


Abstract
Background Self-harm is a serious risk factor for suicide, a major public health concern, and a significant burden on the NHS. Rates of self-harm presentation in primary care are rising and GPs interact with patients both before and after they have self-harmed. There is significant public and political interest in reducing rates of self-harm, but there has been no robust synthesis of the existing literature on the role of GPs in the management of patients who self-harm.
Aim This study aimed to explore the role of the GP in the management of patients with self-harm behaviour.
Design and setting A systematic review and narrative synthesis of primary care literature.
Method This systematic review was conducted and is reported in line with PRISMA guidance. Electronic databases systematically searched were MEDLINE, PsycINFO, EMBASE, CINAHL, Web of Science, and AMED. Two independent reviewers conducted study screening and selection, data extraction, and quality appraisal of all included studies. Thematic analysis was conducted.
Results From 6976 unique citations, 12 studies met eligibility criteria and were included. These 12 studies, published from 1997–2016, of 789 GPs/family medicine physicians from Europe, the US, and Australia were of good methodological quality. Five themes were identified for facilitating GP management of self-harm: GP training, improved communication, service provision, clinical guidelines, and young people. Four barriers for GP management of self-harm were identified: assessment, service provision, local, and systemic factors.
Conclusion GPs recognise self-harm as a serious risk factor for suicide, but some feel unprepared for managing self-harm. The role of the GP is multidimensional and includes frontline assessment and treatment, referral to specialist care, and the provision of ongoing support.
INTRODUCTION
Self-harm is the strongest risk for suicide and a major public health challenge in the UK.1,2 Self-harm is a concern throughout the life-course, with more than half of young people who die by suicide having a history of self-harm.2 Among male patients, there are increasing self-harm rates reported in midlife, and in older adults (aged >65 years) self-harm raises the risk of suicide by 145 times.3,4 The increasing incidence and prevalence of self-harm are a significant burden on the NHS.5,6 An estimated 220 000 self-harm episodes present yearly to accident and emergency (A&E) departments in England.7
The rates of self-harm presenting to primary care are rising (there was a 68% increase in self-harm presentation in girls aged 13–16 years between 2011 to 2014), but only a minority of patients who self- harm in the community present to healthcare services.5,6,8,9 The National Institute for Health and Care Excellence (NICE) guidelines for self-harm highlight the important role primary care has in the management of patients who self-harm.4–6,10 However, there are only a few recommendations specific to general practice.10
In 2018, the NHS Zero Suicide Ambition was launched and the first Minister for Suicide Prevention in the UK was appointed, highlighting the growing national focus on suicide prevention.11,12 Reducing self-harm is a new key national priority for the National Suicide Prevention Strategy, and The NHS Long Term Plan commits to the development of primary care self-harm models.13,14
Two-thirds of patients who self-harm present to their GP in the month prior to a self-harm episode and in the month after an episode of self-harm.15 There is no synthesised evidence regarding the knowledge, attitudes, and behaviours of GPs, or the facilitators and barriers to GP management of patients who self-harm. Therefore, it is important to systematically study the role of the GP in the management of patients who self-harm.15
The aim of this systematic review was to explore the role of the GP in the management of patients with self-harm behaviour. Specific objectives were to:
study the knowledge, attitudes, and behaviour of GPs in the assessment and treatment of self-harm;
explore the barriers, facilitators, and areas of need for the GP management of self-harm in primary care; and
identify outcomes of GP consultations for self-harm.
| Self-harm presenting to primary care is rising. Two-thirds of patients visit their GP in the month preceding and the month following self-harm. There has been no systematic synthesis on the role of the GP in the management of patients who self-harm. The role of the GP is multidimensional and flexible throughout the patient journey, and includes frontline assessment and treatment, referral to specialist care, and ongoing support in primary care. This study will inform the development of primary care self-harm models as outlined in The NHS Long Term Plan. |
How this fits in
METHOD
Protocol
The protocol was registered with PROSPERO (CRD42018084703).16 This review was conducted and reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidance.17
Search strategy and information sources
Six electronic databases (MEDLINE, PsycINFO, EMBASE, Web of Science, AMED, and CINAHL) were searched from inception to 6 February 2018 using structured search strategies. The full MEDLINE search strategy can be found in Supplementary Table S1. Self-harm was defined in accordance with NICE guidelines as: ‘self-poisoning or injury, irrespective of the apparent purpose of the act’, thus including the term ‘suicide attempt’.10 ‘Parasuicide’, despite being an abandoned term, was included for thoroughness.18 ‘Suicidal ideation’ was incorporated as a search term to capture studies where self-harm data may have been reported. Reference lists of included studies were hand-searched. No language or location restrictions were applied.
Eligibility criteria
Studies were included if they reported relevant self-harm data from GPs/physicians/family physicians/primary care physicians. Self-harm data from patients of all ages were included. Observational, qualitative, and mixed-method study designs were all included. The study eligibility criteria are outlined in Box 1.
| Inclusion criteria population(s) and condition of interest | Population(s): GPs, family medicine physicians, family physicians, primary care physicians Condition of interest: Self-harm (SH), non-suicidal SH, deliberate SH, suicidal attempt/behaviour, parasuicide, suicidal ideation |
| Intervention(s)/exposure | Patients of all ages who have history of SH or have SH thoughts |
| Comparators | None |
| Outcome |
|
| Setting | International primary care |
| Study designs | Mixed methods, observational, qualitative |
| Exclusion criteria | Non-English-language studies where translation could not be obtained Studies only reporting outcomes on ‘assisted suicide’, ‘suicidal ideation’, and ‘suicide’ Studies that were randomised controlled trials Studies without doctors in ‘practitioner’ role Studies where medical students were in the ‘practitioner’ role |
Inclusion and exclusion criteria adopted in this review
Study screening and selection
Two authors independently reviewed all titles, abstracts, and full texts against predefined and piloted eligibility criteria. Discrepancies were resolved through discussion with a third author. Where appropriate, translations of full-text studies were sought in order to determine eligibility. References were managed through Legacy RefWorks.
Data extraction and quality assessment
Eligible full-text studies were subjected to data extraction and quality appraisal by two authors. Data were extracted on study aim, study design and location, number of clinicians, clinician knowledge, attitudes and behaviours, facilitators, barriers, consultation outcomes (referral, follow-up, and duration of consultation), and clinician and author-expressed training needs. It was necessary to request clarification from the corresponding authors of four of the studies, to ensure accurate representation of their data.
Terms were pre-defined (using Oxford English Dictionary definitions)19 to ensure consistency in data extraction:
Clinician ‘knowledge’: ‘facts, information, and skills, acquired through experience or education; the theoretical or practical understanding of a subject’.
Clinician ‘attitude’: ‘a settled way of thinking or feeling about something’.
Clinician ‘behaviour’: ‘the way in which one acts or conducts oneself, especially towards others’.
The Mixed Methods Appraisal Tool (MMAT) was used to assess methodological quality of included studies.20 Discrepancies in data extraction and quality assessment were resolved through discussion until a consensus was reached.
Narrative synthesis
A narrative synthesis of data was conducted using the framework developed by Popay et al.21 First, and prior to beginning this study, a theory was developed on the role of the GP (not reported here).
Second, a preliminary synthesis was developed and, on tabulation, patterns began to emerge. Third, relationships within and across studies were explored, achieved by the analysis of similarities and differences among them.
Thematic analysis enabled themes to be identified across studies, which were agreed on by all authors. Finally, the robustness of the synthesis was assessed (further details are available from the authors on request).
RESULTS
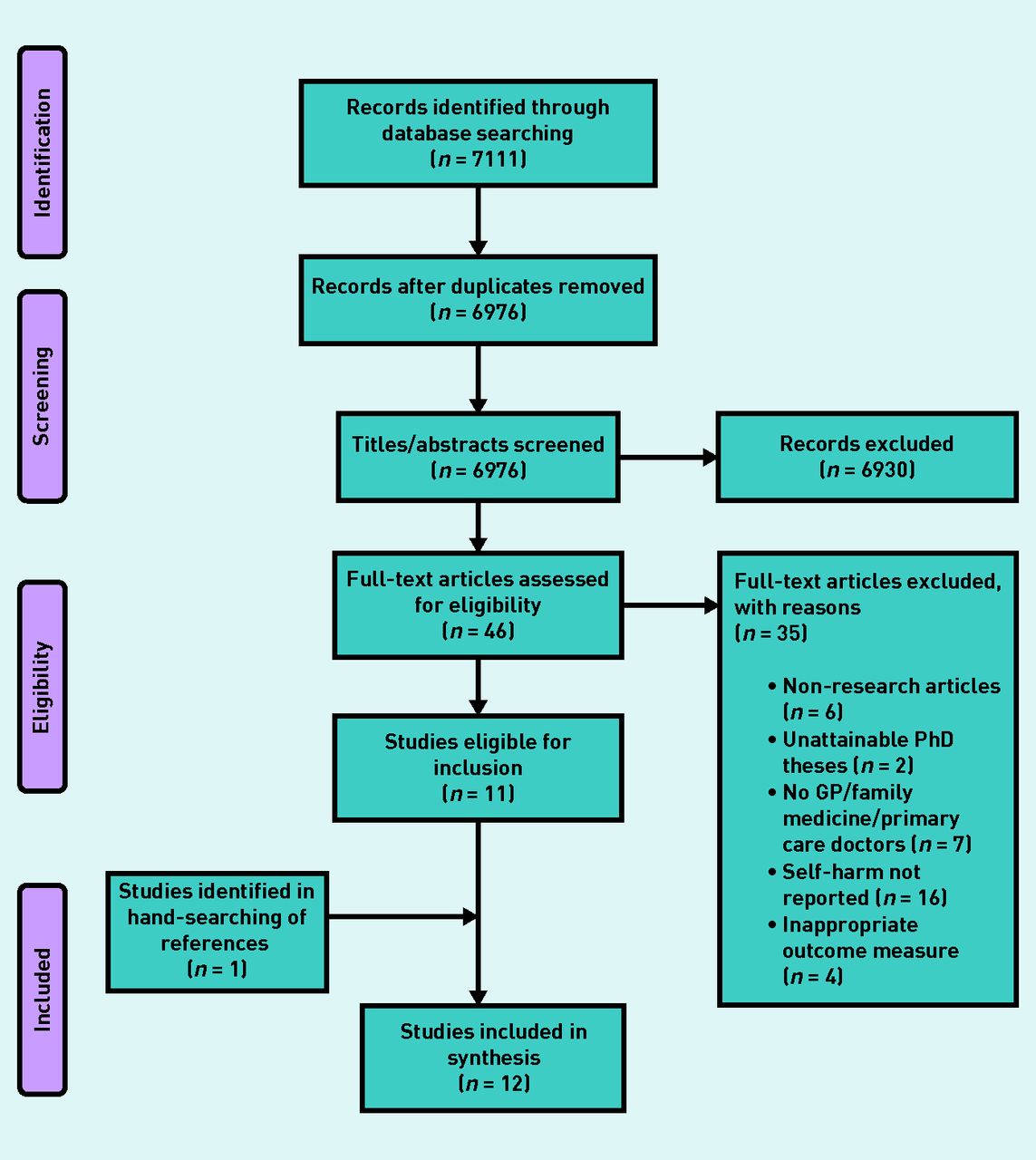
The search yielded 6976 unique citations, from which 46 full-text articles were reviewed for eligibility, and 12 studies were included in the final synthesis. Figure 1 outlines the flow of studies within the review.
{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Study characteristics
Table 1 details individual study characteristics. Included studies involved 789 GPs/family medicine physicians from Europe (n = 10), the US (n = 1), and Australia (n = 1).22–33 The clinician age range was reported to be 20–67 years, while male-to-female clinician ratio was 254:203.22–33
Characteristics of included studies
Quality assessment
The methodological quality of most of the included studies (n = 9) was high, scored as either 75% or 100%. Table 2 highlights MMAT study scores with reasons given for the studies that did not achieve a 100% score. Studies that scored poorly, rated 25% (n = 3), had unrepresentative samples, poor reporting of outcomes, used non-validated tools, and had a low response rate.27,30,33 Studies that scored 100% (n = 3) presented findings in the appropriate context with researcher reflexivity.24,28,29
MMAT results for included studies
Clinician knowledge, attitudes, and behaviours
In the following section, the primary outcomes of the systematic review are presented: clinician knowledge, attitudes, and behaviours, facilitators and barriers for GP management, consultation outcomes, and training needs. Within facilitators and barriers, the emergent themes that were identified from the data are reported.
Box 2 summarises the key similarities and differences across studies of clinician knowledge, attitudes, and behaviours.
| Across studies | Clinician knowledge | Clinician attitudes | Clinician behaviours |
|---|---|---|---|
| Similarities | Less self-harm training provided in comparison with general mental health, evidenced by only 39% of GPs receiving suicidal behaviour training in the previous 5 years26,30 | Self-harm a ‘cry for help’ and a ‘help-seeking behaviour’22, 28, 31 GPs want patients who self-harm to access mental health assessment27,29 Want to help patients who self-harm and see themselves as a frontline service for young people who self-harm25,26 Lack confidence assessing and talking to patients who self-harm, including young people22,25, 33 Feel self-harm is on a ‘spectrum of risk’ for suicide22,25 Use ‘gut feeling’ and instinct to manage risk with self-harm in adults and young people22,28 | Most refer patients who self-harm to hospital setting (mental health, A&E, ABC)23,24,27 Patients who self-harm are also managed in primary care22,23,25,27 |
| Differences | In young people there is uncertainty in establishing the severity of self-harm and future risk of self-harm28 GPs are aware risk of suicide greater in those who self-harm22 | Self-harm in young people as a coping strategy25 Few self-harm primary care services30 Feel hospital admission reinforces self-harm behaviour32 Self-harm common in older adolescents, linked to social problems, should not be ignored, and should be acknowledged for both young person and parent/carer25 Concerns over conflict with parents of young people and in alienating young person25 Difficult assessing suicide risk in patients who had self-harmed and in establishing suicidal intent according to patient demographic22 | Do not always intervene, and share responsibility for patient safety with patient22 Exhibit uncertainty when managing young people28 Ask direct questions with young people in lay terms while wanting to build rapport. Concerns over maturity of young people, signpost to services, and offer GP follow-up25 Lack of coding self-harm on electronic records29 Prescribe medication and undertake psychosocial intervention after self-harm23 More likely to intervene if documented suicidal ideation/behaviour23 In rural settings, referral influenced by service provision32 |
A&E = accident and emergency. ABC = ambulatory care.
Clinician knowledge, attitudes, and behaviours across studies
Knowledge
Some GPs attain some knowledge of managing self-harm, primarily through teaching and training. Three studies mentioned clinicians receiving additional training in self-harm.22,26,30 One study reported GP self-perceived competence on suicidal behaviour at an average of 3.2 (95% confidence interval = 3.1 to 3.4) on a 1–5 scale, with only 38% (35/91) of GPs having attended training in the past 5 years.26 Among included studies, reports concerning self-harm training being provided less than general mental health training were noted.30 GPs reported a taught theoretical link between self-harm and risk of suicide, but this was in contrast with practical experience of managing patients who self-harm as a means of ‘releasing’ emotions.22 Furthermore, there remains uncertainty among GPs over how to establish future risk of self-harm.28
Attitudes
Some GPs suggest that self-harm is help-seeking behaviour. Although positive in their attitude towards supporting patients who self-harm, GPs lack confidence in self-harm management. They rely on clinical instinct to guide risk assessment and recognise the challenge of identifying suicidal intent in self-harm risk assessment.
Three studies reported that GPs felt self-harm to be a ‘cry for help’ and help-seeking behaviour.22,28,31 One study described self-harm as being ‘tension release’ and another as being a coping strategy for young people.22,25 Two studies found that GPs believed patients with self-harm behaviour should have a mental health assessment.27,29 Another study reported that GPs want to support patients who have self-harmed, and have a positive attitude towards people with self-harm behaviour.26 One study reported that GPs see themselves as frontline support for young people and as a ‘stop-gap’ service for young people with self-harm behaviour awaiting specialist assessment.25
Three studies suggested that GPs lack confidence and that 53% (137/260) felt unprepared when assessing and communicating with patients who self-harm, especially when working with young people, and assessing suicide risk.22,25,33 GPs considered that self-harm is on a ‘spectrum of risk’ for suicide, with some GPs finding it difficult to separate self-harm from ‘suicidality’ (self-harm with suicidal intent).22,25
GPs in one study commented that identifying suicidal intent is imprecise, and also that the patient may not be able or want to disclose suicidal intent if present.22 They suggested that the difficulty lies in the complex and close relationship between self-harm and suicide.22 Two studies reported that GPs use instinct and ‘gut feeling’ when conducting self-harm risk assessment and management in adults and young people.22,28
In another study, GPs emphasised the lack of accessible self-harm primary care services.30 A further study found that GPs felt that hospital admission following self-harm reinforces self-harm behaviour.32
GPs working with disadvantaged patient groups seemed more likely to suggest that suicide risk assessment is an imprecise practice because their patients’ lives were described as being volatile and dangerous.22
Interestingly, GPs who worked in rural and affluent areas discussed self-harm with and without suicidal intent as being distinct clinical behaviours.22
In one study, GPs felt that self-harm in young people should be acknowledged for both the young person and the parents or carers, and not ignored in the consultation.25 GPs stated that self-harm is linked to social problems and is more common in older adolescents (age 15–18 years).25 They also had concerns about potential conflicts with the parents or carers of young people, and thus isolating the young person who self-harms.25
Behaviours
GPs appear to adopt different consultation strategies when assessing self-harm in adults versus young people, and use an array of treatment options. They reported managing self-harm by utilising both primary and secondary care services.
Three studies described GPs referring patients with self-harm behaviour to different secondary care settings; A&E, ambulatory care, and mental health services.23,24,27 Four studies mention GPs managing self-harm in primary care.22,23,25,27
One study described a GP who reported not always intervening with a self-harm patient with suicidal thoughts, reflecting the responsibility back onto the patient.22 A further study described GPs using direct questions, lay terminology, and building rapport with young people who self-harm.25 Another study portrayed uncertainty among GPs when managing young people with self-harm behaviour.28
One study reported the lack of self-harm coding in electronic general practice records, and in a separate study, in rural settings, GP referrals are influenced by service provision.29,32 Crawford and Wessely23 identified that GPs undertake psychosocial interventions post-self-harm, begin or continue prescription of psychotropic medication, refer to community counselling, and are more likely to intervene if the patient’s suicidal behaviour/ideation has been documented.23
Facilitators
Five themes around facilitators to GP management of self-harm in primary care emerged from the synthesis:
GP training
Training was an important facet to improved care of patients with self-harm behaviour and is key to improving care of patients with self-harm behaviour.25,27,28,30,33 Specific types of training highlighted included continuing professional development (CPD) on self-harm, communication skills for the primary care team, GPs learning brief psychosocial interventions, and assessment of young people.25,27,28,33 An improvement in GP confidence in suicide risk assessment, and self-harm training within the primary care context, were identified.22,30
Improved communication
Enhanced communication between primary care and mental health teams is an essential facilitator. Four studies relayed the need for better communication between mental health (Community Mental Health Teams/Child and Adolescent Mental Health Services [CAMHS]) and primary care teams on patient risk assessment, treatment plans, follow-up, and discharge.25,27,30,32
Service provision
Enhanced service provision for self-harm in primary care would support GP management. A single point of access (SPOA) for patients who self-harm, and a keyworker operating across practices focusing on information sharing and mental health care integration, were two proposals.29 A community psychiatry nurse (CPN), counsellor, or psychologist attached to practices were also suggested.29 The need for dedicated primary care self-harm services was highlighted.29,30
Clinical guidelines
The co-production of self-harm guidelines is key for effective GP self-harm management. Three studies identified a need for co-produced self-harm clinical guidelines across all age groups.29,30,33 The use of general practice self-harm risk tools and implementation of self-harm management guidelines was advocated by GPs in one study.32
Young people
Parents and carers of young people have an important part to play in the management of young people who self-harm. Two studies described the involvement of parents and carers in help-seeking and in the consultation as a facilitator.25,28 Another study reported GPs considered that asking young people to complete a questionnaire (questionnaire content not stated) ahead of the next consultation would assist them in management.25
Barriers
Four themes on barriers to GP management of self-harm in primary care emerged from the synthesis:
Assessment
Time and confidence were reported to affect GP assessment of patients with self-harm behaviour.22,25,28,29 Feeling unprepared and having a lack of specialist knowledge were further challenges identified.22,33 One study found a self-harm screening tool for young people to be too formal and a barrier to effective listening.25
Service provision
The current shortage of alternative self-harm and support services is a barrier to effective GP management. Shortages in funding, patient liaison and community services, in-practice self-harm services, and counsellors who speak minority languages were all identified as barriers to GP management.25,29,30 One study identified a lack of support for suicide risk assessment in primary care.22
Local factors
Local factors were identified that negatively influenced GP management of self-harm. The long waiting times to receive letters from CAMHS were highlighted.29 A lack of written self-harm practice policies was also recognised as a barrier.30 In rural settings, there were concerns over maintaining patient confidentiality as well as over inadequate follow-up and communication on risk, treatment, and discharge plans from mental health services.32 Two studies mentioned the involvement of parents or carers as being potential barriers to the open discussion of self-harm with young people in the consultation.25,28
Systemic factors
Systemic factors hindered GPs’ ability to effectively manage patients who self-harm. A heavy workload for GPs was seen as a barrier to thorough suicide risk assessment.28 Demographic boundaries were considered to interfere with GP referral pathways to mental health services.29 One study cited a lack of out-of-hours patient record access and limited access to mental health services as obstacles to GP management.32 The same study mentioned GPs’ inability to choose which mental health professional to refer to as a further barrier.32
Consultation outcomes
Admission
GPs admit patients who have self-harmed to hospital, although the severity of self-harm in those admitted is unknown. Three studies reported on GPs admitting patients who have self-harmed to hospital, ranging from 60% (128/212) to 80% (244/305) of patients who had attempted suicide.24,27,31
Referral
GPs refer to counselling and secondary care services. GPs referred 19% (58/305) of patients who self-harm for ambulatory care follow-up.24 One study identified a GP referring patients to specialist services for suicide risk assessment.22 Three studies reported GP referrals made to mental health services: 15% (31/211) in Crawford and Wessely23 and 30% (64/212) in Fitzsimons et al.25,27 Two studies mentioned referrals to counselling services.23,27
Follow-up
Patients who self-harm are followed up in general practice. In Fitzsimons et al, 7% (14/212) were followed up in general practice.27 In young people, GPs provided regular follow-up.25 Patients perceived to be at greater risk of repeat self-harm were more likely to have self-harm documented in their records.23
Management
GPs undertake psychosocial interventions and prescribe medication for patients who self-harm. Two studies outlined GPs conducting psychosocial interventions in the consultation, which 26% (55/211) of GPs did in Crawford and Wessely.23,25 New or repeat psychotropic medication were prescribed to 9% (18/211) of patients.23 Where self-harm was documented in patient records, 75% (42/56) received an intervention.23
Duration of consultation
No studies reported on GP consultation duration.
Training needs
Clinician expressed
Primary care doctors want varied, continual CPD with a focus on consultations with young people. Three studies reported GPs stating a need for ongoing CPD with practical information in various formats (online, small groups, face-to-face, and tutor).25,27,29 Three studies described training needed for managing young people on involving guardians in consultations, maintaining confidentiality, communication, self-harm risk factors, and managing challenging consultations.25,28,33
Author inferred
Study authors relay a need for training on the management of patients with self-harm behaviour within a general practice context. One study stated that accessible and enhanced training is needed on the assessment and management of self-harm, incorporating GP experience and the role of general practice in suicide prevention.22 There were concerns about low identification of self-harm in patients aged 11–14 years and a push for training on managing young people.25 Michail and Tait argue for a taught, co-produced, holistic approach to suicide risk assessment in young people.28 Taliaferro et al 33 recommended training on psychosocial assessment and methods of reducing self-harm behaviour in young people.
DISCUSSION
Summary
GPs recognise self-harm as a serious risk for suicide, and assessing and treating patients who self-harm as their responsibility, but some feel unprepared. The lack of available self-harm training is a cause for concern given that self-harm is generally managed in primary care. The challenging nature of managing self-harm is especially apparent in young people, but GPs nonetheless see themselves as frontline support for young people who self-harm.
Five facilitating themes were identified that if addressed would enable more effective GP management: GP training, improved communication, service provision, clinical guidelines, and young people. Four themes on barriers arose: assessment, service provision, local factors, and systemic factors.
GP consultation outcomes with patients who self-harm include patient admission to hospital, referral to counselling or secondary care services, follow-up in general practice, and GPs conducting psychosocial interventions and/or prescribing psychotropic medication. GP self-harm training must be varied, include managing young people, and be relevant to the primary care context.
The role of the GP in the management of patients with self-harm behaviour is multifaceted and flexible across the patient journey, and includes providing frontline assessment and treatment; referral to specialist care; and ongoing support in primary care.
Strengths and limitations
This is the first systematic review exploring the role of the GP in managing patients who self-harm. The review methodology was consistent with established standards (PRISMA) for review processes of study selection, data extraction, and quality appraisal piloted by the review team and conducted independently by two authors.17 The narrative synthesis approach allowed for inclusion of both quantitative and qualitative data.21 A broad search strategy was implemented to achieve high search sensitivity.34
A limitation of narrative synthesis is that without a critically reflexive approach to the synthesis process there exists a possibility of biased and inaccurate conclusions.21 This was addressed by reflecting on the quality of evidence included and by predefining terms prior to data extraction. Two PhD theses were excluded during the selection process because of resource capacity and difficulties in obtaining them, thus increasing risk of selection bias.35 Four studies that utilised survey methodology recruited small samples, and their results may not be representative of all eligible GPs.26,27,30,33
No data on GP consultation duration were found in included studies; however, GPs reported a lack of time as a significant barrier in the management of self-harm.22,25,29 Two studies stated GP age range in England as beginning at 20 and 25.25,28 Neither age would represent the minimum age of a post-Certificate of Completion of Training GP in England, thus possibly affecting the validity of both study findings.36 Included studies were from Western countries and this review did not capture GP evidence from low- and middle-income countries.
Comparison with existing literature
An Australian qualitative study reported that GPs believed they had no significant role to play in the care of older adults (aged ≥80 years) who self-harm, felt hopeless when dealing with complex medical and social needs, and cited a lack of treatment options.37 This systematic review found that GPs were concerned over a lack of primary care self-harm services to support their management. Importantly, GPs believed that they were positive towards patients with self-harm taking responsibility to manage them, but sometimes reflected this responsibility onto the patient.25,26,31
GP training as part of suicide prevention programmes can improve clinician skills in the assessment and management of suicide risk, but the effect on reducing self-harm, repeat self-harm, and suicide is equivocal.38–40 The difficulty in distinguishing suicidal intent in self-harm is widely recognised; the NICE self-harm definition is irrespective of suicidal intent.10,22,41
GPs expressed uncertainty in establishing self-harm risk.28 The authors are not aware of effective general practice methods to predict or assess self-harm and therefore feel that this uncertainty is appropriate. The prediction of self-harm using self-harm risk scales in emergency departments is poor and not cost-effective.42,43
Implications for research and practice
This review highlights the lack of evidence on the GP role in self-harm management. The authors believe that the role of the GP is multidimensional, but characterised by time constraints.22,25,28,29 Future research should examine how patients who self-harm impact on GP consultation duration and understand how GPs can maximise the potential of the general practice consultation to support patients who self-harm.44
Obtaining the in-depth views of patients and mental health colleagues is important to further explore the role of the GP. The authors present the role of the GP as being grounded in current primary care but recognise that the role of the GP will be refined and developed over time.14
The GP is positioned to support early identification and intervention in patients who self-harm, and therefore the development and testing of effective, brief, GP-delivered self-harm interventions to reduce self-harm is urgently needed, and could potentially reduce admission and referral rates to secondary care.22,23,25,27 At present, there are no effective GP-delivered self-harm interventions.40 Developing these would also meet one of the key aims of the National Suicide Prevention Strategy.13
This review identifies an urgent need for acceptable, ongoing, and holistic training for GPs managing patients who self-harm to improve their knowledge and confidence in management, particularly in communication with young people, which must be continually evaluated and cost-effective.22,28 The recent self-harm and suicide prevention competence framework may aid in developing appropriate general practice training.45 The development of self-harm clinical guidelines and practice policies should be specific to general practice, and co-produced with primary care staff, patients, and the public.29,30,33,46
Primary care networks should incorporate these guidelines and policies into wider suicide prevention strategies and pilot and evaluate, in partnership with relevant third-sector organisations, integrated evidence-informed primary care self-harm models and services.13,14,47 For GPs to assess, treat, refer, and support patients who self-harm in primary care, improved communication on patient management with secondary care services, the development of brief and effective GP-led interventions, and the integration of evidence-based primary care self-harm models are all fundamental.
Acknowledgments
The authors thank Buddhika Fernando and Nadia Samuelsson for assistance in translation of studies and the study authors who responded to individual data requests. Thanks go to Jennie Popay and colleagues for their guidance on the conduct of narrative synthesis in systematic reviews.
Notes
Funding
This manuscript presents independent research supported by Faraz Mughal’s National Institute for Health Research (NIHR) In-Practice Fellowship (ref: IPF-2017-11-002). M Isabela Troya was funded by a Keele University ACORN studentship. Lisa Dikomitis was awarded a Senior Fellowship by the Higher Education Academy. Carolyn A Chew-Graham is part-funded by West Midlands Collaboration for Leadership in Applied Health Research and Care. The views expressed in this paper are those of the authors and not necessarily those of the NHS, NIHR, or the Department of Health and Social Care.
Ethical approval
Ethical approval was not sought; however, this study adheres to the ethical standards set by the Declaration of Helsinki.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
Faraz Mughal is the RCGP Clinical Fellow in Mental Health, Clinical Innovation and Research Centre, RCGP, and has authored RCGP TopTips for GPs on self-harm and suicide in young people. Carolyn A Chew-Graham is chair of the RCGP Scientific Foundation Board and RCGP Curriculum Advisor, Mental Health; and Chair of the Society for Academic Primary Care. All other authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received June 4, 2019.
- Revision requested August 1, 2019.
- Accepted August 16, 2019.
- © British Journal of General Practice 2020
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

