


Childhood adversity or childhood trauma has been, and continues to be, connected to poor quality of health and life. A growing body of evidence points to millions of people across the world experiencing events in their childhood that are detrimental to their physical and mental development.
As a GP, I have grown to be interested in this subject and the role that primary care may have to play in mitigating the impact of this adversity. What I do know is that on an everyday basis patients tell me of the trauma they have experienced in their lives, be that as a child or as an adult.
CURRENT MANAGEMENT OF CHRONIC PAIN
This is a complex intergenerational problem that will require many streams of solutions. Fibromyalgia and chronic pain are common diagnoses found and coded in primary care. In the UK approximately 28 million people are thought to be affected by chronic pain (CP).1 CP is a complex problem across the world, costs the UK economy millions of pounds a year, and detrimentally impacts the quality of lives. Primary care manages the vast majority of patients with chronic pain whether or not there is a specific diagnosis, or it has an unknown origin. Only a small percentage of patients are referred to a secondary care pain clinic.
One paper has reported that 22% of GP consultations are regarding chronic pain.2 Childhood adversities are common across the world; the average number that people experience before the age of 18 is 2.5–2.9 different types of trauma.3 Negative experiences in childhood include physical abuse, emotional neglect and abuse, sexual abuse, and family dysfunction, as well as living with those with poor parental mental health or incarceration. These have been linked to chronic health conditions, including chronic pain, in adulthood.4
CHILDHOOD ADVERSITY AND CHRONIC PAIN
Childhood adversity can lead to more pain and greater dysfunction with the pain experienced.5 There is some debate in the literature, but childhood adversity is thought to be associated with fibromyalgia, with family dysfunction such as conflict, divorce, and being fearful of a family member, and alcohol abuse in parents being directly linked.6 Emotional neglect, lack of affection, and emotional abuse often goes unnoticed but can be linked to pain. Studies have concluded that patients with chronic pain should be asked about childhood trauma or current traumatic events.7 Studies also show that if any childhood adversity is not identified then management plans may not be as effective.8
For example, women with fibromyalgia may benefit from trauma-focused care9 and those with post-traumatic stress disorder arising from childhood adversity and chronic pain may benefit from therapy focusing on emotional regulation.10 However, we will not be able to refer people for these therapies if we do not know that trauma is part of their story. Assessing for any childhood adversity can therefore be important to developing management options for their pain. More societal education on the detrimental impact of childhood adversity is required. Further larger-scale research should address the assessment and management of these long-term sequelae of childhood adversity in primary care. Children should be safe in their environments at home, and, for those who did not have a safe and secure environment growing up and now experience pain, more consideration is required. Prevention of childhood adversity is crucial in reducing the impact chronic pain has in adulthood.
Why not try doing an audit in your practice?
MY AUDIT IN A SCOTTISH INNER-CITY PRACTICE
A question grew in my mind: If trauma was associated with fibromyalgia and chronic pain, were we asking about it? As a result, in April 2021 I conducted a short audit in an inner-city GP practice in Scotland.
My aim was to look and see what traumatic events, in adulthood or childhood, were being documented or enquired about for those who have been coded as chronic pain (CP) or fibromyalgia (FM). Literature review determined the most commonly used expressions of childhood adversity or current adversity as: abuse, trauma, neglect, adversity, or maltreatment. For the purposes of the audit, the term ‘trauma’ was used to encapsulate all known terms.
The practice has a mixed demographic across areas of deprivation. The practice has 6094 patients looked after by five GPs and two practice nurses as well as an extended team of administration staff, district nurses, health visitors, and a psychology clinical assistant.
Patients coded with either CP or FM were identified. Using the practice-based Vision software, electronic notes were searched for the above terms to determine whether patients with these conditions had ever been asked about these negative life events.
Ethical approval was not required as this was an audit based in a single practice. A total of 98 patients (14.0%) were identified with chronic pain, fibromyalgia, and both conditions.*
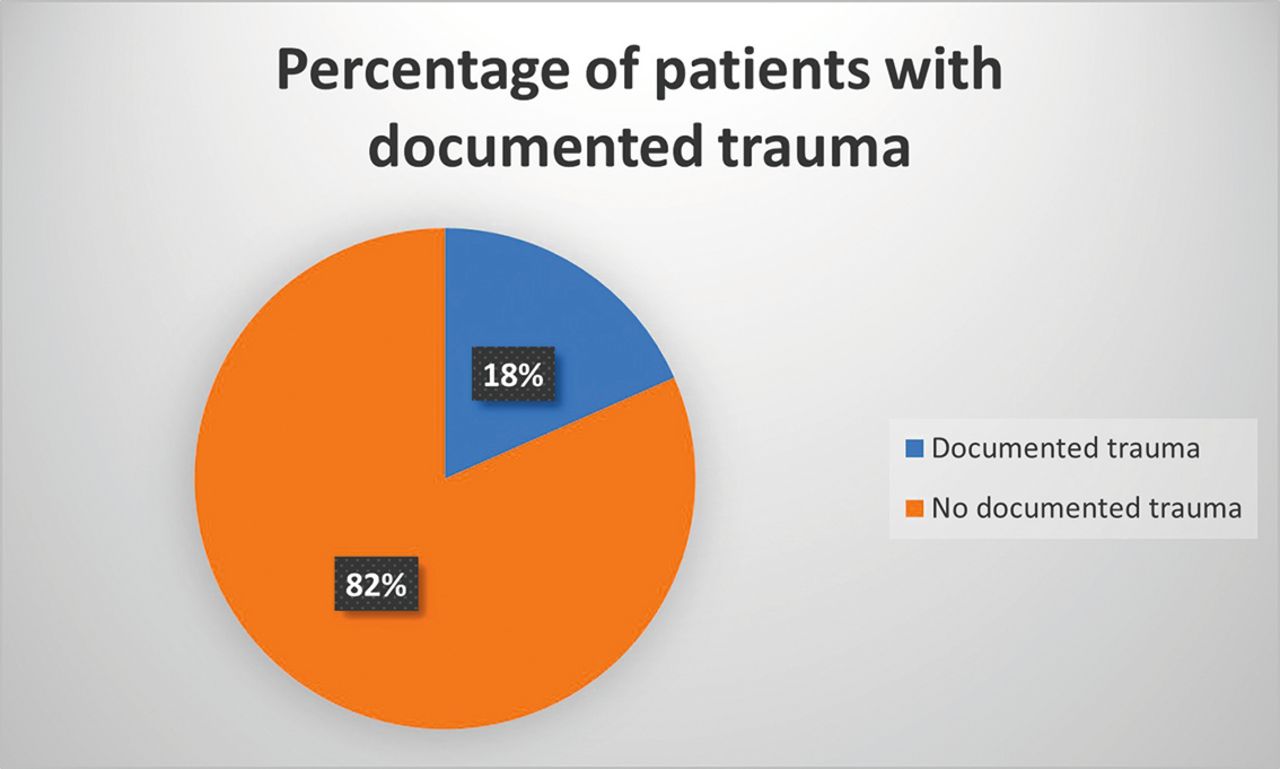
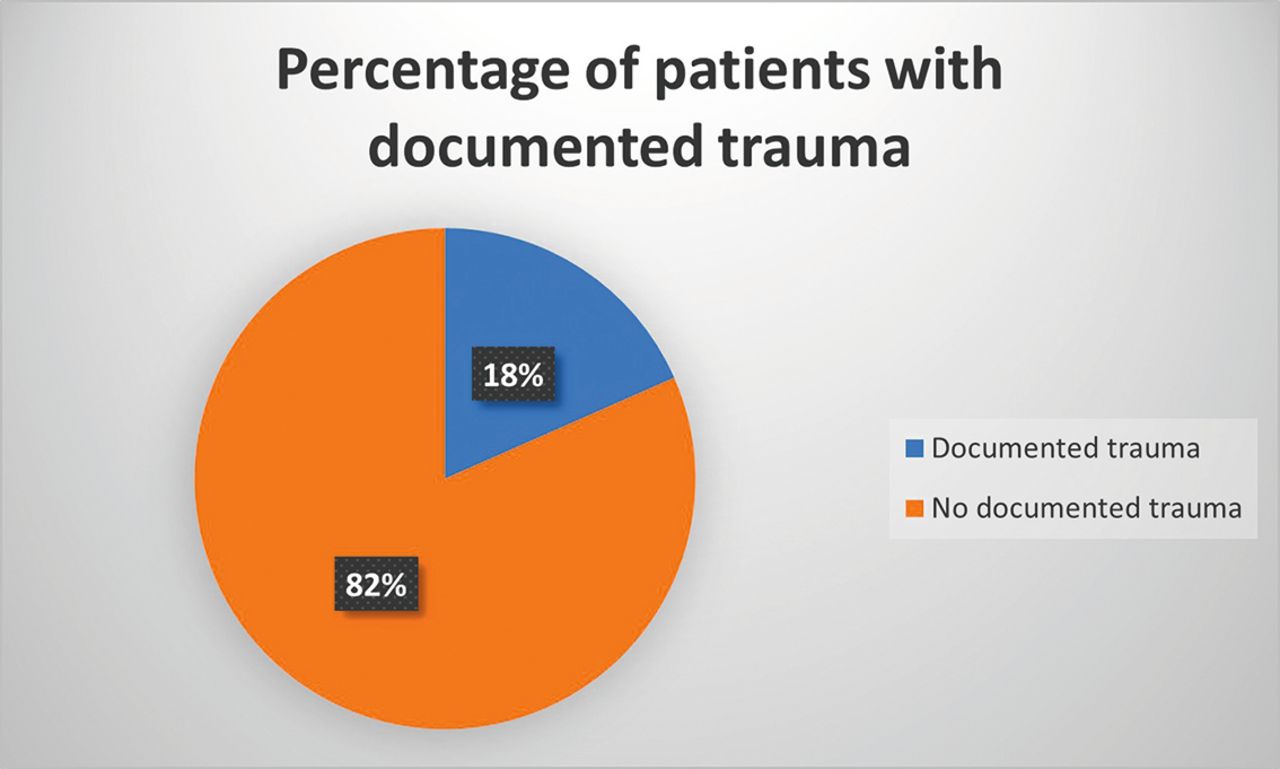
Figure 1 shows the results from across the two VisionTM codes utilised: CP = #1M52 and FM = #N248.
{kind=link}
Pie chart showing what percentage of patients with coded chronic pain, fibromyalgia, or both conditions have been asked about psychological trauma.
The pie chart shows that trauma had not been documented in many patient notes that have these codes.
TYPES OF TRAUMA THAT HAD BEEN REVEALED AND DOCUMENTED
Road traffic accident.
Childhood abuse.
Experience of abuse as an adult.
Domestic abuse as an adult.
Physical trauma.
Witnessing a traumatic event.
Sexual abuse as a child.
Sexual and physical abuse as a child.
Physical and emotional abuse as a child.
This audit revealed that only small numbers (18.0%; 18.4 of the 98 patients) had had trauma documented in primary care in this practice.
Footnotes
↵* Data reproduced with the permission of and verification by the relevant practice, which have been submitted to the editorial team.
This article was first posted on BJGP Life on 5 May 2022; https://bjgplife.com/fibro
- © British Journal of General Practice 2022
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

