


Abstract
Background Pre-existing concurrent medical conditions (multimorbidity) complicate cancer diagnosis when they provide plausible diagnostic alternatives for cancer symptoms.
Aim To investigate associations in bladder cancer between: first, pre-existing condition count and advanced-stage diagnosis; and, second, comorbidities that share symptoms with bladder cancer and advanced-stage diagnosis.
Design and setting This observational UK cohort study was set in the Clinical Practice Research Datalink with Public Health England National Cancer Registration and Analysis Service linkage.
Method Included participants were aged ≥40 years with an incident diagnosis of bladder cancer between 1 January 2000 and 31 December 2015, and primary care records of attendance for haematuria, dysuria, or abdominal mass in the year before diagnosis. Stage at diagnosis (stage 1 or 2 versus stage 3 or 4) was the outcome variable. Putative explanatory variables using logistic regression were examined, including patient-level count of pre-existing conditions and ‘alternative-explanations’, indicating whether pre-existing condition(s) were plausible diagnostic alternatives for the index cancer symptom.
Results In total, 1468 patients (76.4% male) were studied, of which 399 (35.6%) males and 217 (62.5%) females had alternative explanations for their index cancer symptom, the most common being urinary tract infection with haematuria. Females were more likely than males to be diagnosed with advanced-stage cancer (adjusted odds ratio [aOR] 1.62; 95% confidence interval [CI] = 1.20 to 2.18; P = 0.001). Alternative explanations were strongly associated with advanced-stage diagnosis in both sexes (aOR 1.69; 95% CI = 1.20 to 2.39; P = 0.003).
Conclusion Alternative explanations were associated with advanced-stage diagnosis of bladder cancer. Females were more likely than males to be diagnosed with advanced-stage disease, but the effect was not driven entirely by alternative explanations.
INTRODUCTION
Bladder cancer is a significant global health burden. It is the 10th most common cancer in the UK and worldwide, with the highest incidence rates in males and older people.1,2 Bladder cancer is the ninth most common cause of cancer death in the UK1 and the 15th worldwide.2 Early-stage diagnosis of cancer is associated with improved survival.3 Identifying and understanding barriers to early-stage diagnosis of bladder cancer remain an important focus for research, clinical practice, and cancer policy.
Sex disparities in bladder cancer diagnosis and outcomes are well documented. Although females have a lower bladder cancer incidence compared with males, overall they present with more advanced disease and a have worse survival rate.4–7 Of all the cancer types, bladder cancer has the largest sex difference in 1-year survival rate.3 Compared with males, females are approximately 25% more likely to experience a delay in bladder cancer diagnosis of >9 months after presentation with haematuria.8 Additionally, females have ≥3 pre-referral consultations in primary care more often than males.9
Multimorbidity, that is, the presence of ≥2 concurrent medical conditions, may present a barrier to early-stage cancer diagnosis, including bladder cancer. Multimorbidity is highly prevalent in older people, who also have the highest incidence of bladder cancer.10 Multimorbidity has been associated with advanced-stage breast cancer diagnosis, acting through a number of mechanisms, including the competing-demand and alternative-explanations hypotheses.11 In the competing-demands hypothesis, early symptoms of cancer may be overlooked by physicians or patients because the management of comorbid diseases diverts attention and resources away from the diagnosis of cancer. In the alternative-explanations hypothesis, existing conditions that provide a plausible diagnostic alternative for the presenting cancer symptom may delay investigation and subsequent diagnosis of cancer. The role of multimorbidity, and the competing-demands and alternative-explanations hypotheses in bladder cancer diagnosis remain poorly investigated. Further, most studies of the relationship between multimorbidity and cancer diagnosis examine the time to diagnosis rather than stage at diagnosis. The latter is more directly related to survival, so is preferable.
The aims of this study were: to assess whether having ≥1 comorbid conditions is associated with more advanced stage of bladder cancer at diagnosis; and test the ‘alternative-explanations’ hypothesis,12 to see if it sheds light on the observed diagnostic delays experienced by females.
METHOD
Data source
This population-based, observational study was set in the Clinical Practice Research Datalink (CPRD) GOLD database with linkage to Public Health England National Cancer Registration and Analysis Service (NCRAS, Set 15) and Office for National Statistics data. NCRAS collects detailed information on >99% of all non-skin cancer tumours in England. Set 15 includes cancers diagnosed between January 1990 and December 2015, coded using the International Classification of Diseases, 10th revision (ICD-10).13
| Early-stage diagnosis of cancer is associated with improved outcomes, including survival. The impact of multimorbidity on the diagnostic process in symptomatic patients, and on the likelihood of early-stage diagnosis, is poorly understood. This research investigated if the condition count and the presence of conditions that share symptoms with bladder cancer are associated with advanced-stage bladder cancer diagnosis. The findings confirm that females are more likely than males to be diagnosed with advanced-stage bladder cancer. To the authors’ knowledge, this study is the first to show that pre-existing conditions providing plausible diagnostic alternatives for bladder cancer symptoms (notably urinary tract infections) are associated with advanced-stage bladder cancer diagnosis. Alternative explanations do not account for the poorer outcomes for females compared with males. In line with the 2015 National Institute for Health and Care Excellence suspected cancer referral guidelines, it is recommended that clinicians consider undiagnosed bladder cancer in patients aged ≥40 years with visible haematuria, dysuria, abdominal mass, or urinary tract infection. |
How this fits in
The CPRD is the largest database of anonymised, longitudinal electronic medical records from primary care in the world.14 CPRD GOLD contains data collected as part of routine clinical care in general practices in the UK. In 2013, data linkage between the CPRD and NCRAS was enabled for 404 practices, representing approximately 75% of English practices and 58% of UK practices in the CPRD.
Patient inclusion criteria
Patient inclusion criteria were as follows:
an incident bladder cancer code (any ICD-10 code commencing C67, denoting malignant neoplasm of the bladder) in NCRAS between 1 January 2000 and 31 December 2015, with stage at diagnosis;
a minimum of 1 year of CPRD records, containing ≥1 consultations preceding the cancer diagnosis and presenting with ≥1 possible symptoms of bladder cancer, using National Institute for Health and Care Excellence (NICE) guidelines.15,16 GPs have no opportunity to be involved in patients’ cancer diagnosis if the patient does not consult or is asymptomatic; and,
aged ≥40 years on diagnosis.
Bladder cancer symptoms
Four symptoms of bladder cancer were selected: haematuria (visible or non-visible), dysuria, and abdominal mass.15,16 Libraries of Read codes that might be used by GPs to record these symptoms were collated using robust methods.17 Symptomatic patients were identified by the presence of any of these codes in their records. Symptoms presented >1 year before diagnosis are not reliably more common in people who are subsequently diagnosed with cancer compared with controls; therefore, searches were constrained to 1 year before diagnosis.18 The earliest recorded symptom(s) of bladder cancer was identified, and denoted the index date.
Comorbidity
The authors identified whether patients had comorbid medical conditions before their index date. The choice of conditions was made by two medical students in the research group and one experienced GP from the group. Criteria for condition selection included reliability of recording or sharing symptoms with bladder cancer:
conditions that are part of the Quality and Outcomes Framework (QOF), the pay-for-performance scheme in the UK.19 QOF conditions are well defined, and, being linked to practice payments, recording is likely to be good. The following QOF conditions were selected: asthma, atrial fibrillation, chronic obstructive pulmonary disease, coronary heart disease, dementia, depression, diabetes mellitus, epilepsy, heart failure, hypertension, and stroke. Anxiety was also included because it has been linked to increased time to cancer diagnosis in previous work; and,12,20
conditions that share the following symptoms with bladder cancer:
—haematuria and dysuria: urinary tract infection, sexually transmitted disease, kidney disease, urinary tuberculosis, sickle cell disease, nephrolithiasis, prostatitis, menorrhagia (presumably misattributed haematuria), endometriosis, and benign prostatic hyperplasia; and,
—abdominal mass: uterine fibroids, aortic aneurysm, and retention.
Libraries of Read codes for the above conditions were collated,17 and patients with these conditions were identified.
Two patient-level variables were created: the patient’s pre-existing conditions count; and the ‘alternative-explanations’ variable, identifying whether the patient had a history of a comorbid condition that could provide an alternative explanation for their index symptom of bladder cancer.
Stage at diagnosis
Stage at diagnosis was provided by NCRAS. Stage was categorised as ‘early’ (stages 1 or 2) or ‘advanced’ (stages 3 or 4) for the regression analyses.
Patient characteristics
Patient sex was obtained from the patient file provided by CPRD GOLD. Patient age at diagnosis was estimated, assuming that the patient was born on 1 July of their year of birth, provided by CPRD GOLD. Patient-level deprivation was estimated using the Townsend Score as a quintile score of 1 (least deprived) to 5 (most deprived) by linked Office for National Statistics data.
Data analysis
Simple descriptive statistics were used for demographic data. Associations between stage of cancer at diagnosis, ordinal condition count, and binary ‘alternative-explanations’ variables were analysed using logistic regression. The analyses were adjusted for age at diagnosis, sex, and deprivation. Interaction terms were sought on clinical grounds between sex and: count of pre-existing conditions; and presence of an alternative explanation. Post-estimation diagnostics tested for model specification (linktest), goodness of fit (lfit), and collinearity between explanatory variables (collin). All analyses used Stata/SE (version 16).
Missing data
Both the CPRD and NCRAS have some missing data. Data may be missing in the CPRD because they were not reported by the patient, or not recorded by the GP using a Read code. In line with standard practice, the absence of a Read code for a symptom was interpreted as an absence of the symptom itself.14 The authors acknowledge from previous experience that this is likely to result in an underestimation of people with symptoms of bladder cancer.21
NCRAS introduced a change in reporting standards in 2012 affecting the consistency of data collection and quality across the study period. Logistic regression was used to check for any associations between ‘missing stage’ and the explanatory variables.
Power calculation
A sample of 1468 people has 99% power to detect a 10-point increase in percentage of advanced-stage diagnoses in the group with alternative explanations for their first symptom of cancer compared with those without, that is, a change from 20% to 30%. This was based on 42% of the sample having an alternative explanation for their cancer symptom12 and a baseline of 20% of patients being diagnosed with advanced-stage disease.1
Sensitivity analyses
Urinary tract infection, although an alternative explanation for haematuria and dysuria, is also listed in the NICE suspected cancer referral guidelines as a possible feature of undiagnosed bladder cancer warranting investigation.15 Two sensitivity analyses were carried out, with results reported in Supplementary Tables S2 and S3. First, separate effects of alternative explanations for bladder cancer symptoms were sought between those with and without urinary tract infection. The second sensitivity analysis excluded participants who presented with urinary tract infection in the 6 months before the bladder cancer diagnosis.
RESULTS
Study participants
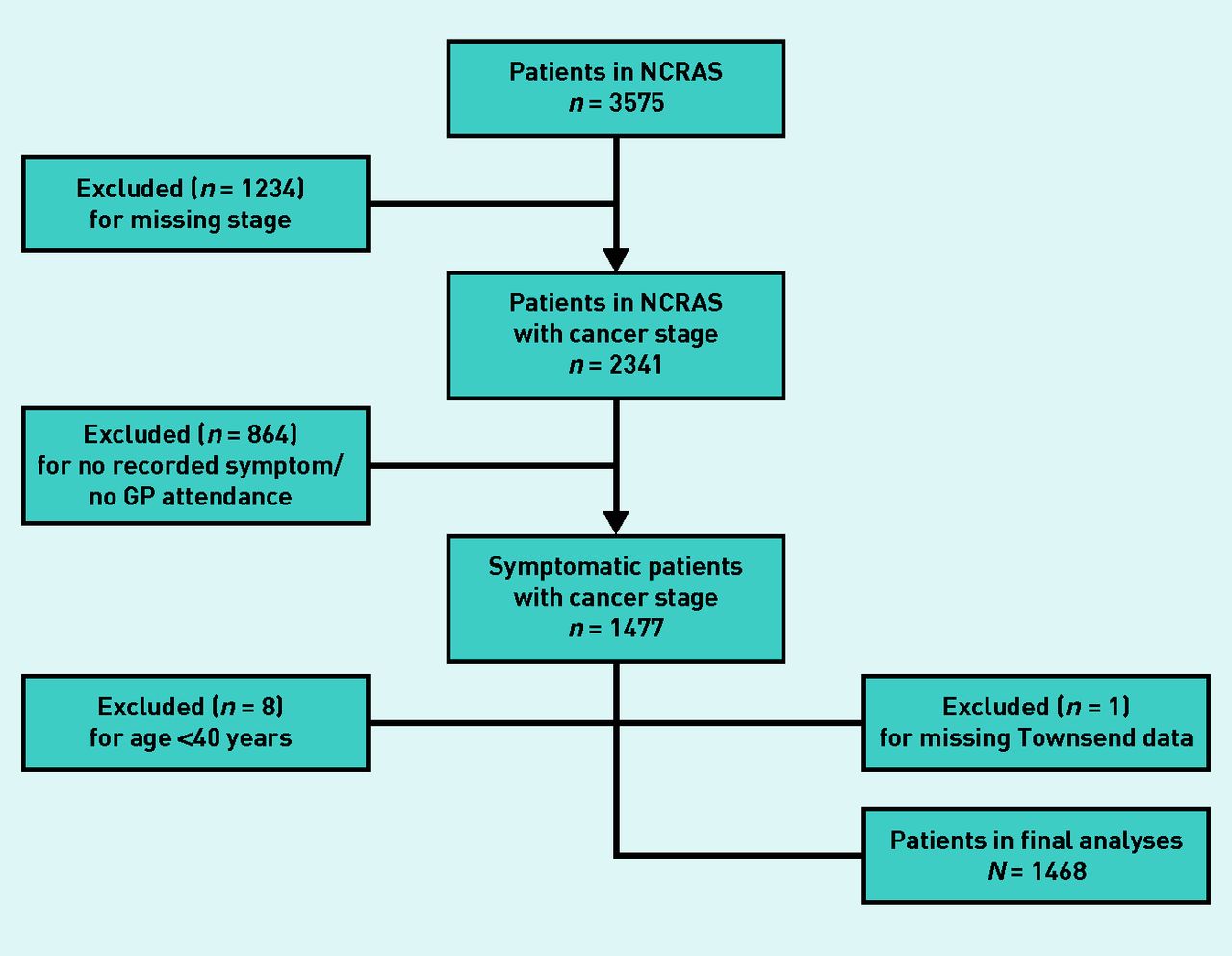
The CPRD and NCRAS searches identified 3575 adults (n = 2606 males,n = 969 females) diagnosed with bladder cancer between 1 January 2000 and 31 December 2015. Of these, 2107 were excluded from the analyses for the reasons given in Figure 1. The distribution of participants by year of diagnosis varied, rising from 184 (12.5%) in 2000–2003, peaking in 2008–2011 (520, 35.4%), and reducing to 386 (26.3%) in 2012–2015. Levels of missing staging data reduced considerably over time (Table 1).

{kind=link}
Application of exclusion criteria. NCRAS = National Cancer Registration and Analysis Service.
Patient characteristics
The final analyses included 1468 (n = 1121 males, n = 347 females) symptomatic adults aged ≥40 years with known stage of bladder cancer. The mean age at diagnosis was 72.9 years (95% confidence interval [CI] = 72.4 to 73.5) and 74.7 years (95% CI = 73.6 to 75.8) for males and females, respectively. Patient characteristics by cancer stage are shown in Table 1.
Index symptoms of cancer
The majority of patients (n = 1459/1468, 99.4%) had a single index symptom of bladder cancer recorded in the year before diagnosis. The most common bladder cancer symptom was visible haematuria (n = 954/1121, 85.1% of males; n = 275/347, 79.3% of females), followed by dysuria (n = 120/1121, 10.7% of males; n = 57/347, 16.4% of females). Index symptoms of non-visible haematuria (n = 44/1121, 3.9% of males; n = 11/347, 3.2% of females) and abdominal mass (n = 3/1121, 0.3% of males; n = 4/347, 1.2% of females) were infrequent. The nine patients with two index symptoms of bladder cancer had haematuria and dysuria (data not shown).
Comorbid conditions
The majority (n = 1178/1468, 80.2%) of patients had been diagnosed with ≥1 comorbid condition before their index symptom of bladder cancer (Table 1). Of the QOF conditions (Table 2), by far the most common in both sexes was hypertension (n = 451/1121, 40.2% of males; n = 166/347, 47.8% of females). Depression and/or anxiety was more common in females (n = 115/347, 33.1%) than in males (n = 205/1121, 18.3%). The comorbid conditions provided alternative explanations for the first possible symptom of bladder cancer for 616 of 1468 (42.0%) patients overall (Table 1). This was more likely for females (n = 217/347, 62.5%) than for males (n = 399/1121, 35.6%) (data not shown). Of the conditions that presented with haematuria and dysuria, the most common was urinary tract infection, which was diagnosed in a greater proportion of females (n = 170/347, 49.0%) than in males (n = 193/1121, 17.2%). A small proportion (n = 98/1468, 6.7%) of patients had conditions presenting with abdominal mass (Table 2).
Comorbid conditions diagnosed before the first possible symptom of bladder cancer
Some of the comorbid conditions sharing symptoms with bladder cancer were sex-specific; namely, conditions of the prostate are only experienced by males, whereas menorrhagia, endometriosis, and uterine fibroids are specific to females. Similar proportions of males (n = 160/1121, 14.3%) and females (n = 58/347, 16.7%) had sex-specific comorbidities.
Stage at diagnosis
Bladder cancer was diagnosed at an early stage in 1199 of the 1468 patients (81.7%) and at an advanced stage in the remaining 269 (18.3%), with no gross fluctuation over time (Table 1). A greater proportion of females experienced advanced-stage (n = 87/347, 25.1%) than early-stage (n = 260/347, 74.9%) disease. The proportion of people with ≥1 comorbid condition was similar in the groups with early-stage (n = 960/1199, 80.1%) and with advanced-stage (n = 218/269, 81.0%) disease. The proportion of people with an alternative explanation for their index bladder cancer symptom was higher in the group diagnosed with advanced-stage cancer (n = 134/269, 49.8%) than in those with early-stage disease (n = 482/1199, 40.2%) (Table 1).
Regression analyses
Females were more likely to be diagnosed with advanced-stage cancer than males (adjusted odds ratio [aOR] 1.62; 95% CI = 1.20 to 2.18; P = 0.001) (Table 3). Alternative explanations for the first possible symptom of bladder cancer were strongly associated with advanced-stage diagnosis (aOR 1.69; 95% CI = 1.20 to 2.39; P = 0.003).
Association between stage of bladder cancer diagnosis, multimorbidity, and alternative explanations for cancer symptoms; adjusted for age, sex, and deprivation
The interaction term between sex and alternative explanations was not statistically significant (see Supplementary Table S1). Post-estimation regression diagnostics suggested no problems of model specification, goodness of fit, or collinearity between explanatory variables.
A logistic regression analysis comparing patients with and without complete staging information indicated that missingness was random with regard to all explanatory variables.
Sensitivity analyses
Only alternative explanations provided by urinary tract infections (n = 363/616, 58.9%) were strongly associated with advanced-stage diagnosis (aOR 2.02; 95% CI = 1.39 to 2.94; P<0.0001) (see Supplementary Table S2).
Associations with advanced-stage diagnosis for sex (aOR 1.37; 95% CI = 0.98 to 1.93; P = 0.068) and alternative explanations (aOR 1.43; 95% CI = 0.98 to 2.08; P = 0.062) were weakened when the authors excluded the 132 of 363 (36.4%) urinary tract infections occurring in the 6 months before participants were diagnosed with bladder cancer (see Supplementary Table S3).
DISCUSSION
Summary
Having comorbid conditions that offered plausible diagnostic alternatives for the symptoms of bladder cancer increased the odds of being diagnosed with advanced-stage disease (aOR 1.69; 95% CI = 1.20 to 2.39; P = 0.003).
This effect was the same in males and females, and is unlikely to account for the observation that females are more likely than males to be diagnosed with advanced-stage bladder cancer (aOR 1.62; 95% CI = 1.20 to 2.18; P = 0.001).
Sensitivity analysis indicated that the effect of alternative explanations was carried by urinary tract infections, which are a classical alternative explanation when bladder cancer is present. Some of these may be misdiagnoses, and others true urinary tract infections as a complication of the cancer.
The sensitivity analyses of removing patients whose urinary tract infections only occurred in the final 6 months before diagnosis suggests that this pattern exists and that it has consequences for some of these patients (mostly females), who have a worse stage at diagnosis as a result.
Strengths and limitations
A real strength of this study was its setting in primary care, where GPs face the difficult clinical problem of recognising possible cancer symptoms but which could be plausibly explained by a patient’s existing medical conditions. The CPRD is the largest database of longitudinal primary care records in the world and is recognised for its high-quality data.14 Robust methods for case identification in the CPRD were used17 and cancer diagnoses were validated by NCRAS.
Despite this, the use of CPRD and NCRAS data has some limitations. Primary care doctors may record information in free-text fields, which are not included in CPRD research data.22 Based on previous studies of data loss in text fields, the authors anticipated that they identified 80% of the true numbers of people with visible haematuria.21,23
Further limitations included the amount of missing staging data: of the present original sample of 3575 patients, 1234 (34.5%) were missing staging data and so were excluded from the analyses. Stage completeness improved dramatically in 2011–2015, so it could not be assumed that staging data before this were missing at random. The authors had considered restricting the sample to 2011–2015, but the sample number would have been too low (n = 368), partly because of the reducing size of the CPRD in this period (Price et al, unpublished data, 2020). It was reassuring that there was no evidence of an association between missing staging data and any of the explanatory variables in the analyses.
Comparison with existing literature
To the authors’ knowledge, this is the first study to investigate the impact of comorbid conditions that provide a plausible explanation for the symptoms of bladder cancer on stage of diagnosis.
The present findings are consistent with Gurney and colleagues’ study, which reported that increasing comorbidity index was not associated with increased odds of late-stage diagnosis of urological cancers.24 These authors did not explore the alternative-explanations hypothesis.
The findings presented here further confirm an evidence synthesis of seven studies reporting that females are more likely than males to have advanced tumours at the time of diagnosis,4 and are at greater risk of emergency presentation.25 Possible explanations for the poorer outcomes in females include the observed delay in their referral and poor recognition of their urinary symptoms.7,9 The authors deliberately sought, but did not find, any evidence that the presence of alternative explanations for the index bladder cancer symptom might account for the poorer outcomes in females than males.
The sensitivity analyses findings are consistent with the possibility that patients who present with urinary tract infection have a particularly aggressive type of bladder cancer; hence, the association with advanced-stage diagnosis. The prognosis for bladder cancer is known to be worse for patients who do not present with alarm symptoms, compared with those who do.26 In the present study, the alternative explanations were paired between urinary tract infection and the alarm symptom, haematuria. Therefore, the authors consider their findings more likely to represent the scenario of delayed investigation for possible cancer where plausible diagnostic alternatives for the symptoms of cancer exist.9
Implications for research and practice
The present findings suggest that the presence of conditions that provide plausible diagnostic alternatives for bladder cancer symptoms are associated with diagnostic delay, and increase the risk of advanced-stage disease, in males and in females. It is important to note that this is an association, not evidence of misdiagnosis.
In line with the 2015 NICE suspected cancer referral guidelines, the authors recommend that clinicians retain the possibility of undiagnosed bladder cancer in patients aged ≥40 years with visible haematuria, dysuria, or abdominal mass. Studies could investigate the optimal period of ‘watchful waiting’ for morbid patients with haematuria and urinary tract infection that minimises the risk of advanced-stage bladder cancer diagnosis. Furthermore, if associations with non-investigation of possible bladder cancer despite symptoms can be identified, then interventions to help reduce advanced-stage diagnosis can be designed and tested.
Notes
Funding
This work was supported by Madeline Carney’s grant from the University of South Florida (USF) Health Morsani College of Medicine, Research, Innovation and Scholarly Endeavors. The dataset had been used for a separate study on time to diagnosis for many cancers funded by Cancer Research UK (CRUK) (grant reference number: 21550). Sarah Price was funded by the National Institute for Health Research (NIHR) Policy Research Programme, conducted through the Policy Research Unit in Cancer Awareness, Screening and Early Diagnosis Unit. The views expressed are those of the author(s) and not necessarily those of the NIHR, the Department of Health and Social Care, CRUK, NHS, or other government departments or arm’s length bodies. This research is also linked to the CanTest Collaborative, which is funded by CRUK (grant reference number: C8640/A23385), of which Willie Hamilton is Co-Director.
Ethical approval
This study was approved by an Independent Scientific Advisory Committee (protocol: 16_037) and the USF Institutional Review Board (protocol: 00034170).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
Willie Hamilton was clinical lead on the 2015 revision of the National Institute for Health and Care Excellence (NICE) guidance on investigation of suspected cancer, whose contribution to this article was in a personal capacity and does not represent the view of the Guideline Development Group, or of the NICE itself. All remaining authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received November 15, 2019.
- Revision requested February 2, 2020.
- Accepted February 25, 2020.
- ©The Authors
This article is Open Access: CC BY 4.0 licence (http://creativecommons.org/licences/by-nc/4.0/).
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

