


Abstract
Background C-reactive protein (CRP) point-of-care testing can reduce antibiotic use in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) in primary care, without compromising patient care. Further safe reductions may be possible.
Aim To investigate the associations between presenting features and antibiotic prescribing in patients with AECOPD in primary care.
Design and setting Secondary analysis of a randomised controlled trial of participants presenting with AECOPD in primary care (the PACE trial).
Method Clinicians collected participants’ demographic features, comorbid illnesses, clinical signs, and symptoms. Antibiotic prescribing decisions were made after participants were randomised to receive a point-of-care CRP measurement or usual care. Multivariable regression models were fitted to explore the association between patient and clinical features and antibiotic prescribing, and extended to further explore any interactions with CRP measurement category (CRP not measured, CRP <20 mg/l, or CRP ≥20 mg/l).
Results A total of 649 participants from 86 general practices across England and Wales were included. Odds of antibiotic prescribing were higher in the presence of clinician-recorded crackles (adjusted odds ratio [AOR] = 5.22, 95% confidence interval [CI] = 3.24 to 8.41), wheeze (AOR = 1.64, 95% CI = 1.07 to 2.52), diminished vesicular breathing (AOR = 2.95, 95% CI = 1.70 to 5.10), or clinician-reported evidence of consolidation (AOR = 34.40, 95% CI = 2.84 to 417.27). Increased age was associated with lower odds of antibiotic prescribing (AOR per additional year increase = 0.98, 95% CI = 0.95 to 1.00), as was the presence of heart failure (AOR = 0.32, 95% CI = 0.12 to 0.85).
Conclusion Several demographic features and clinical signs and symptoms are associated with antibiotic prescribing in AECOPD. Diagnostic and prognostic value of these features may help identify further safe reductions.
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) affects around 2% of the UK population, and is the third leading cause of death globally.1–3 More than 70% of patients presenting with acute exacerbations of COPD (AECOPD) in primary care are prescribed an antibiotic,4 despite bacterial pathogens only being detectable in 20%–50% of exacerbations.5–7 Antibiotic use for AECOPD accounts for 7.5% of all primary care antibiotic prescriptions.8
Overuse of antibiotics contributes to the development of antimicrobial resistance, exposes patients to the risk of unnecessary side effects, wastes money, and undermines self-care.9 There is, therefore, a need for antimicrobial stewardship initiatives to target the prescribing of antibiotics for patients with AECOPD in primary care.
The PACE trial demonstrated that a management strategy involving the use of C-reactive protein (CRP) point-of-care testing (POCT) for patients with AECOPD in primary care can lead to a reduction in antibiotic use without any evidence of patient harm.10 In this randomised controlled trial, antibiotics were used by 77% of patients in the usual-care group compared with 57% in the CRP-POCT group (a relative difference of 26%), while potential bacterial pathogens were isolated in the sputum of only 44% of participants. This suggests that there may be potential for further reductions in antibiotic prescribing, and it is therefore important to understand the determinants of antibiotic prescribing for this condition.
The aim of this study was to examine the presenting features associated with antibiotic prescribing decisions for AECOPD in primary care, and to explore if these were different when clinicians had access to a CRP measurement (available for patients randomised to the intervention arm of the trial), and whether the CRP value was elevated (≥20 mg/l) or not.
| Overuse of antibiotics contributes to antimicrobial resistance, unnecessarily exposes patients to side effects, and undermines self-care. A recent randomised controlled trial demonstrated that, when clinical management is supplemented with a C-reactive protein (CRP) point-of-care test, antibiotics can be safely reduced in patients presenting in primary care with an acute exacerbation of chronic obstructive pulmonary disease (AECOPD). Further analysis, in the present study, found several demographic and clinical features associated with the prescribing of antibiotics to patients presenting with AECOPD in UK primary care, independent of the CRP test result. Studying the diagnostic and prognostic value of these features is warranted to understand how to safely reduce antibiotic use in this population. |
How this fits in
METHOD
Study design
This was a secondary analysis of an open, multi-site, parallel-group, individually randomised controlled trial that evaluated the effectiveness of a CRP-POCT management strategy for patients with an AECOPD in UK primary care (the PACE trial). Target recruitment was 650 participants. The protocol and findings for the original study are reported elsewhere.10–12
Participants and setting
Participants aged ≥40 years with a clinically recorded diagnosis of COPD (with or without spirometry confirmation) who presented with an acute exacerbation for 1–21 days were recruited into the trial from general practices across England and Wales. Full inclusion and exclusion criteria have been described previously.11
Procedures
After patients gave informed consent, their baseline data were collected. Participants were then randomly allocated using remote online computer randomisation (ratio 1:1) either to management via usual care (no CRP-POCT) or to CRP-POCT in addition to usual care.
All general practices (n= 86) were provided with a POCT device and all associated materials, information on current best practice for managing AECOPD, with no other specific guidance given to clinicians with regards to the management of their patients. Participants allocated to the usual-care arm were managed without the use of a CRP-POCT measurement. Those allocated to the CRP-POCT arm had a CRP measurement taken using a POCT desktop machine, to help guide initial antibiotic prescribing decisions. Clinicians received guidance and training on how to use the device and interpret the result. The guidance indicated that antibiotics were unlikely to be beneficial and should usually not be prescribed for patients with a CRP <20 mg/l; that antibiotics may be beneficial, especially if purulent sputum is present, for patients with a CRP 20–40 mg/l; and that antibiotics are likely to be beneficial and should usually be prescribed (unless a patient is assessed as being at low risk of complications) for patients with a CRP >40 mg/l. The CRP cut-offs were based on data from a placebo-controlled trial of antibiotics for patients with acute exacerbations of mild-to-moderate COPD.13
Clinicians recorded participants’ demographic details (age and sex), their medical history (presence of comorbidities and COPD stage according to Global Initiative for Chronic Obstructive Lung Disease [GOLD] criteria), and clinical features pertaining to their exacerbation: number of days experiencing symptoms, temperature, pulse rate, oxygen saturation, ability to complete a full sentence, tachypnoea, presence and number of Anthonisen symptoms (increased shortness of breath, increased sputum volume, and/or increased sputum purulence),14 presence of crackles, wheeze, diminished vesicular sounds, or evidence of consolidation on auscultation of the lungs. Clinicians recorded the colour of the sputum sample using a BronkoTest chart.15 Where a sputum sample could not be obtained, participants estimated their current sputum colour using the chart. Participants were also asked about their smoking status (nonsmoker, current smoker, or ex-smoker) during 1-week follow-up assessments.
Antibiotic prescribing and other management decisions were made and recorded after receipt of the test result for those allocated to the CRP-POCT arm.
Statistical methods
Descriptive statistics were reported as frequencies and percentages or means and standard deviations, as appropriate.
To investigate the association between patient and clinical features and antibiotic prescribing, multilevel multivariable logistic regression models were fitted, accounting for any clustering of participants in practices. Each explanatory variable (those described in the Procedures section) was included in separate regression models. Sputum colour was ranked 1 (lightest colour) to 5 (darkest colour). Continuous variables were grand-mean-centred and included as linear effects following the inspection of model parsimony, when comparing linear terms with restricted cubic splines with both five and three knots, using the Akaike information criterion (see Supplementary Table S1 for details). Each model was adjusted for CRP measurement (defined as no measurement taken, CRP <20 mg/l, and CRP ≥20 mg/l) in addition to increased sputum purulence. Sputum purulence was adjusted for as a potential confounder as it was an exacerbation feature specifically mentioned in the guidance on interpreting the CRP measurement. The differential association between explanatory variables and antibiotic prescribing by CRP measurement was explored by extending models to include CRP measurement interacted with explanatory variables.
The proportion of the total variance, for explanatory variable, that was attributable to differences across practices was expressed by estimating the intra-cluster correlation coefficient (ICC), with the π2/3 estimator used where considering a binary response. These were calculated to indicate practice (as a proxy for prescriber) variation in the reporting of these features.
Statistical analyses were conducted using Stata (version 16.0).
RESULTS
Participant flow
The PACE trial consented and randomised 653 participants from 86 general practices across England and Wales. Three participants withdrew their permission for their data to be used and one was randomised in error, leaving 649 participants: 324 were allocated to usual care and 325 to CRP-POCT. CRPPOCT data were not available for eight participants, leaving 241 allocated to CRPPOCT with a CRP value <20 mg/l, and 76 allocated to CRP-POCT with a CRP value ≥20 mg/l (Figure 1). See Supplementary Table S2 for details of descriptive statistics overall, by CRP measurement, and by antibiotic prescription receipt at the index consultation.
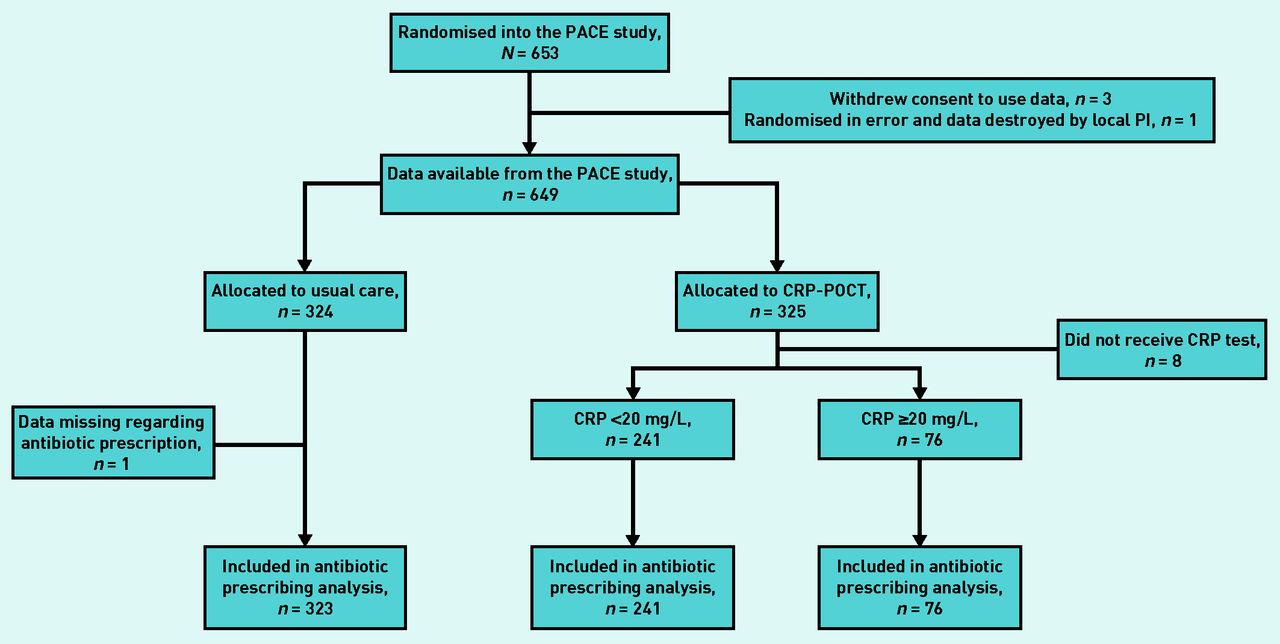
Participant flow diagram.
CRP = C-reactive protein. PI = principal investigator. POCT = point-of-care test.
Numbers analysed
One participant (CRP not measured) did not have data available regarding antibiotic prescribing decisions at the index consultation. Data availability varied for each of the candidate variables, and numbers of participants for each are given in Table 1. Antibiotics were prescribed at the index consultation to 225 (69.7%) participants in whom CRP was not measured, 79 (32.8%) with CRP <20 mg/l, and 68 (89.5%) with CRP ≥20 mg/l (see Supplementary Table S2 for details).
Associations between demographic features, comorbid illness, symptoms and signs, and antibiotic prescribing at the index consultation
Demographic features and comorbid illness
Higher participant age was associated with lower odds of antibiotic prescribing (adjusted odds ratio [AOR] per additional year increase = 0.98, 95% confidence interval [CI] = 0.95 to 1.00, P = 0.035) (Table 1). The presence of heart failure was associated with lower odds of antibiotic prescribing (AOR = 0.32, 95% CI = 0.12 to 0.85, P= 0.022). There was no evidence that the association between any of the patient characteristics and antibiotics were different by CRP measurement (see Supplementary Table S3 for details).
Practice-level ICCs for demographic features and comorbid illness ranged from 0.02 (95% CI = 0.00 to 0.17) for age to 0.13 (95% CI = 0.05 to 0.28) for the presence of at least one comorbid illness (see Supplementary Figure S1 for details).
Symptoms and signs
Clinician-reported chest auscultation findings of crackles (AOR = 5.22, 95% CI = 3.24 to 8.41, P<0.001), wheeze (AOR = 1.64, 95% CI = 1.07 to 2.52, P= 0.022), and diminished vesicular breathing (AOR = 2.95, 95% CI = 1.70 to 5.10, P<0.001), as well as clinician-reported evidence of consolidation (AOR = 34.40, 95% CI = 2.84 to 417.27, P = 0.005), were all associated with higher odds of antibiotic prescribing (Table 1). A greater number of participants in the high CRP group (59.2%) experienced crackles than did those in the low CRP group (44.0%) (see Supplementary Table S2).
ICCs for clinical features ranged from 0.02 (95% CI = 0.00 to 0.15) for pulse rate to 0.60 (95% CI = 0.32 to 0.81) for evidence of consolidation on auscultation of the lungs (see Supplementary Figure S2 for details).
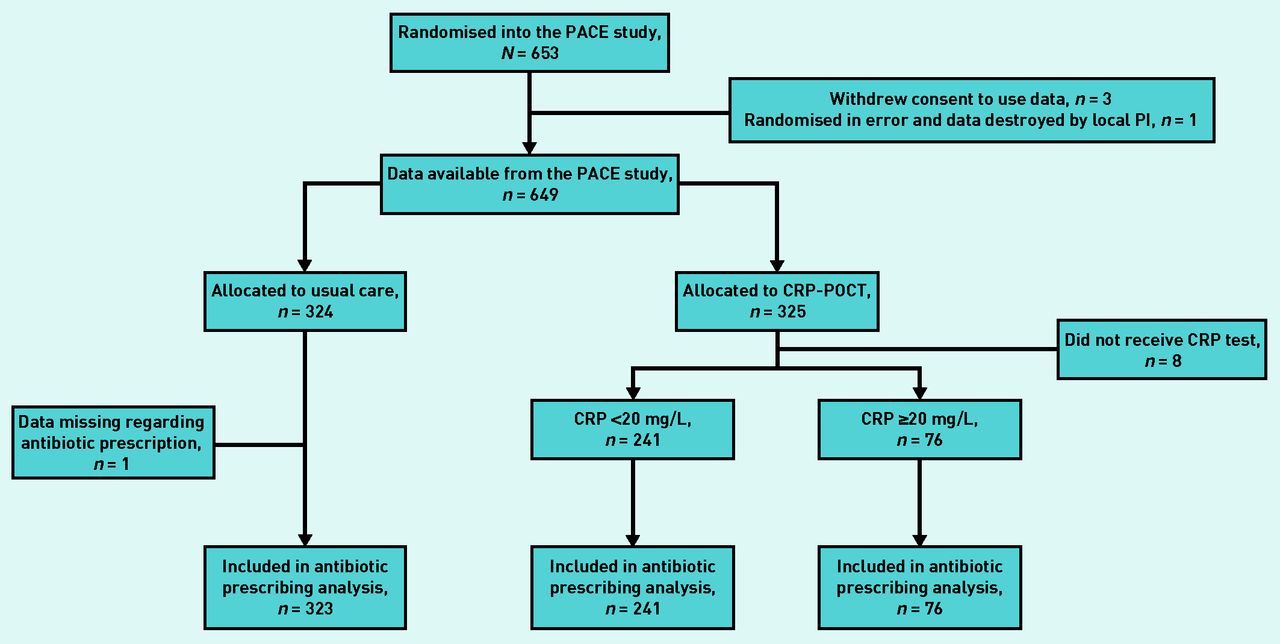
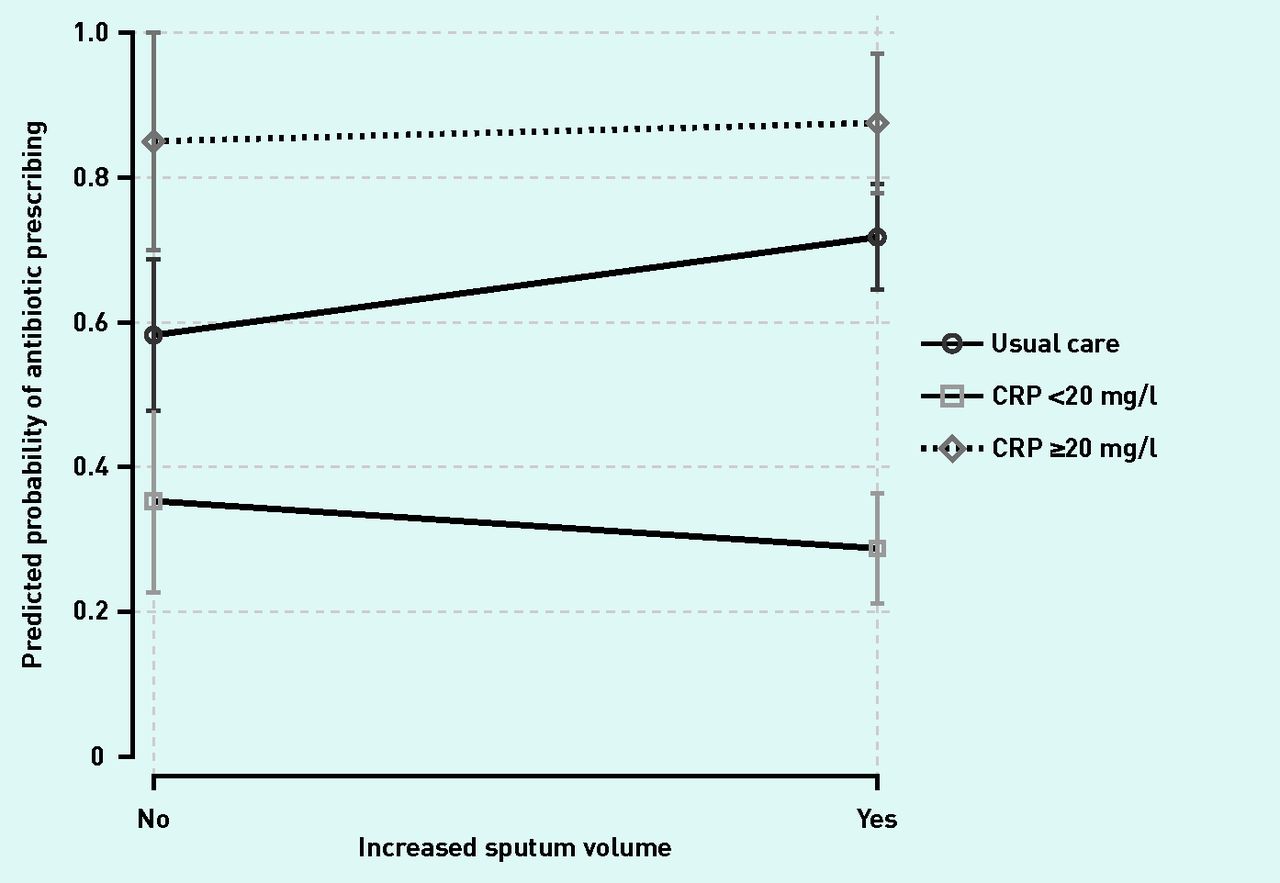
There was evidence to suggest a differential association between increased sputum volume and antibiotic prescribing by CRP measurement. Specifically, while an increase in sputum volume was associated with higher odds of antibiotic prescribing for participants in whom CRP was not measured (increased sputum volume main effect odds ratio [OR] = 2.18, 95% CI = 1.17 to 4.07; CRP <20 mg/l main effect = 0.30, 95% CI = 0.13 to 0.65; CRP ≥20 mg/l main effect: 5.88, 95% CI = 1.36 to 25.50) (see Supplementary Table S3 for details), there was minimal influence on antibiotic prescribing for those with CRP <20 mg/l (interaction between increased sputum volume and CRP <20 mg/l OR = 0.31, 95% CI = 0.12 to 0.80) (Figure 2). Evidence of consolidation was reported for 18 participants in total (seven in those for whom CRP was not measured, eight with CRP <20 mg/l, and three with CRP ≥20 mg/l). All but one of these participants (who had CRP <20 mg/l) were prescribed antibiotics at the index consultation (data not shown). The reporting of crackles was associated with the highest odds of antibiotic prescribing, and there was no evidence of a differential association by CRP measurement (Figure 3).

Differential association between increased sputum volume and antibiotic prescribing by CRP measurement. Vertical lines indicate 95% CIs.
CI = confidence interval. CRP = C-reactive protein.

{kind=link}
{kind=link}
{kind=link}
Differential association between reporting crackles on auscultation and antibiotic prescribing by CRP measurement. Vertical lines indicate 95% CIs.
CI = confidence interval. CRP = C-reactive protein.
DISCUSSION
Summary
This study investigated antibiotic prescribing associations for patients with AECOPD in UK primary care. It found that lower age, presence of heart failure, and clinician-reported abnormal findings on examination of the lungs (crackles, wheeze, diminished vesicular breathing, and evidence of consolidation) were all associated with antibiotic prescribing at the index consultation after adjusting for CRP measurement category and the presence of increased purulent sputum.
Increased patient-reported sputum volume was associated with antibiotic prescribing when CRP was not measured, but considerably less so when it was measured. Reporting crackles on auscultation was the feature most strongly associated with antibiotic prescribing, and the magnitude of this association was large across all three CRP measurement groups.
Strengths and limitations
These data were obtained from the largest trial of patients with AECOPD in UK primary care, covering 86 general practices across England and Wales. The trial benefitted from a representative sample of this patient population,8,16 and, with high data completion, most participants were retained for these analyses. Clinicians in the participating practices were trained in study procedures and data collection processes in accordance with a standardised protocol, and this minimised any biases arising from variable research practices.
This was a secondary analysis of a randomised controlled trial, and no formal power calculation was conducted for these particular analyses. Furthermore, the ICC estimates should be interpreted with some caution, as these were obtained from data arising from a randomised controlled trial, and the sources of variation may reflect on the type of person a clinician was willing to include in such a trial. In addition, the calculation of ICC values on the log-odds scale for binary variables, while not depending on cluster prevalence, may not directly translate to other studies. The ICC of 0.60 for clinician-reported evidence of consolidation likely reflects the variability in clinical assessment of this feature, as well as how rare it is in primary care. Finally, it is not possible to draw causal conclusions regarding the presenting features and their relationship to antibiotic prescribing.
The considerable practice variation in recording of clinical features suggests a high degree of subjectivity, as has been shown in previous studies.17,18 It is also not possible to rule out a relationship between clinical features and antibiotic prescribing being confounded by clinicians’ perceptions of the need for antibiotics, which have previously been shown to influence the recording of ‘objective’ features such as clinical findings and diagnosis.19
Comparison with existing literature
Several of the study’s findings are consistent with previous studies on the determinants of antibiotic prescribing for acute cough/lower respiratory tract infection in primary care, including crackles, wheeze, and diminished breath sounds (and other abnormal auscultation findings).20–23
The finding that increasing age was associated with lower odds of antibiotic prescribing was unexpected and inconsistent with the study by Llor and colleagues.4 The current study differs in two key ways. First, it was a randomised controlled trial with several eligibility criteria, whereas the study by Llor and colleagues was an observational study, in which clinicians included all patients over a defined time period. Thus, the current study may have inadvertently excluded older participants who would more likely be prescribed antibiotics, despite there being no upper age limit. Second, the association between age and antibiotic prescribing in the current study was adjusted for CRP measurement and increased sputum purulence (none, <20 mg/l, or ≥20 mg/l), whereas the study by Llor and colleagues was adjusted for several variables in a multivariable analysis (sex, days with symptoms, several different types of symptoms, utilisation of CRP, clinician request for a chest X-ray, and patient demanding antibiotics).
The weak association between sputum volume and antibiotic prescribing may indicate that clinicians are less certain about an increase in sputum volume as an indicator of bacterial infection compared with other clinical features. This is in line with the GOLD statement24 that sputum purulence is the strongest predictor of bacterial infection among the Anthonisen criteria, and that sputum volume and increased dyspnoea should not be emphasised in the absence of purulence. This point of view is supported by Miravitlles and colleagues,25 who found that purulence was the only Anthonisen criterion independently predicting an unfavourable outcome in patients with AECOPD treated with placebo.
Implications for research
Clinicians use a range of demographic and clinical features, including age and lung sounds, in their decision to prescribe antibiotics to patients presenting with AECOPD in UK primary care. In this study, the importance attributed to chest findings, and crackles in particular, in deciding on prescribing of antibiotics for AECOPD is not supported by a strong evidence base nor included in current guidelines. The emphasis on crackles by clinicians is probably related to the increased frequency found in pneumonia.26 However, crackles are commonly heard in COPD,27 and especially during exacerbations, related to worsened bronchial obstruction.28 In the present study, while the link between crackles and antibiotic prescribing was independent of CRP result, a greater number of participants in the high CRP group (59.2%) experienced crackles than did those in the low CRP group (44.0%), indicative of a relationship between crackles and more seriously unwell participants. Further investigation is required to determine the diagnostic and prognostic value of crackles and other chest sounds, and whether further safe reductions in antibiotic prescribing for AECOPD are possible.
Acknowledgments
The authors would like to thank the patients who participated in the trial and their families, without whom this study would not have been possible. Thanks also to the contribution of other members of the PACE trial team (Angela Watkins, Christy Barlow, Deborah Fitzsimmons, and Micaela Gal). Jacqueline Nuttall provided study design input.
Two UK Clinical Research Collaboration-registered clinical trials units were involved in the study: Centre for Trials Research, Cardiff University; and University of Oxford Primary Care and Vaccines Clinical Trials Collaborative. Thanks to Health and Care Research Wales workforce and the following Clinical Research Networks (CRNs) for their support in helping to identify sites and carry out notes reviews at these sites: Thames Valley & South Midlands CRN, East Midlands CRN, West Midlands CRN, West of England CRN, North Thames CRN, North West London CRN, and South London CRN. Thanks to Abbott Rapid Diagnostics, formally Alere Ltd, which provided the Afinion analysers and CRP cartridges and controls to the recruitment sites at no cost. Alere provided training on the use of the CRP point-of-care tests to a number of the participating sites.
Notes
Funding
The study was supported by funds from the National Institute for Health Research (NIHR) Health Technology Assessment Programme (project number: 12/33/12).
Ethical approval
Ethical approval for the PACE trial was given on 15 September 2014 by the Research Ethics Committee (REC) for Wales (Wales REC 6), recognised by the UK Ethics Committee Authority (REC reference number: 14/WA/1106). The aims of the current study fall within the remit of the original ethics application.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
David Gillespie, Ann Cochrane, Bernadette Sewell, Emma Thomas-Jones, Gurudutt Naik, Helen Stanton, Janine Bates, Evgenia Riga, Kerenza Hood, Nigel Kirby, Patrick White, Rachel Lowe, Rhiannon Phillips, and Nick A Francis report grants from NIHR, during the conduct of the study. Christopher C Butler reports grants from NIHR, NIHR Health Technology Assessment Programme, NIHR Health Protection Research Unit on Health Care Associated Infections and Antimicrobial Resistance, and NIHR Community Healthcare MedTech and In Vitro Diagnostics Cooperative. Afinion C-reactive protein (CRP) devices and associated training to participating general practices were provided at no cost to the study by Alere; and is part of publicly funded research consortia that include industrial partners. All other authors have declared no competing interests.
Data sharing
Data available from the authors on request.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received September 7, 2020.
- Revision requested November 1, 2020.
- Accepted November 23, 2020.
- © The Authors
This article is Open Access: CC BY 4.0 licence (http://creativecommons.org/licences/by/4.0/).
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

