


Article Figures & Data
Figures
- Figure 1.
PRISMA diagram. T2DM = type 2 diabetes mellitus.
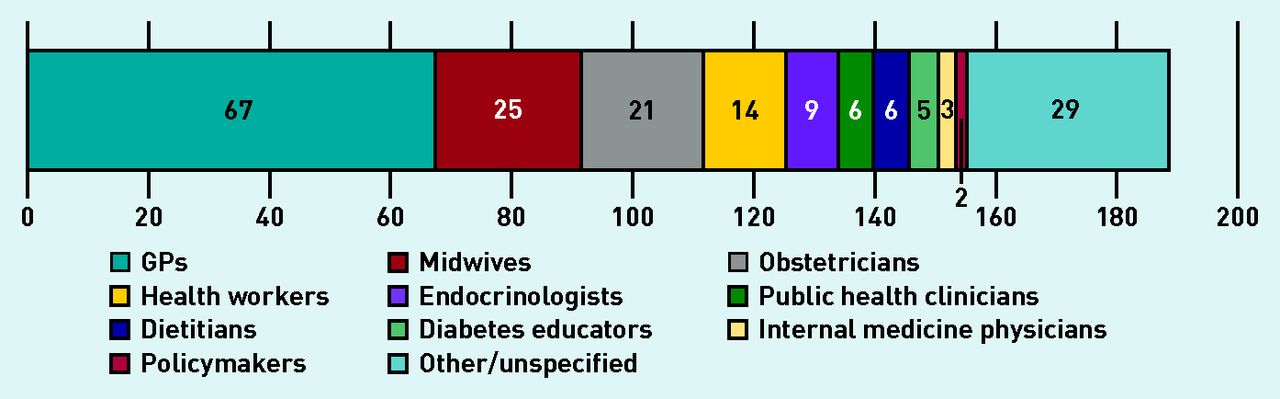
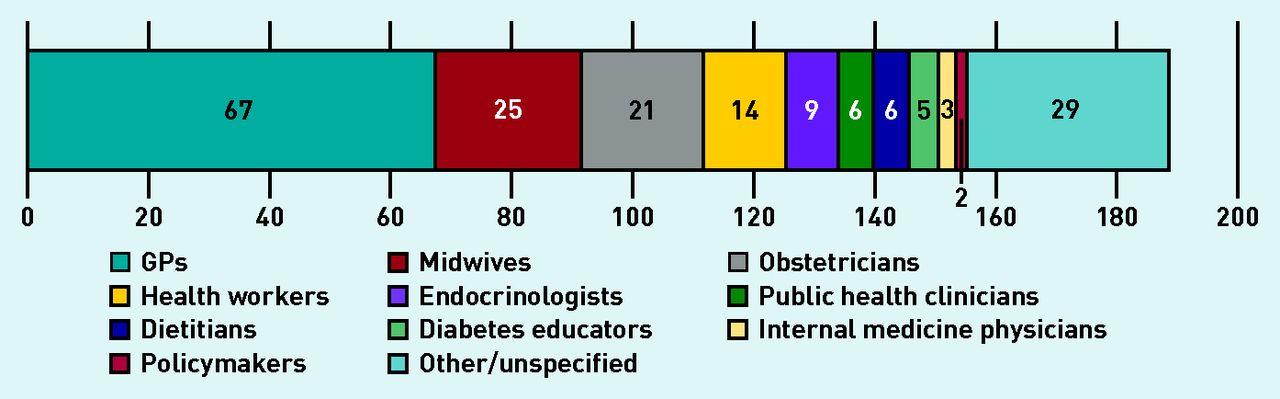
- Figure 2.
Types of clinicians represented in the qualitative synthesis.

{kind=link}
{kind=link}
Tables
How this fits in
Postpartum diabetes screening after a gestational-diabetes-affected pregnancy is poorly attended, and barriers to attendance have been examined from women’s perspectives and in quantitative-based reviews from clinicians’ perspectives. This systematic review and thematic synthesis of qualitative studies included a wide variety of clinicians from different settings to provide deeper insight into handover difficulties between primary and secondary care as well as patient-centric barriers. It also revealed how a focus on short-term medical issues negatively impacts screening rates. Addressing these barriers through improved clinical protocols, better reminder systems, and more convenient testing options may allow for improved uptake of screening. CASP appraisal criteria Doran, 201024 Wilkinson, 201427 Bernstein, 201622 Campbell, 201725 Pennington, 201728 Hewage, 201821 Muhwava, 201823 Kilgour, 201926 McCloskey, 201920 Clear aims? ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ Qualitative methodology appropriate? ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ Appropriate research design? ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ Appropriate recruitment strategy? ✓ ✓ ? ✓ ✓ ✓ ✓ ✓ ✓ Appropriate data collection? ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ Adequate consideration of relationship between researcher and participants? ? X X ? X X X X X Consideration of ethical issues? ? ? ? ? ? ? ✓ ✓ ? Data analysis sufficiently rigorous? X ? ✓ ✓ ✓ ? ✓ ✓ ✓ Clear statement of findings? ? ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ Valuable to the literature review? ? X ✓ ? ✓ ✓ ✓ ✓ ✓ Total score 7 7 8 8.5 8.5 8 9 9 8.5 ↵✓ = Clearly met criterion. ? = Unclear if criterion met. X = Criterion not met. CASP = Critical Appraisal Skills Programme.
Theme Quotes/explanation 1. Difficulties in handover between primary and secondary care Ambiguous roles and responsibilities
‘Look how confusing it is. Who do you see, when do you see them, who do you refer them to? There’s no simple pathway.’ (health professional)25
‘One of the core issues is that you’ve got a resource constrained situation, [clinicians] are full to the brim […] Their job is 120%, so anything else you give them, is a problem.’ (public health specialist)23
‘It’s not that people are not aware that [screening] needs to be done, it is because the environment will be challenging for people to be doing OGTTs. That’s associated with human as well as financial resources.’ (obstetrician)23
‘I personally hate those […] discharges, they are impossible! I mean something much more succinct, a summary. They obviously have printed the entire record!’ (GP)26
Discharge summaries that: ‘Tell us how she is going, what you have done, what you are going to do and what you want me to do.’ (GP)26
‘No proper system to identify and retain patients in the current care model.’ (primary care clinician)21
2. Short-term focus in consultations ‘We present it like “okay, you have GDM, it’s a potential risk, but it’s not technically affected the baby per se.” I think we may be part of it […] that we maybe simplify it so they don’t see it as “oh it’s not going to kill my baby right”.’ (community nurse midwife)20
‘Our focus is the pregnancy, keep the sugar down, try and have a healthy baby and a mother that’s not injured during the birth. And we don’t think too much to the afterwards.’ (professor in obstetrics)23
‘You see the patient and talk about the baby but not beyond.’ (unspecified)22
3. Patient barriers ‘They’ve got too many other things.’ (GP)28
‘They’re so focused on the here and now they can’t even comprehend what might happen in the future.’ (health worker)25
‘The drink, a lot of people don’t like it, so they won’t come in for it. And the time it takes to have it as well.’ (health worker)25
GDM = gestational diabetes mellitus. OGTT = oral glucose tolerance test.
Clinician Their role/priorities Consequences for postpartum screening Quotes Hospital clinicians GDM management main priority and prevention much lower priority
Role ends at ∼6 weeks postpartum, so no control over follow-up
Viewed as important but not their role
Long-term risk communication is lacking:
Fear of overwhelming patient and impacting GDM control
No time for discussions
‘Our focus is the pregnancy, keep the sugar down, try and have a healthy baby and a mother that’s not injured during the birth. And we don’t think too much to the afterwards.’ (professor in obstetrics)23
‘I don’t feel equipped to handle a positive test, so I think that’s why I don’t have them follow-up with me […] I want them to follow-up with their primary care provider, so they can say “Okay, this is how we’re going to go forward in the future. And I feel like I’m not equipped to give them that information, so it wheels down to be like “Test is normal, you know, bye”.’ (community nurse midwife)22
Primary care providers Primary prevention a main priority but often lack sufficient information to support this process
Viewed as important, and their role, but the barriers prevent them achieving it
‘It is the GP role, our domain to follow that up.’ (GP)26
‘I would like to know what I am meant to do to be fairly clearly guided as to what to check when or what to do next time, or when to be seen back again.’ (GP)26
GDM = gestational diabetes mellitus.
Supplementary Data
Supplementary material is not copyedited or typeset, and is published as supplied by the author(s). The author(s) retain(s) responsibility for its accuracy.
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

