


Article Figures & Data
Figures
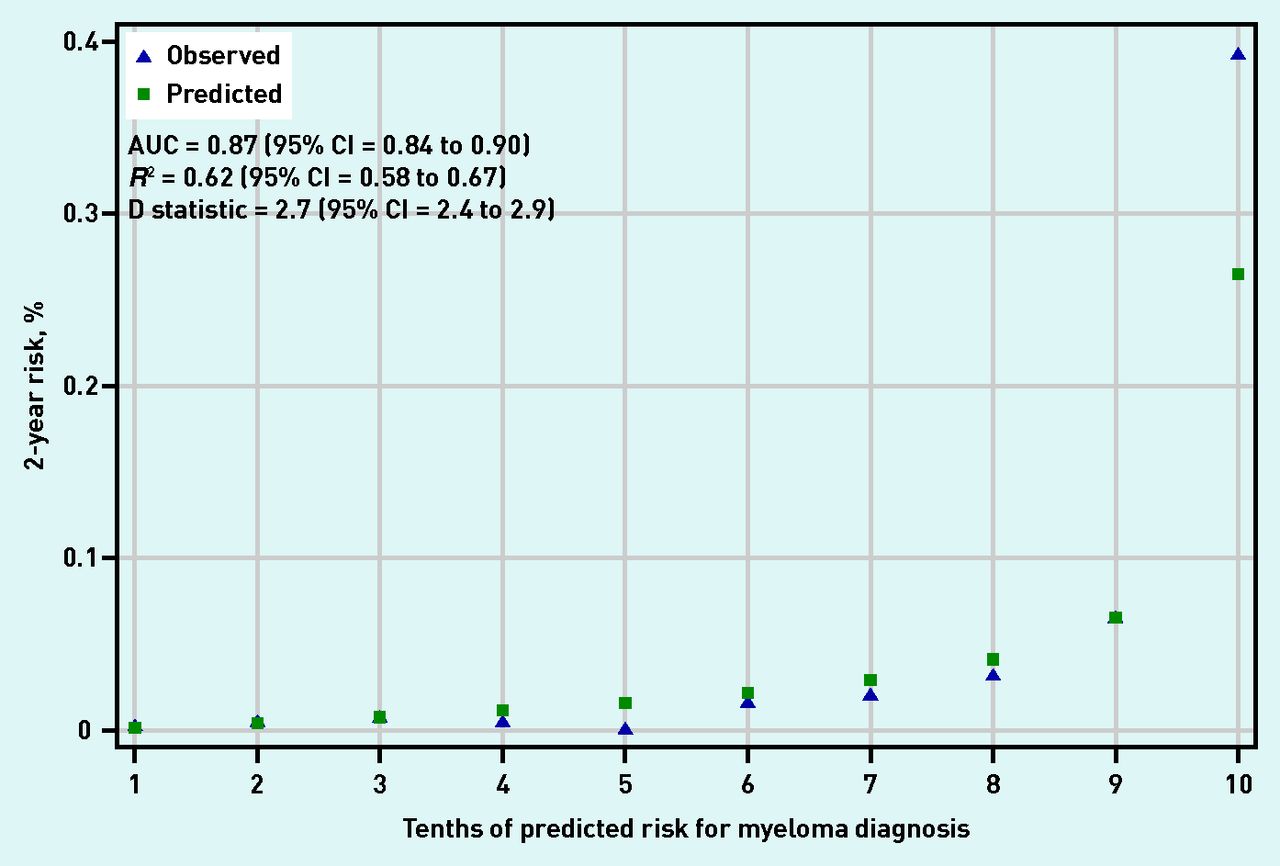
- Figure 1.
Calibration and discrimination of full blood count model.
AUC = area under curve.
- Figure 2.
Calibration and discrimination of all-test model.
AUC = area under curve.

{kind=link}
{kind=link}
Tables
How this fits in
Multiple myeloma is a haematological cancer in which 50% of patients experience symptoms for at least 3 months before diagnosis and have multiple consultations in primary care before referral to secondary care. Symptoms on their own are not predictive enough to suggest referral and they have to be combined with abnormalities in blood tests. The authors of the present study developed two clinical prediction rules that combine patient characteristics, symptoms, and common blood tests to identify patients at high risk of having undiagnosed myeloma. The study found that the prediction rules were shown to have good discrimination, and have the potential to reduce the delays observed in the diagnosis of myeloma. Variable Missing data (n = 835 404), n (%)a Non-myeloma (n= 834 909), n (%)a Myeloma (n= 495), n (%)a Demographics Female 0 (0.0) 492 039 (58.9) 227 (45.9) Mean age, years (SD) 0 (0.0) 63.7 (13.8) 70.9 (10.5) Mean BMI (SD) 541 782 (64.9) 28.5 (6.2) 26.5 (4.6) Symptoms Back pain 0 (0.0) 78 291 (9.4) 94 (19.0) Chest pain 0 (0.0) 53 256 (6.4) 56 (11.3) Bone pain 0 (0.0) 12 933 (1.5) 12 (2.4) Rib pain 0 (0.0) 3809 (0.5) 8 (1.6) Joint pain 0 (0.0) 35 348 (4.2) 19 (3.8) Shortness of breath 0 (0.0) 66 047 (7.9) 53 (10.7) Chest infections 0 (0.0) 54 198 (6.5) 40 (8.1) Fatigue 0 (0.0) 66 903 (8.0) 34 (6.9) Nosebleeds 0 (0.0) 7022 (0.8) 14 (2.8) Bruising 0 (0.0) 8682 (1.0) 5 (1.0) Fracture 0 (0.0) 13 361 (1.6) 12 (2.4) Weight loss 0 (0.0) 10 985 (1.3) 12 (2.4) Nausea 0 (0.0) 25 126 (3.0) 21 (4.2) Blood tests 2nd FBC test (index) Mean haemoglobin (SD) 50 292 (6.0) 13.5 (1.6) 12.0 (1.9) Mean white cell count (SD) 62 843 (7.5) 7.3 (5.2) 6.5 (3.6) Mean platelets (SD) 67 222 (8.0) 265.4 (80.2) 247.4 (80.6) Mean MCV (SD) 72 537 (8.7) 90.6 (5.9) 93.5 (6.1) Difference in FBC parameters (2nd – 1st) Mean haemoglobin diff (SD) 87 941 (10.5) 0.01 (1.0) −0.25 (1.1) Mean white cell count diff (SD) 101 091 (12.1) −0.04 (5.3) 0.13 (2.3) Mean platelets diff (SD) 107 485 (12.9) −1.8 (54.9) −2.9 (61.1) Mean MCV diff (SD) 114 841 (13.7) 0.19 (3.1) −0.06 (2.4) Other tests Mean calcium (SD) 634 969 (76.0) 2.3 (0.12) 2.4 (0.18) Mean creatinine (SD) 453 831 (54.3) 89.3 (30.2) 99.9 (44.9) Mean ESR (SD) 621 155 (74.4) 18.6 (19.5) 55.3 (41.7) CRP, median (IQR) 679 841 (81.4) 5 (2 to 10) 5 (2.5 to 17) Mean PV (SD) 798 298 (95.6) 1.71 (0.16) 1.96 (0.73) Blood tests (normal/abnormal)b FBC (index test) Anaemia 50 292 (6.0) 120 247/784 649 (15.3) 269/463 (58.1) Leukopenia 62 843 (7.5) 22 424/772 119 (2.9) 59/442 (13.3) Low platelets 67 222 (8.0) 25 165/767 738 (3.3) 44/444 (9.9) High MCV 72 537 (8.7) 52 385/762 443 (6.9) 85/424 (20.0) Other testsb Abnormal calcium 634 969 (76.0) 4056/200 263 (2.0) 14/172 (8.1) High creatinine 453 831 (54.3) 56 106/381 341 (14.7) 63/232 (27.2) High ESR 621 155 (74.4) 89 735/214 088 (41.9) 129/161 (80.1) High CRP 679 841 (81.4) 51 000/155 452 (32.8) 47/111 (42.3) High PV 798 298 (95.6) 14 080/37 084 (38.0) 15/22 (68.2) ↵a Unless otherwise stated.
↵b Percentages reported for patients with complete data. Denominator displayed to indicate where missing data applies. BMI = body mass index. CRP = C-reactive protein. ESR = erythrocyte sedimentation rate. FBC = full blood count. IQR = interquartile range. MCV = mean corpuscular volume. PV = plasma viscosity. SD = standard deviation.
Variable FBC model,a All-test model,b HR (95% CI) HR (95% CI) Demographics Female 0.45 (0.37 to 0.54) 0.48 (0.39 to 0.58) Agec FP (0.5, 0.5) FP (0.5, 0.5) Symptoms Back pain 2.37 (1.89 to 2.98) 2.46 (1.96 to 3.10) Chest pain 1.76 (1.33 to 2.33) 1.85 (1.39 to 2.45) Rib pain 2.94 (1.46 to 5.99) 2.81 (1.38 to 5.72) Nosebleeds 2.26 (1.32 to 3.85) 2.11 (1.23 to 3.61) FBC Haemoglobinc FP (3, 3) FP (3, 3) White cell countc FP (−2, −2) FP (−2, −2) Plateletsc FP (−1, −0.5) FP (−0.5, 0) MCVc FP (3, 3) FP (3, 3) Other tests ESR NA 1.03 (1.03 to 10.33) Calciumc NA FP (−1) ↵a FBC model contains a single FBC.
↵b All-test model contains a single FBC, plus ESR and calcium.
↵c Numerals in parenthesis represent the transformations used. CI = confidence interval. ESR = erythrocyte sedimentation rate.
FBC = full blood count. FP = fractional polynomials. HR = hazard ratio. MCV = mean corpuscular volume. NA = not applicable.
- Table 3.
Comparison of different diagnostic approaches in the validation cohort (after performing imputation)a
Variable Pr, %b Sensitivity, % (95% CI) Specificity, % (95% CI) LR+ (95% CI) LR– (95% CI) PPV, % (95% CI) NPV, % (95% CI) Symptoms Back pain NA 21.5 (16.5 to 27.2) 91.2 (91.1 to 91.3) 2.4 (1.9 to 3.1) 0.86 (0.81 to 0.92) 0.13 (0.10 to 0.17) 99.95 (99.94 to 99.96) Rib pain NA 1.2 (0.3 to 3.6) 99.5 (99.5 to 99.5) 2.5 (0.8 to 7.7) 0.99 (0.99 to 1.0) 0.14 (0.01 to 0.29) 99.94 (99.94 to 99.95) Chest pain NA 9.1 (5.8 to 13.4) 93.6 (93.6 to 93.7) 1.4 (0.9 to 2.1) 0.97 (0.93 to 1.0) 0.08 (0.05 to 0.11) 99.95 (99.94 to 99.95) Nosebleeds NA 1.2 (0.3 to 3.6) 99.2 (99.2 to 99.2) 1.6 (0.5 to 4.9) 0.99 (0.98 to 1.0) 0.09 (0.01 to 0.18) 99.94 (99.94 to 99.95) FBC (index test) Anaemia (any type) NA 55.6 (48.6 to 62.5) 83.6 (83.5 to 83.7) 3.4 (3.2 to 3.6) 0.53 (0.39 to 0.67) 0.18 (0.15 to 0.21) 99.97 (99.96 to 99.98) Normocytic anaemia NA 43.5 (37.0 to 50.0) 85.1 (84.9 to 85.2) 2.9 (2.7 to 3.2) 0.66 (0.54 to 0.77) 0.15 (0.13 to 0.19) 99.96 (99.95 to 99.97) Macrocytic anaemia NA 11.9 (8.1 to 15.8) 98.5 (98.4 to 98.6) 8.1 (6.3 to 9.8) 0.89 (0.84 to 0.95) 0.43 (0.26 to 0.61) 99.95 (99.94 to 99.96) Low platelets NA 8.3 (5.5 to 11.1) 96.5 (96.4 to 96.6) 2.4 (1.9 to 2.9) 0.95 (0.91 to 0.98) 0.13 (0.07 to 0.18) 99.95 (99.94 to 99.96) Low WCC NA 7.0 (4.5 to 9.6) 96.9 (96.9 to 97.0) 2.3 (1.7 to 2.9) 0.96 (0.93 to 0.99) 0.13 (0.06 to 0.19) 99.94 (99.94 to 99.95) High MCV NA 22.9 (17.5 to 28.4) 91.6 (91.5 to 91.7) 2.8 (2.3 to 3.2) 0.84 (0.76 to 0.92) 0.15 (0.10 to 0.19) 99.95 (99.94 to 99.96) Other tests Hypercalcemia NA 5.7 (1.9 to 9.6) 98.3 (98.2 to 98.4) 3.4 (1.3 to 5.5) 0.96 (0.91 to 1.0) 0.19 (0.04 to 0.33) 99.95 (99.94 to 99.96) High ESR NA 80.3 (70.4 to 90.3) 54.8 (54.5 to 55.1) 1.7 (1.6 to 1.9) 0.35 (0.08 to 0.63) 0.10 (0.08 to 0.11) 99.98 (99.97 to 99.99) High ESR or anaemia NA 90.5 (81.4 to 99.5) 50.0 (49.8 to 50.3) 1.8 (1.7 to 1.9) 0.19 (0.13 to 0.28) 0.10 (0.08 to 0.12) 99.99 (99.98 to 99.99) High ESR and anaemia NA 45.5 (38.9 to 51.9) 88.4 (88.2 to 88.5) 3.9 (3.6 to 4.2) 0.62 (0.50 to 0.74) 0.20 (0.17 to 0.25) 99.96 (99.96 to 99.97) FBC model 77th percentilec 0.06 78.9 (73.2 to 83.9) 77.2 (77.1 to 77.3) 3.5 (3.2 to 3.7) 0.27 (0.21 to 0.35) 0.19 (0.16 to 0.22) 99.98 (99.97 to 99.98) 90th percentile 0.12 61.6 (55.1 to 67.7) 90.2 (90.1 to 90.3) 6.3 (5.7 to 6.9) 0.43 (0.36 to 0.50) 0.34 (0.29 to 0.40) 99.98 (99.97 to 99.98) 95th percentile 0.20 41.3 (35.1 to 47.8) 95.1 (95.0 to 95.2) 8.4 (7.3 to 9.8) 0.62 (0.55 to 0.69) 0.46 (0.37 to 0.55) 99.96 (99.96 to 99.97) 99th percentile 0.60 18.2 (13.5 to 23.6) 99.1 (99.1 to 99.1) 19.9 (15.2 to 26.1) 0.83 (0.78 to 0.88) 1.10 (0.80 to 1.40) 99.95 (99.95 to 99.96) 99.5th percentile 0.90 12.8 (8.9 to 17.7) 99.5 (99.5 to 99.6) 27.6 (19.8 to 38.4) 0.88 (0.84 to 0.92) 1.50 (1.00 to 2.10) 99.95 (99.95 to 99.96) 99.9th percentile 2.20 4.1 (2.0 to 7.5) 99.9 (99.9 to 99.9) 42.4 (23.5 to 82.9) 0.96 (0.94 to 0.99) 2.30 (1.10 to 4.10) 99.95 (99.94 to 99.95) All-test model 84th percentilec 0.06 82.6 (77.3 to 87.2) 83.9 (83.8 to 84.0) 5.1 (4.8 to 5.4) 0.21 (0.16 to 0.27) 0.28 (0.24 to 0.32) 99.98 (99.98 to 99.99) 90th percentile 0.09 71.9 (65.8 to 77.5) 90.3 (90.2 to 90.4) 7.4 (6.9 to 8.0) 0.31 (0.25 to 0.38) 0.40 (0.34 to 0.47) 99.98 (99.97 to 99.98) 95th percentile 0.15 62.4 (56.8 to 68.5) 95.1 (95.0 to 95.1) 12.9 (11.7 to 14.2) 0.40 (0.34 to 0.47) 0.70 (0.59 to 0.81) 99.98 (99.97 to 99.98) 99th percentile 0.45 34.3 (28.3 to 40.6) 99.0 (99.0to 99.1) 35.1 (29.4 to 41.9) 0.66 (0.61 to 0.73) 1.9 (1.5 to 2.3) 99.96 (99.96 to 99.97) 99.5th percentile 0.70 24.0 (18.7 to 29.9) 99.5 (99.5 to 99.5) 48.9 (38.9 to 61.4) 0.76 (0.71 to 0.82) 2.6 (2.0 to 3.3) 99.96 (99.95 to 99.96) 99.9th percentile 1.90 7.8 (4.8 to 12.0) 99.9 (99.9 to 99.9) 80.5 (51.8 to 125.0) 0.92 (0.89 to 0.96) 4.2 (2.5 to 6.4) 99.95 (99.94 to 99.95) ↵a Results presented are based on multiple imputation as described in the methods section.
↵b Pr = corresponding probability (%) of the selected risk score percentile.
↵c These percentile values were selected to match the background prevalence in the whole cohort. ESR = erythrocyte sedimentation rate. FBC = full blood count. LR– = negative likelihood ratio. LR+ = positive likelihood ratio. MCV = mean corpuscular volume. NA = not applicable. NPV = negative predictive value. PPV = positive predictive value. WCC = white cell count.
- Table 4.
Performance of the different diagnostic approaches in a population of 100 000 tested individuals based on the validation cohort measures
Variable Per 100 000 patients (60 myeloma cases), n Ratio of false alarms to cancers diagnosed Ratio of true negatives to cancers missed Cancers diagnosed False alarms Cancers missed Correctly spared investigations Symptoms Back pain 13 8995 47 90 945 692 to 1 1935 to 1 Chest pain 5 5996 55 93 944 1199 to 1 1708 to 1 Rib pain 1 500 59 99 440 500 to 1 1685 to 1 Nosebleeds 1 800 59 99 140 800 to 1 1680 to 1 FBC (index test) Anaemia (any type) 34 16 990 26 82 950 500 to 1 3190 to 1 Low platelets 5 2998 55 96 942 600 to 1 1763 to 1 Low WCC 4 2999 56 96 941 750 to 1 1731 to 1 High MCV 14 7995 46 91 945 571 to 1 1998 to 1 Other tests Hypercalcemiaa 4 1999 56 97 941 500 to 1 1748 to 1 High ESRa 48 44 973 12 54 967 936 to 1 4581 to 1 High ESR or anaemiaa 54 49 970 6 49 970 925 to 1 8328 to 1 High ESR and anaemiaa 27 11 993 33 87 947 444 to 1 2665 to 1 FBC model Prevalence 48 22 986 12 76 954 479 to 1 6412 to 1 90th percentile 37 9994 23 89 946 270 to 1 3910 to 1 95th percentile 25 4997 35 94 943 200 to 1 2712 to 1 99th percentile 11 999 49 98 941 91 to 1 2019 to 1 All-test modela Prevalence 50 16 090 10 83 850 322 to 1 8385 to 1 90th percentile 43 9994 17 89 946 232 to 1 5290 to 1 95th percentile 37 4997 23 94 943 135 to 1 4127 to 1 99th percentile 20 999 40 98 941 25 to 1 2473 to 1 ↵a Corresponds to the performance measures if ESR and calcium were to be ordered for all patients in the sample. ESR = erythrocyte sedimentation rate. FBC = full blood count.
MCV = mean corpuscular volume. WCC = white cell count.
Supplementary Data
Supplementary material is not copyedited or typeset, and is published as supplied by the author(s). The author(s) retain(s) responsibility for its accuracy.
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

