four intervention functions identified in the authors’ previous qualitative research.11 Box 1 gives an overview of how these BCTs and intervention functions informed intervention content.
| Behaviour change technique | Function | Definition of function | Intervention component |
|---|---|---|---|
| Instructions on how to perform the behaviour | Education | Increasing knowledge or understanding | Provide guidelines on when to request the test and how to manage abnormal results using an algorithm |
| Credible source, information about health consequences | Persuasion | Using communication to induce positive or negative feelings or stimulate action | Provide guidance on how to manage patients with abnormal immunoglobulin test results |
| Restructuring the physical environment; adding objects to the environment | Environmental restructuring | Changing the physical or social context | Provide automated interpretive comments to test reports |
| Prompts and cues | Enablement | Increasing means/reducing barriers to increase capability or opportunity | Provide details on how to interpret test results |
Overview of the theoretical framework used for designing the intervention: behaviour change techniques, intervention functions, and selected intervention components
The aim of this study was to use laboratory data and an interrupted time series design to determine the impact of this intervention on serum immunoglobulin ordering rates.
METHOD
Study sample and setting
Participants were all GPs located in a large geographical area: the Cork and Kerry region of the Republic of Ireland. The region has a combined population of 664 534, with low population density and long distances between practices and hospital laboratories outside of Cork City. All serum immunoglobulin tests for the population are performed at one laboratory, located in Cork University Hospital (CUH).
Description of intervention
The first component of the intervention targeted decisions of when to request an immunoglobulin test and how to further evaluate a patient with an abnormal finding. This involved creating a 1-page guideline algorithm design based on current UK guidelines (Appendix 1).10 These guidelines provided information on when to request an immunoglobulin test, along with a patient evaluation plan following the test request.
The second element of the intervention assisted with the interpretation of test results. Eight educational messages (Box 2) were developed by a multidisciplinary team of senior laboratory scientists and consultant haematologists based on myeloma guidelines10 and reviewed by a professor of general practice to ensure they were appropriate for a GP audience. The brief educational messages provided interpretive comments on test results and were added to the test reports sent to the requesting GP. These messages were activated using electronic ‘action cues’, which were defined as triggers or prompted for an action to be taken.22 For example, ‘raised IgM with a normal electrophoresis’ prompts the addition of the following interpretive message to the test results:
‘Patient has a slightly raised IgM. If antimitochondrial antibodies are negative, this may be consistent with recent infection, particularly viral. If antimitochondrial antibodies are positive, this may be consistent with primary biliary cirrhosis.’
| Test | Action cue | Brief educational message |
|---|---|---|
| ELE | Raised alpha-1 and alpha-2 globulins | Pattern may be consistent with low-grade inflammation |
| IgG | Diffusely raised IgG | Pattern of persistent infection or inflammation |
| IgG, IgA | Diffusely raised IgG and IgA | Polyclonally raised IgG and IgA: pattern of persistent infection or inflammation |
| IgA, IgG, IgM | IgA deficiency (IgA must be <0.1 g/l with a normal IgG and IgM with a normal pattern) | Normal electrophoretic pattern but very low total IgA concentration: would be consistent with IgA deficiency. This is seen in approximately 1/500 of the population and often without clinical consequence |
| IgM | Raised IgM with a normal electrophoresis | Patient has a slightly raised IgM. If antimitochondrial antibodies are negative, this may be consistent with recent infection, particularly viral. If antimitochondrial antibodies are positive, this may be consistent with primary biliary cirrhosis |
| IgA, ELE | Raised IgA with a normal electrophoresis | Normal electrophoresis pattern with a slightly raised IgA: may be consistent with mucosal inflammation, autoimmune illnesses, or liver disease |
| IgM | Low IgM in an older patient (>70 years) with normal electrophoresis | Slightly low IgM: this may be an incidental finding, particularly in older patients, but it may also be an indicator of some secondary immune suppression |
| Interpretive comment for when a paraprotein is present | ||
| PARA | If a faint band is present | Serum shows a small paraprotein with normal background gamma. This pattern could be an incidental finding in a patient of this age or may be seen secondary to recent infection. However, urine must be checked for Bence Jones protein and suggest recheck serum in 3–4 months to assess any progression. If you do have strong clinical indications, for example, hypercalcaemia, renal impairment, anaemia, bone pain, etc., suggest investigate further |
ELE = serum protein electrophoresis. IgA = immunoglobulin A. IgG = immunoglobulin G. IgM = immunoglobulin M. PARA = paraprotein.
Details of the eight educational interpretive comments attached to test reports: targeted laboratory tests, educational interpretive comments, and cues
Previously, GPs detected a ‘raised IgM with a normal electrophoresis’ based on the provided reference ranges for abnormal levels (>2.9 g/L). During the study period and thereafter, the GP received an interpretive comment added to the test result, which further explains the test result and possible cause or diagnosis. This information (Box 2) supports the GP with their patient management plan.
Delivery of intervention
The intervention strategy was introduced in October 2015. This involved sending a one-time hard copy of the guideline to all GPs practising in the Cork and Kerry region. GPs using laboratory services at CUH were identified through Health Service Executive records. The laboratory-based educational messages were programmed into the laboratory system. A three-phase quality testing process (initial assessment, implementation plan, and a review of effectiveness) was performed by the laboratory before the intervention was implemented using hypothetical patients. The messages were activated and embedded in electronic GP test reports each time the ‘action cue’ occurred.
Data collection
The count of immunoglobulin tests ordered by GPs in the Cork and Kerry region between January 2012 and October 2016 was compared before and after the introduction of the intervention. These routinely collected data were extracted from the hospital’s laboratory system using Cognos Impromptu data extraction software and imported into Stata (version 12) for analysis.
Study design
The combined guideline and educational messages intervention was evaluated using a quasi-experimental interrupted time series (ITS) design and complied with the quality criteria for ITS studies adapted by Ramsay and colleagues;23 the quality criteria for ITS studies are available from the authors on request. Total immunoglobulin requests were calculated at fortnightly time points. Time was rescaled so that the starting fortnightly segment was assigned number 1 (17 January 2012), with time being measured backwards and forwards from the date the intervention was introduced (20 October 2015). This resulted in 96 time points pre-intervention and 26 time points post-intervention. A sufficient number of time points before and after the intervention was needed to conduct segmented regression analysis, at least 12 data points before and after the intervention (based on power). There also needed to be a sufficient number of observations (a minimum of 100 is desirable) at each fortnight segment to achieve an acceptable level of variability of the estimate at each time point.24
Statistical analysis
A segmented Poisson regression model was used to examine the impact of the intervention, estimating the trend in the volume of immunoglobulin test orders before the intervention (January 2012 to October 2015) and the changes in trend following the intervention (October 2015 to October 2016). The mean count was modelled as a log-linear function of time with a potential change in slope and level at time of intervention. Segmented regression analysis of ITS data allowed the authors to assess how much an intervention changed an outcome of interest, immediately (level change) and over time (trend change). As a separate control group was not available, the model could not control for other events that may have influenced the outcome. However, the level and trend of the pre-intervention segment served as the control for the post-intervention segment in single-group time series, still addressed important threats to internal validity, and represented a methodologically acceptable design for measuring the impact of interventions, previously recommended for evaluating healthcare-based interventions.23,25 The three outcomes in the ITS analysis were the change in the count of test orders immediately after the intervention, the difference between pre-intervention and post-intervention slopes (trend change), and the estimation of fortnightly average intervention effect after the intervention.
Regression analysis definitions
Four variables were included in the dataset. T: the time elapsed since the start of the observation period (17 January 2012) expressed in fortnightly segments; Xt: a dummy variable indicating the pre-intervention period (coded 0) and post- intervention period (coded 1); TXt: the time elapsed since the intervention and Yt: the outcome at time t. The following segmented regression model was used for this analysis:
 where β0 represents the baseline level at T = 0, β1 estimates the change in mean fortnightly test orders before the intervention, that is, the underlying pre-intervention trend, β2 estimates the level change in the mean number of test orders immediately after the intervention, and β3 estimates the change in the trend (slope) in the mean fortnightly number of test orders after the intervention, compared with the trend before the intervention (using interaction term for time and intervention: TXt). The sum of β1 and β3 is the post-intervention slope.
where β0 represents the baseline level at T = 0, β1 estimates the change in mean fortnightly test orders before the intervention, that is, the underlying pre-intervention trend, β2 estimates the level change in the mean number of test orders immediately after the intervention, and β3 estimates the change in the trend (slope) in the mean fortnightly number of test orders after the intervention, compared with the trend before the intervention (using interaction term for time and intervention: TXt). The sum of β1 and β3 is the post-intervention slope.
Checking for seasonality and wild data points
Many laboratory tests have a seasonal pattern owing to the nature of the condition for which the test is requested. Seasonality can cause autocorrelation and overdispersion. The authors checked for seasonality using Fourier terms (pairs of sine and cosine functions).26 Extreme values known as wild data points were dealt with by assessing the data plot for any outliers and following recommended methods for handling such data.24
RESULTS
In total, 17 442 tests were requested in the pre-intervention period, including 5988 in the year pre-intervention (October 2014 to October 2015) and 5396 tests in the post-intervention period (October 2015 to October 2016). Table 1 presents an overview of the patient characteristics associated with test orders in pre-intervention and post-intervention periods.
Crude overview of patient characteristics of immunoglobulin test requests for 1-year pre- and post-intervention periods
Effect of the intervention
Table 2 provides the results of the segmented Poisson regression modelling the effects of the intervention on fortnightly GP requests for immunoglobulins. These are presented as incidence rate ratios (IRRs) with corresponding confidence intervals (CIs) and P-values.
Effect of intervention on fortnightly requests for serum immunoglobulins
Change in trend following the intervention (Model B)
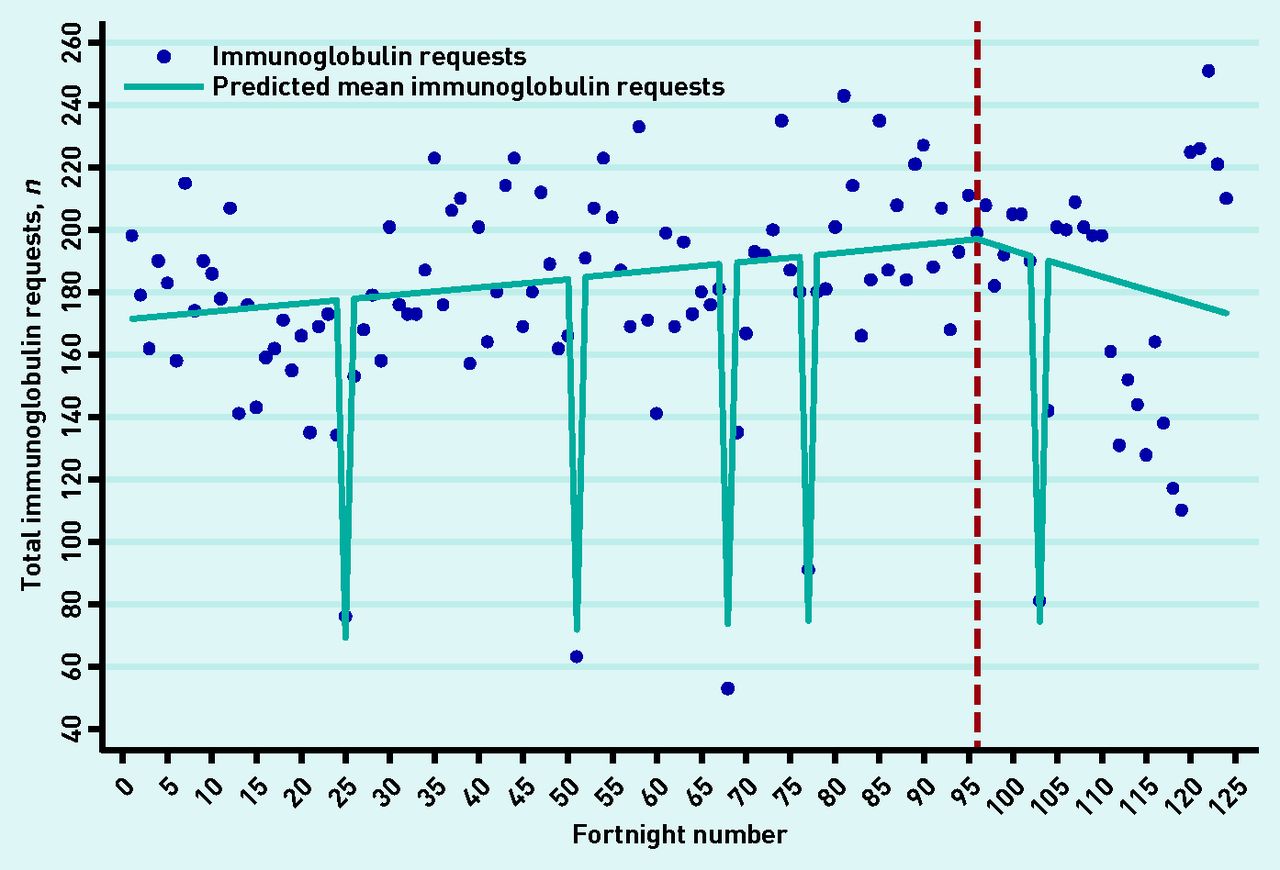
There was a statistically significant reduction in the slope after the introduction of the intervention (Figure 1). Before the introduction of the intervention, test orders were increasing at a rate of 0.16% per fortnight (P<0.001). After the strategy had been implemented, test orders were falling at a rate of 0.42% per fortnight (IRR 0.996, 95% CI = 0.993 to 0.998; P<0.001), with an absolute reduction of 0.59% in the slope per fortnight, corresponding to a reduction of 14.5% over the 12-month study period.
{kind=link}
Interrupted time series (ITS) model with a trend change regression model (model B). Blue line: predicted slope based on the regression model allowing for a December effect. Red dashed line: the introduction of intervention. The time points at fortnights 25, 52, 77, and 103 (dips in data) represent the same fortnightly time period in December each year and 68 represents a known wild point owing to laboratory error.
Adjusting for seasonality and outliers
The association was largely unaffected by seasonality. Five outliers were evident in the data. At fortnight 68 (August 2015) an IT laboratory system failure was responsible for a marked drop in requests, and fortnights 25, 52, 77, and 103 all mark the same 2-week period in December each year (2012 to 2016) with consistently low test orders. These time points were controlled for in each of the segmented regression models found in Table 2.
DISCUSSION
Summary
To the authors’ knowledge, this is the first study to systematically design an intervention using a combination of theoretical approaches to improve test ordering in primary care. In the year following the introduction of the intervention, test orders for serum immunoglobulins fell by 0.59% per fortnight, which corresponds to a 14.5% reduction over the 1-year period, compared with the trend before the intervention.
Strengths and limitations
A strength of this study was the systematic use of both qualitative and quantitative research methods, with explicit use of theory to create an intervention tailored to target barriers to changing clinicians’ behaviour.19 A multidisciplinary team including biochemistry, haematology, and primary care representatives were involved in the development of the intervention. Finally, all immunoglobulin results requested by GPs in the two studied counties were analysed.
Segmented regression models have some limitations. The unit of analysis in the model was the fortnightly count of immunoglobulin tests, rather than each GP’s individual test-ordering counts per fortnight. Contrary to cross-sectional analysis methods, such as logistic regression, segmented regression analysis of time series data does not allow control for the patient or GP-level covariates. These would only confound the time series results, however, if they predicted the outcome and changed in relationship to the time of the intervention: this is unlikely to be the case. Finally, though the interpretive messages devised in this study were based on best-practice guidelines at the time of design,10 these messages should be updated and revised as new evidence emerges for best practice. For example, any future educational messages of this kind would be strengthened by the inclusion of most recent evidence around negative predictive values of normal inflammatory markers.17 Moreover, the authors have not measured the potential impact on the diagnosis of blood dyscrasias.
Comparison with existing literature
This study set out to optimise laboratory ordering, using serum immunoglobulin tests as a case study. At the outset, there was a possibility of test ordering increasing, decreasing, or remaining the same. The authors observed a reduction in test orders post-intervention. Therefore, a reasonable interpretation of the present findings is that, before the intervention, the level of test overuse was larger than the level of underuse, and the intervention, which deals with both problems, has led to a net reduction in test ordering.
A possible explanation for this net reduction is the use of detailed interpretive comments provided on the test results. As found in a previous study by the authors, before the intervention, GPs expressed the need for specialist interpretation of test results, ideally accompanying the test result, as they do not always know or may be unable to recall all the possible reasons for particular findings.11 GPs also mentioned ‘fear of litigation’ and ’fear of missing a myeloma’ as other drivers of test ordering.11 Diagnostic uncertainty has been cited as a common reason for inflammatory marker testing in primary care.27 Providing clear guidelines and interpretive comments on results may have increased confidence in GPs to request fewer tests. The authors’ previous systematic review also found similar educational strategies incorporating guidance successful at reducing other laboratory tests.18 On the other hand, it is also probable that, in a smaller group of patients, tests are now being ordered where they previously would not have been. For example, a small number of GPs expressed concern that they were unaware of certain clinical scenarios where immunoglobulin evaluation could be useful. The educational requesting algorithm may have increased awareness of these clinical scenarios.11 However, this may also be explained by variation in test ordering caused by physician-level factors,28 such as risk adversity.29 For example, in the authors’ previous related study examining physician-related factors associated with serum immunoglobulin test ordering, they found that female sex and having less experience were associated with higher test ordering.28
Implications for research and practice
The use of a laboratory system to deliver interpretive comments on test results is a transferable strategy for all laboratories in Ireland, and internationally also as hospital pathology laboratories generally have customisable systems with the capacity to readily alter the end user report. The present findings suggest that GP test ordering may be improved by an intervention based on a guideline with educational messages; however, further research is required to explore the clinical impact of this. For example, most abnormal results involve benign elevations of immunoglobulins that are not owing to cancer (or pre-cancer correlates of the paraproteins). Thus, these messages may have shaped GP ordering behaviour by constantly reminding them of the benign nature of most abnormal serum immunoglobulin results. However, it may also be likely that potential effects of educational messages are seen in the downstream activities resulting from serum immunoglobulin test ordering, such as referrals to secondary care, which requires further investigation. However, the authors cannot say definitively that appropriateness has been improved. Further research, using individual patient-level data, is required: particularly to exclude the unlikely possibility that the intervention has led to tests being denied to patients who need them. In addition, further research is required to explore the wider clinical impact of the intervention.
Laboratory health information technology (IT) systems could support calibrating the quality and safety of diagnostic procedures, by providing feedback and communicating with GPs,30,31 leading to effective knowledge sharing.31 It is also likely that the theoretical behaviour change strategy used to design this intervention is applicable to other specialised tests.
A cost comparison for reagent suppliers for the same time period pre-intervention and post-intervention identified a reduction of over €1000 per month. The authors estimate that the reagent supply costs associated with serum immunoglobulin activity at CUH will decrease by €12 000 annually. While modest, the financial benefits to the public health service in Ireland will be much larger if the intervention presented here is applied to other settings and is found to work for other tests. This study was designed to target the key issues around GP serum immunoglobulin test-ordering behaviour. At a policy level, the findings point to the possible benefits of laboratories becoming more actively engaged in GP education about test ordering. Any such engagement should seek to understand drivers of the GP behaviour first, and interventions should be jointly developed with GPs on the basis of sound behaviour change theory.
Appendix 1. Copy of the guideline algorithm sent to GPs.

Notes
Funding
Sharon Cadogan was funded to complete this research by the Health Research Board in Ireland under the Scholars Programme in Health Services (research grant reference number: PHD/2007/16).
Ethical approval
Ethical approval was provided by the clinical research ethics committee of the Cork University Teaching Hospitals (reference number: ECM (ii) 07/01/14).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received February 18, 2019.
- Revision requested April 18, 2019.
- Accepted May 24, 2019.
- © British Journal of General Practice 2020
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

