


The introduction of early palliative care might be hoped to moderate the medicalisation of dying and the increasingly frequent medical and surgical treatment that patients generally receive in the last months of life.
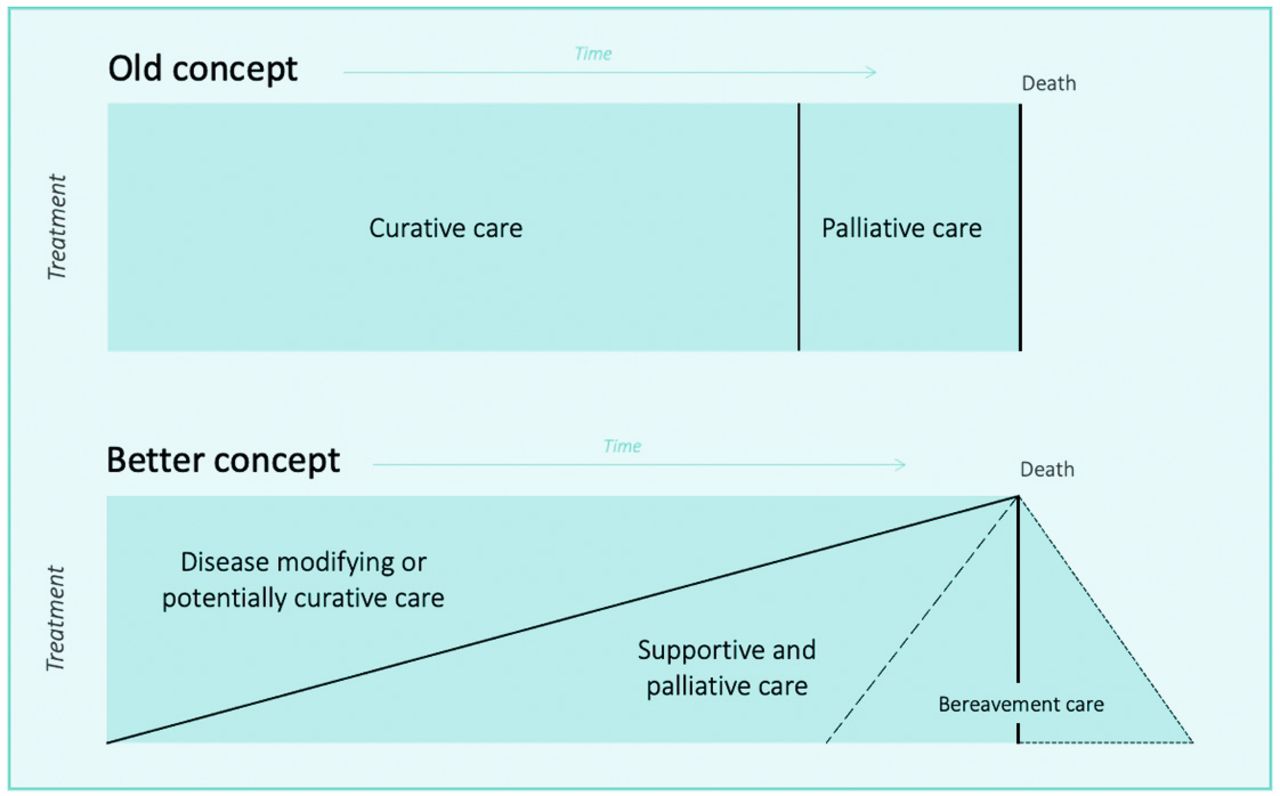
Indeed the old concept of an abrupt change from curative to palliative care when a person is terminally ill and imminently dying is giving way gradually to the better concept of a phased introduction of palliative care from diagnosis of a life-threatening illness, as advocated in Figure 1.1
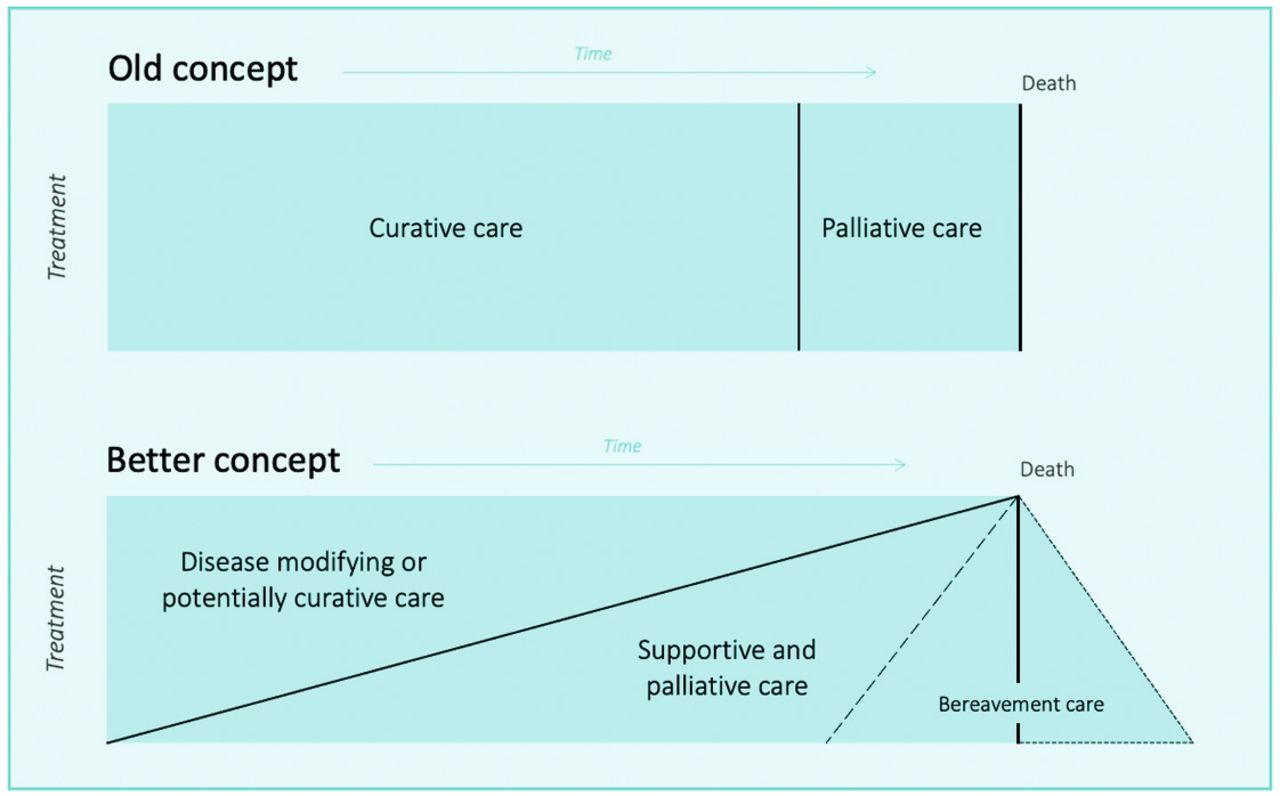
Contrasting the old concept of curative care being suddenly replaced by palliative care to a gradual introduction of palliative care from diagnosis of any life-threatening illness.
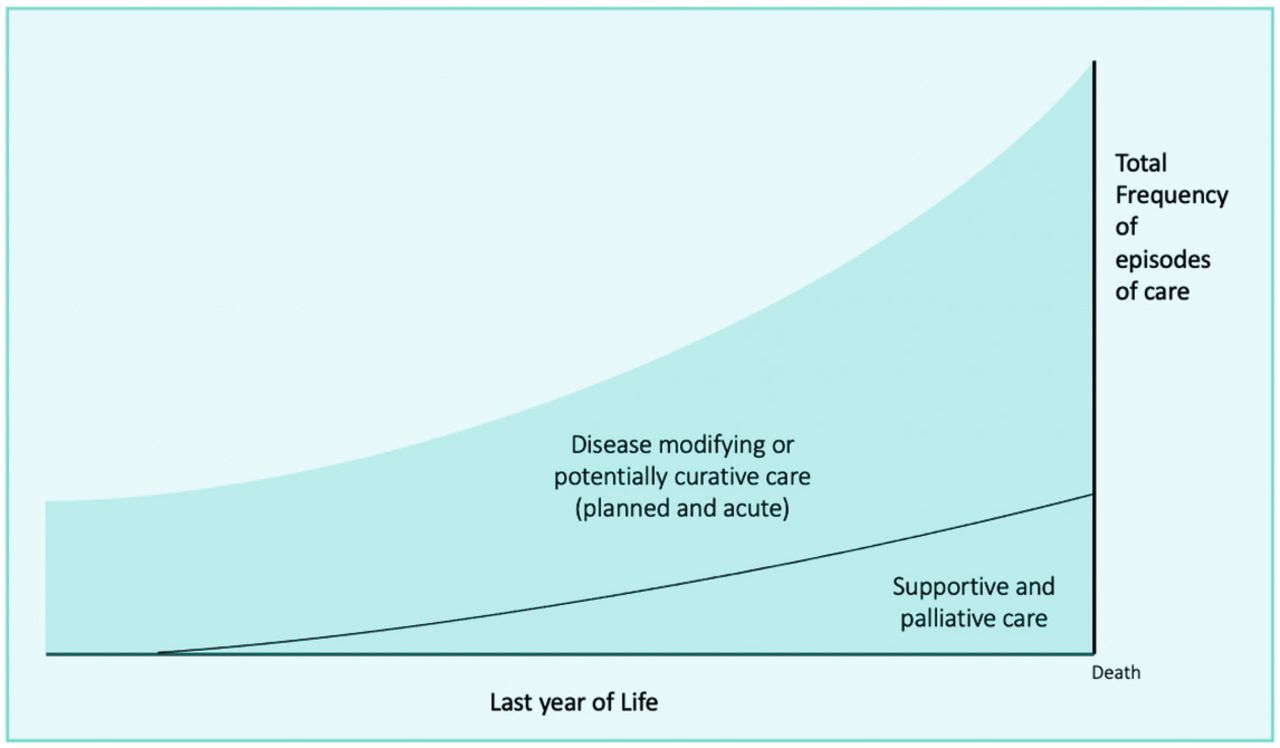
DISEASE MODIFYING OR POTENTIALLY CURATIVE CARE INCREASE RAPIDLY IN THE LAST MONTHS OF LIFE
By 2018, GPs in Scotland recognised 69% of their patients for a palliative care approach by the time they died, calling it ‘anticipatory care’. This ‘primary palliative care’ was associated with more frequent care planning, more patients dying in their place of choice, and less hospital admissions.2
However, while integrated palliative care delivery is gradually increasing throughout the last year of life, disease modifying and potentially curative care and unplanned care is not decreasing. It is instead increasing greatly, especially in the last 3 months of life.
Ninety-five percent of patients in their last year of life receive emergency and unscheduled care.3 Planned primary and hospital care for disease management also rise steeply in the last trimester in England and Canada.4,5
Figure 2 illustrates this by plotting the monthly frequency of medical service episodes that patients receive in their last year of life. This reveals the great increase in the number of episodes of ‘curative’ care as death approaches. This is hidden in Figure 1, which only shows the increasing percentage of people receiving a palliative care approach.
{kind=link}
{kind=link}
Overview of the monthly total frequency of medical service episodes patients receive in their last year of life.
So palliative care is reaching more people with cancer, organ failure, frailty, and dementia, and starting earlier, but planned and emergency medical care continues to expand even more both in hospitals and in primary care.
Why is this? Who is responsible for this, and whose job is it to address this issue? Palliative care specialists bemoan that their specialty is stigmatised, and referrals come late if at all. But they never consider they have a public health duty to address this issue of overzealous treatment of the population who are dying.
OVER-MEDICALISATION OF DEATH
Is it patients demanding more treatments than might be wise, hoping against hope for a cure? Is it hospital doctors doing what they can do and know how to do, rather than should do? Is it lack of effective care planning and communication between all settings? Is it the decrease in continuity of care, especially out-of-hours?
Compared to countries where curative care is not available to some patients at all due to lack of resources, inappropriate and sometimes very costly care is especially wrong and inequitable. The theoretical concept of early palliative care for all in the community is gaining ground slowly in practice in all World Health Organization regions, and there is no doubt that it can decrease emergency care and hospital admissions when care planning is in place and has been communicated between all settings.6
However, the deep-seated overmedicalisation of death must be addressed. Much of this care in retrospect is clearly futile, and quality indicators for appropriate and inappropriate end-of-life care in people with Alzheimer’s disease, cancer, or chronic obstructive pulmonary have been identified to assess this further.7
Low-value, high-cost care can cause much suffering. An early palliative approach can prevent or ameliorate suffering and must be an informed option and available for all. Primary care may be best placed to take this forward.

Footnotes
This article was first posted on BJGP Life on 15 Jul 2021; https://bjgplife.com/curative
- © British Journal of General Practice 2021
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

