


BACKGROUND
All major classes of antidepressants can cause a withdrawal syndrome when removed.1 Withdrawal is common, experienced by 56% of those stopping a selective serotonin reuptake inhibitor (SSRI), with rates varying between antidepressants.1–3 Historically, withdrawal was thought to be mild and self-limiting, misnamed a ‘discontinuation syndrome’; the 2022 National Institute for Health and Care Excellence (NICE) depression guidance still states that withdrawal symptoms ‘usually go away within 1 to 2 weeks’.4 However, most patients will experience symptoms of longer than 2 weeks.2 Additionally, contrary to previous understanding, symptoms of withdrawal are often severe, and can include increased suicidal ideation.1,2
Inaccurate guidance on antidepressant withdrawal has resulted in many patients experiencing distressing, debilitating symptoms; this is highlighted through the thousands of posts on online support groups, such as ‘Surviving Antidepressants’ (https://www.survivingantidepressants.org/). Some of these patients have been misdiagnosed as suffering from a relapse of their original mental health condition, with others left fearful to stop their antidepressant in the future.2 This has likely contributed to the increasing numbers of patients taking an antidepressant for an unnecessarily extended duration.5 Benefits to stopping antidepressants in stable patients include preventing side effects, and avoiding drug interactions and burden, alongside reducing costs.
Despite more widespread understanding of withdrawal syndrome and methods to taper antidepressants safely, there remains uncertainty on how to best manage patients wishing to stop their antidepressant, or already experiencing withdrawal symptoms. This article primarily discusses withdrawal from SSRIs as they are the most prescribed antidepressant class by GPs in England and are the main focus of research into withdrawal.5
WHY DO PEOPLE EXPERIENCE WITHDRAWAL?
By preventing the re-uptake of serotonin, SSRIs increase brain levels of serotonin alongside other neurotransmitters including noradrenaline, dopamine, and GABA. To adapt to this, the brain down-regulates serotonin receptors, reducing their sensitivity to serotonin. SSRI cessation triggers an abrupt reduction in the level of serotonin, which, coupled with reduced sensitivity, is perceived as a serotonin deficiency.1,6 Withdrawal symptoms therefore persist until the brain returns to its original level of sensitivity pre-antidepressant.7 Based on this, SSRIs in higher doses, used for longer periods of time and with shorter half-lives, such as paroxetine, will cause a more severe withdrawal.1
WHAT ARE THE SYMPTOMS OF WITHDRAWAL?
Owing to the vast distribution of serotonin receptors within the brain and body, potential withdrawal symptoms are diverse. Psychological symptoms include irritability, anxiety, low mood, sleep disturbance, suicidal ideation, and hallucinations. Physical manifestations include dizziness, flu-like illness, palpitations, headaches, muscle pain and tremors, sweating, gastrointestinal symptoms (nausea, diarrhoea), and sensory disturbances (‘electric shocks’, ‘brain zaps’).2–4
HOW CAN WE DIFFERENTIATE BETWEEN WITHDRAWAL AND RELAPSE?
Patients experiencing antidepressant withdrawal can easily be misdiagnosed as suffering from a relapse of their original mental health condition. This is because of similarity of psychological symptoms between the two, and because of poor understanding of the typical length and severity of withdrawal symptoms.7 Strategies to differentiate between withdrawal and relapse include:
Identifying if the patient is experiencing physical symptoms of withdrawal that are unlikely to be a feature of depressive relapse, such as sensory disturbances, muscle pain, or nausea;
Establishing the symptom timeline — withdrawal typically begins within days of antidepressant cessation, whereas relapse takes weeks to months. Because of the half-life of fluoxetine, withdrawal symptoms can begin weeks after cessation; and
Reintroduction of the antidepressant rapidly reduces the intensity of withdrawal symptoms, whereas, in relapse of anxiety or depression, core symptoms usually require weeks to improve.
HOW SHOULD THE GP STOP SOMEONE’S ANTIDEPRESSANT?
Tapering
SSRIs exhibit a hyperbolic dose–response relationship, that is, when reducing, decreases to smaller doses cause larger change to serotonin receptor occupancy. Because of this, traditional linear dose reductions (for example, reducing sertraline by 50 mg increments) cause increasingly large (or hyperbolic) changes to serotonin receptor inhibition and therefore more severe symptoms.1,6,7 This explains why some patients may tolerate the early stages of their taper but towards the end, at lower doses, they experience withdrawal symptoms.
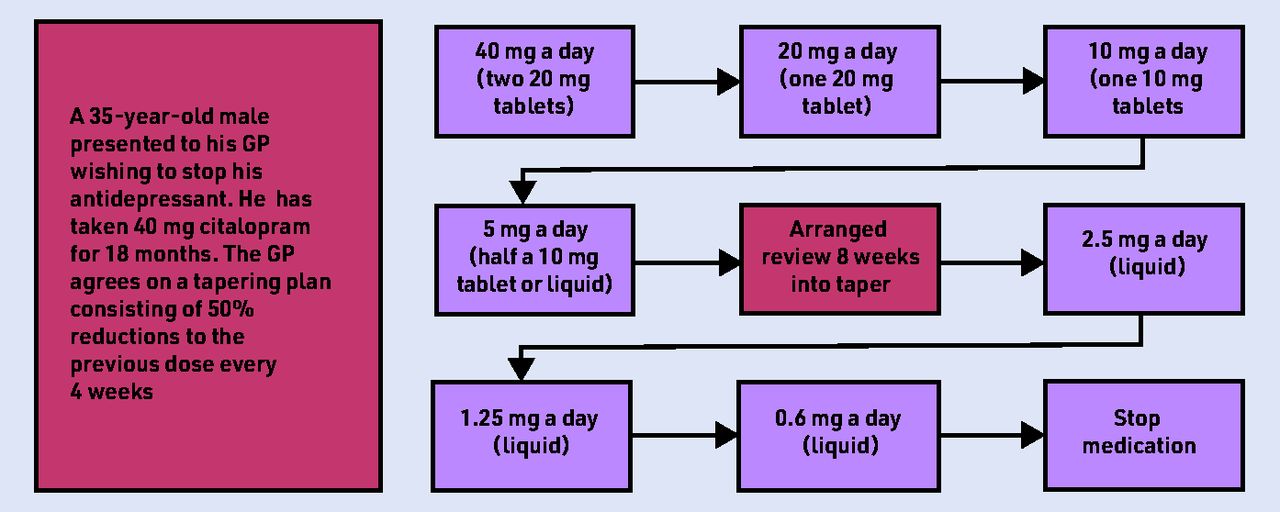
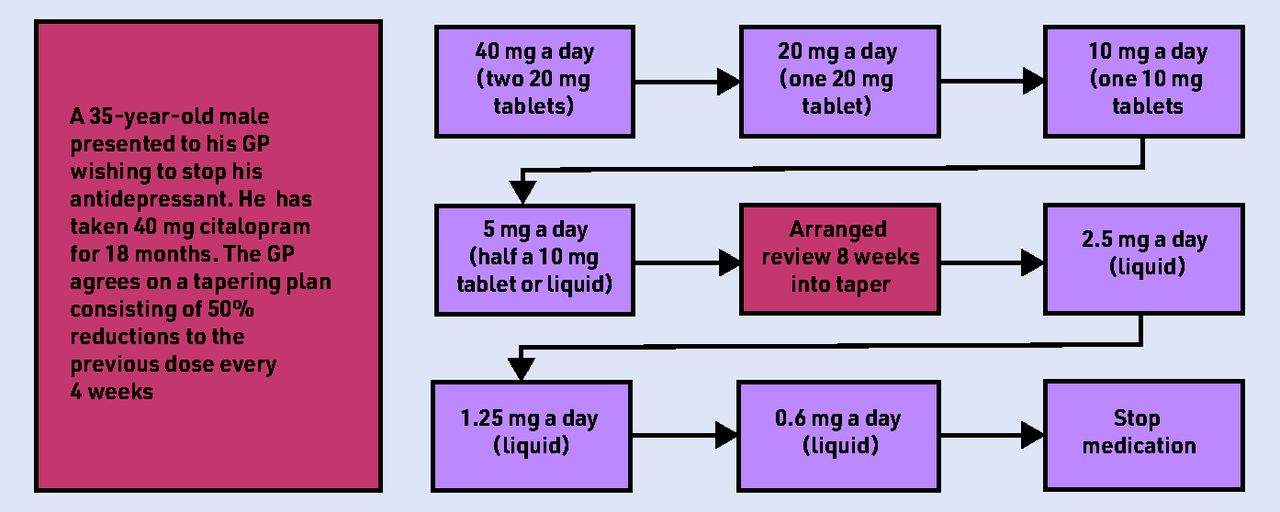
Instead, a proportionate taper, recommended by NICE and the Royal College of Psychiatrists, should be used to reduce withdrawal symptoms.1,4,9 This involves reductions as a proportion of the previous dose (such as 25%); an example tapering plan is shown in Figure 1. Unfortunately, some doses will not be available in tablet form so liquid preparations should be used. These are routinely available for most SSRIs; however, in rural areas or for less common SSRIs, liquid preparations might need to be ordered in advance. To prevent withdrawal symptoms, tapering should take place over a long period of time, spanning months, or even years.1,9 SSRIs with shorter half-lives, such as paroxetine and venlafaxine, require a longer taper.
{kind=link}
Clinical scenario based on a patient taking 40 mg citalopram for 18 months, with their tapering plan involving 50% reductions to the previous dose, every 4 weeks. Adapted from Royal College of Psychiatrists.8
Should patients be advised to skip doses?
As most SSRIs have a half-life of around 24 hours, skipping doses creates large changes to drug levels, and so increases the risk and/or severity of withdrawal.7 Instead, patients should follow a hyperbolic tapering regime outlined above. Fluoxetine, however, has a longer half-life and therefore skipping doses remains an option, and is currently recommended by NICE.1,4
Further support and guidance
While creating a tapering regime, GPs should:
Discuss withdrawal and its symptoms with patients, while providing further resources, such as the Royal College of Psychiatrists online guidance.8 This empowers patients to recognise if they are experiencing withdrawal;
Outline pathways for patients to seek additional support. This could include scheduling a future telephone or in-person appointment to monitor their taper, discussing ways they can access urgent medical attention, and involving pharmacists and practice nurses. Pharmacists can play an important role in leading future appointments to monitor patients’ tapering regime, identifying potential withdrawal symptoms, and modifying tapering plans accordingly. Furthermore, by liaising between prescribers and patients, pharmacists can disseminate up-to-date information, promoting safe SSRI withdrawal;
Explain the importance of following the tapering plan and the potential issues of stopping abruptly or more quickly;
Advise patients that, if they believe they are experiencing withdrawal, to return to the last dose without symptoms and book a GP/pharmacist appointment; and
Acknowledge that stopping antidepressants can be daunting, while encouraging patients to involve their family, friends, and other healthcare providers for support.
How should GPs manage those who experience withdrawal symptoms?
Unfortunately, despite well-planned tapering regimes, some patients will still experience withdrawal. In these patients, tapering should be reduced (for example, changing 20% reductions to 10%) and longer periods introduced between dose changes. Positive coping strategies should be discussed, including exercise, mindfulness, and advice on good sleep hygiene.7 These patients will require ongoing support from either a GP or pharmacist to monitor their progress and allow for further alterations to their tapering regime. GPs should acknowledge how debilitating symptoms can be and give patients the opportunity to discuss their fears and concerns. Importantly, GPs should provide contact details of local crisis services and support patients in referring to psychological services.
CONCLUSION
For patients to be able to make an informed decision regarding their care, and provide valid consent for treatment, GPs must have open and up-to-date discussions around withdrawal syndrome. This, alongside proportionate, slow tapering plans, will reduce the number of patients on antidepressants and the number of patients experiencing withdrawal syndrome (Box 1).
|
Take-home messages
Notes
Funding
There was no funding source for this work.
Ethical approval
Not applicable.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received November 16, 2022.
- Revision requested December 2, 2022.
- Accepted December 14, 2022.
- © British Journal of General Practice 2023
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

